
Abstract
Objective:
To assess the management pathways of ureteric stones within our department and any impact on this as a result of the pandemic.
Patients and methods:
Retrospective data were collected at two different time points defined as ‘pre-COVID-19’, during April and May 2019, and ‘peri-COVID-19’, during April and May 2020 of all patients with ureteric stones.
Results:
Similar patient numbers presented with ureteric stones pre-COVID-19 (63) and during the pandemic (75). Pre-COVID-19, 31 patients were admitted, of which 48% had primary ureteroscopy (URS) or percutaneous nephrolithotomy (PCNL). The average time to theatre was 1.2 days. During the pandemic, there were 34 admissions with 56% of these patients receiving primary URS/PCNL. The average time to theatre was 1.5 days. Of the patients referred to the virtual stone clinic, pre-COVID-19, 38% were listed for urgent-elective surgery which was performed at an average of 62 days. During the pandemic, 49% were listed for surgery, waiting 144 days for their procedure.
Conclusion:
Patients who underwent primary surgery during their first admission had their definitive treatment quicker during the pandemic. However, patients listed for elective procedures waited longer in the peri-COVID-19 period.
Level of evidence:
(Oxford Centre for Evidence-Based Medicine: Levels of Evidence (March 2009)): 2c
Introduction
Ureteric colic is a common urological emergency, and kidney stone rates are increasing in prevalence throughout the world, 1 and therefore, their treatment contributes to a significant proportion of both the emergency and urgent caseload of a urologist. Obstructing ureteric stones can cause urosepsis or irreversible kidney damage if left untreated. Getting It Right First Time (GIRFT) recommends primary management of ureteric stones during an acute presentation with ureterorenoscopy (URS) or extra-corporeal shock-wave lithotripsy (ESWL). 2 Through early stone clearance, the need for repeat procedures or subsequent hospital admissions is reduced. Our department aims to perform early definitive management of ureteric stones; however, this is not common practice throughout the United Kingdom.
The COVID-19 pandemic introduced new surgical prioritisation measures to both elective and emergency operating in the United Kingdom. 3 Within these recommendations, obstructing ureteric stones, if associated with infection, should be treated within 24 hours, and if simple or associated with renal impairment or uncontrolled pain, within 72 hours. This which can include primary URS or insertion of a ureteric stent. They recommend that all patients should receive their definitive treatment of the stone within 1 month. 3
We wanted to establish whether the COVID-19 pandemic had affected our management of patients presenting with ureteric stones. Our aim was to assess how ureteric stones were treated and any impact on treatment as a result of the pandemic.
Methods
Data collection
Retrospective snapshot data were collected at two different time points defined as ‘pre-COVID-19’, during April and May 2019, and ‘peri-COVID-19’, during April and May 2020. During the ‘peri-COVID-19’ time period, there was a national lockdown in place in the United Kingdom, but mass testing had not yet been introduced. There were up to 18,974 patients admitted into hospital with COVID in the United Kingdom in April 2020, and therefore, non-urgent operating was postponed. 4 The audit was registered with our ‘Clinical Effectiveness and Audit’ office. Data extraction was performed by two investigators (C.L. and A.M.). Stone diagnosis was confirmed using a non-contrast computed tomography (CT) Kidneys Ureters Bladder scan (CT KUB). For each of the time periods, all patients identified as having a ureteric stone were collected from daily inpatient lists and the weekly virtual stone clinic lists. Extracted data included patient demographics, stone size and location, length of stay (LOS), waiting time before procedure, type of procedure, stone-free rate (SFR) and complications.
Patient pathway
All patients with an identified ureteric stone, in our department, follow the management pathway as shown in Figure 1. Patients are admitted acutely under urology if ureteric colic pain is uncontrolled, they show signs of infection or acute kidney injury (AKI). The aim is for definitive, primary stone management, which may be URS or percutaneous nephrolithotomy (PCNL). However, if clinical condition or complicating factors precludes this, the patient will be managed with a temporising procedure (ureteric stent or nephrostomy), requiring further intervention at a later date. Alternatively, if no admission criteria are met, the patient may be discharged with referral to the virtual stone clinic. If uncontrolled pain is the sole indication for admission and later settles, the patient may be discharged, with referral to the virtual stone clinic. Patients referred to the clinic are then reviewed by a dedicated endourologist within 1 week, and listed for an urgent-elective procedure (i.e. within 4 weeks) or, continue with conservative management.
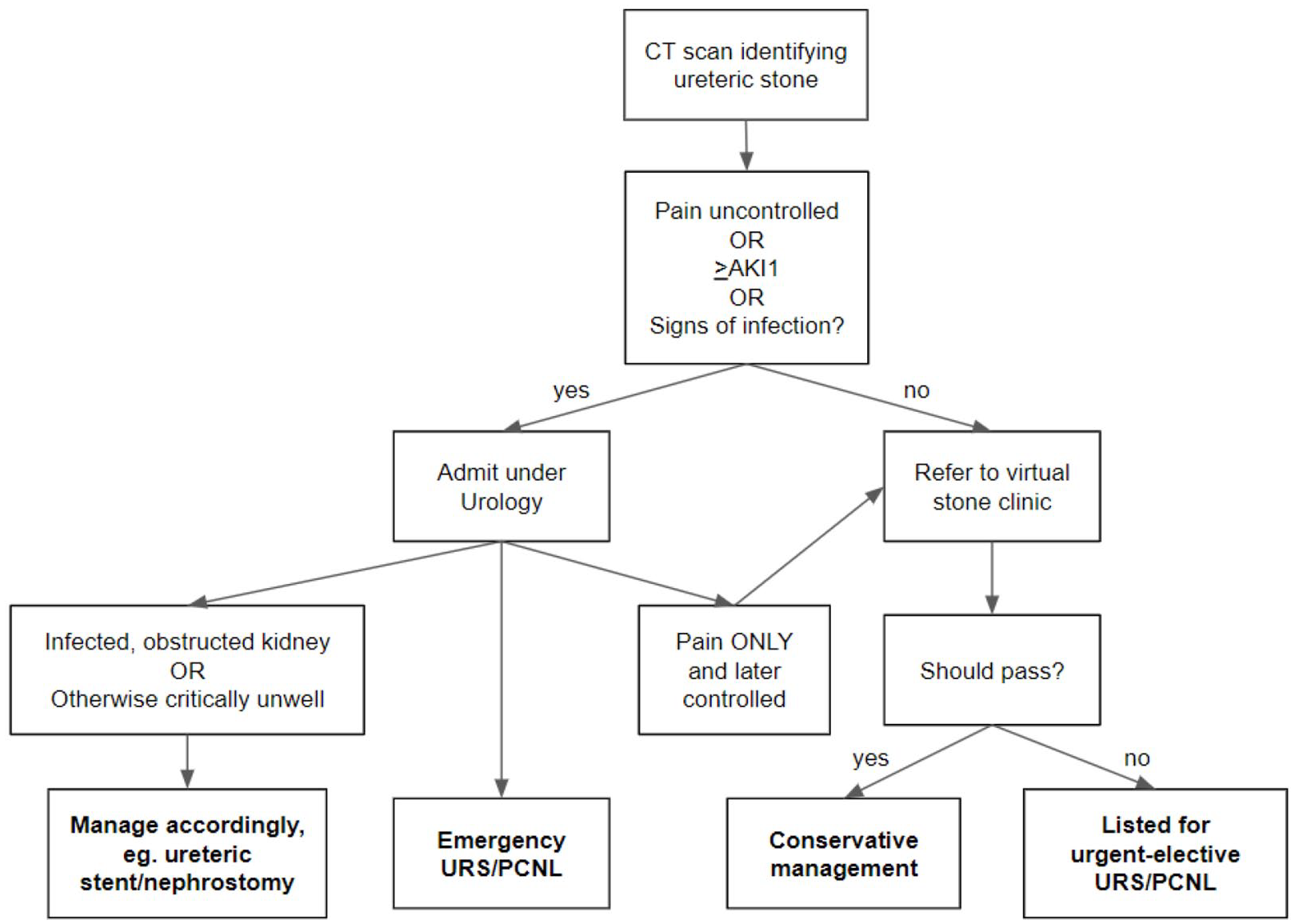
Flowchart demonstrating the management pathway in Eastbourne District General Hospital for patients with ureteric stones.
Outcomes
AKI is defined as a rise in creatinine of more than 50% from the patient’s baseline function. Stone size was calculated by measuring the maximum stone diameter on CT KUB scan or for multiple stones, a sum of maximal dimensions of each stone. SFR was determined intra-operatively with a combination of direct vision and fluoroscopy. If patients were managed with a temporising procedure, the reasons for this decision were included, factors such as AKI or infection. The wait time from admission to first procedure and from discharge following temporising procedure to definitive procedure were also compared.
Statistical methods
Data were recorded onto a Microsoft Excel spread sheet and descriptive statistics were used to report the data. Non-paired t-testing was performed using GraphPad (2022).
Results
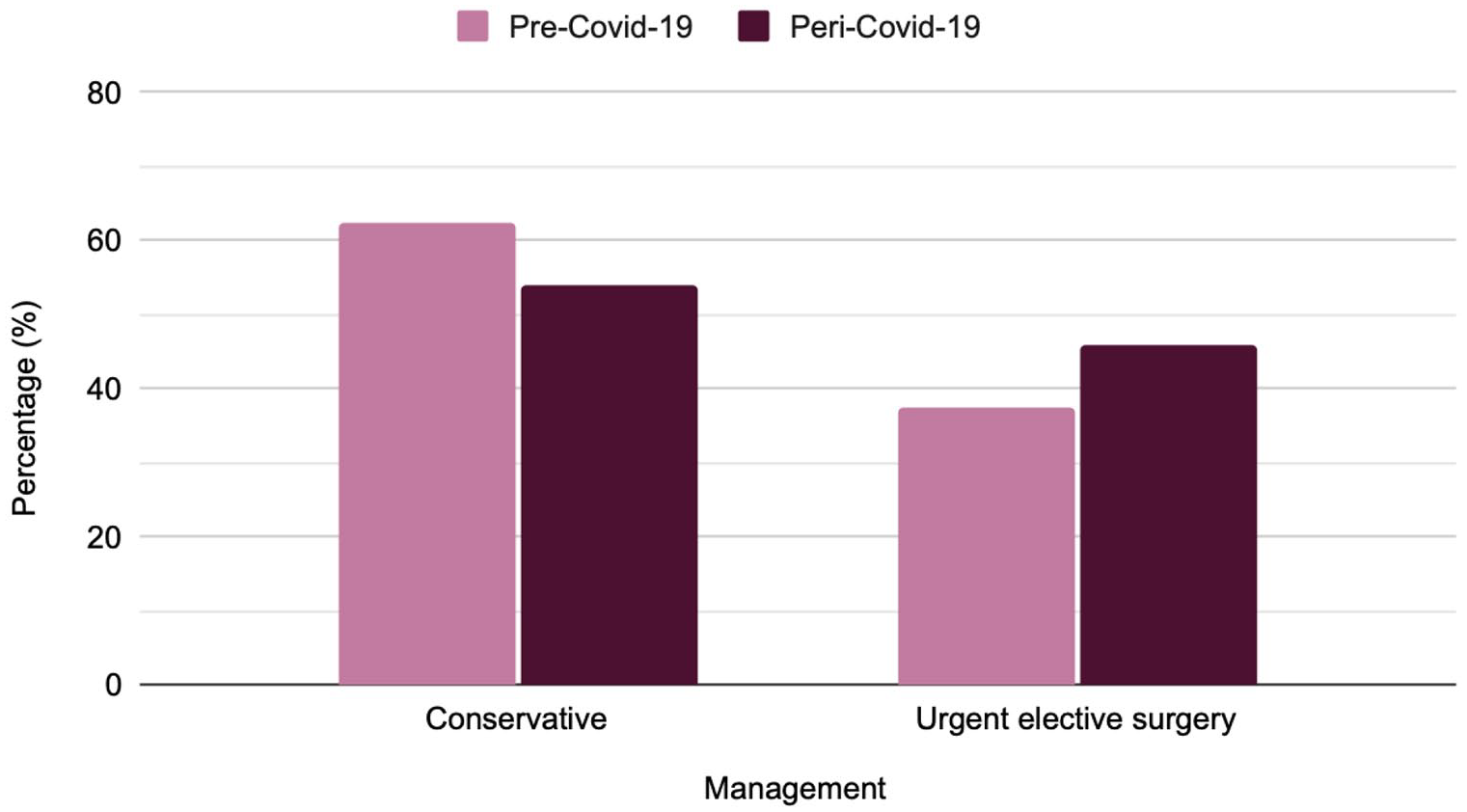
In our study period, there were 63 patients identified as having ureteric stones in the pre-COVID-19 group as shown in Table 1, and Figure 2 shows the management pathway of all patients. Thirty-one patients had an emergency admission, with an average total stone burden of 9.4 mm and an average LOS of 6.3 days. Of these, five patients (16.1%) were managed conservatively and 15 patients (48.4%) underwent URS or PCNL for definitive stone management during their acute admission. Eleven of these patients were managed directly with URS or PCNL, waiting an average of 1.2 days from admission to first procedure, and four patients underwent a temporising procedure initially, due to infection, before undergoing a definitive procedure later during the same admission. The total SFR of these patients was 86.7%. The remaining 11 patients of the emergency admissions group (35.5%) underwent temporising procedures alone, all due to infection, and were discharged for follow-up management, with an average wait time of 58 days until elective definitive procedure. There were 32 patients who were referred to the virtual stone clinic after identification of a ureteric stone in the pre-COVID-19 group. Twenty patients (62.5%), with an average total stone burden of 3.7 mm, were managed conservatively. Twelve patients (37.5%), with an average total stone burden of 7.4 mm, were booked for urgent-elective surgery and had an average wait time of 62.1 days. Those who underwent urgent-elective surgery had an average LOS of 0.1 days and an SFR of 100%. Three patients were admitted as an emergency following virtual stone clinic advice due to ureteric colic.
Clinical presentation data for patients with ureteric stones.
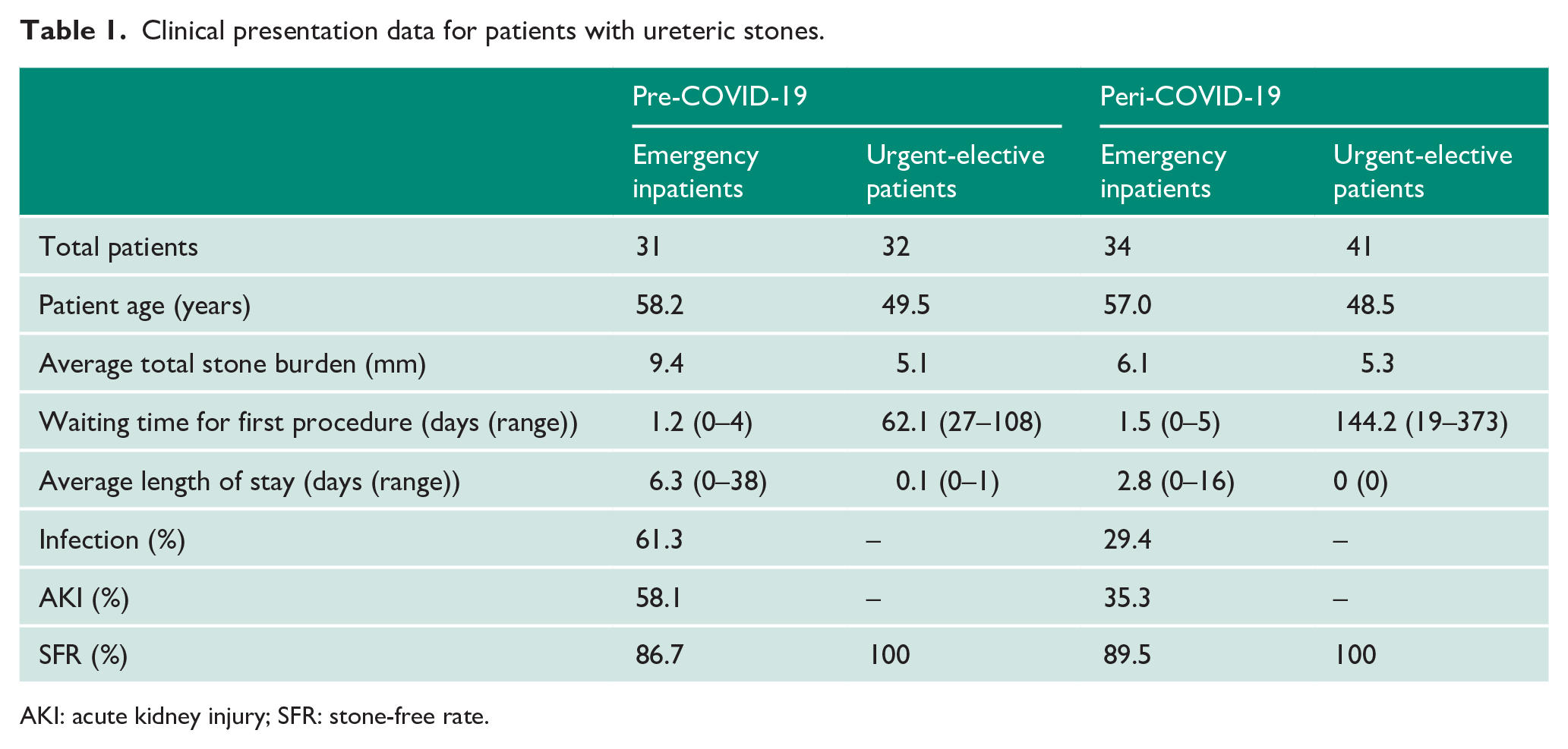
AKI: acute kidney injury; SFR: stone-free rate.
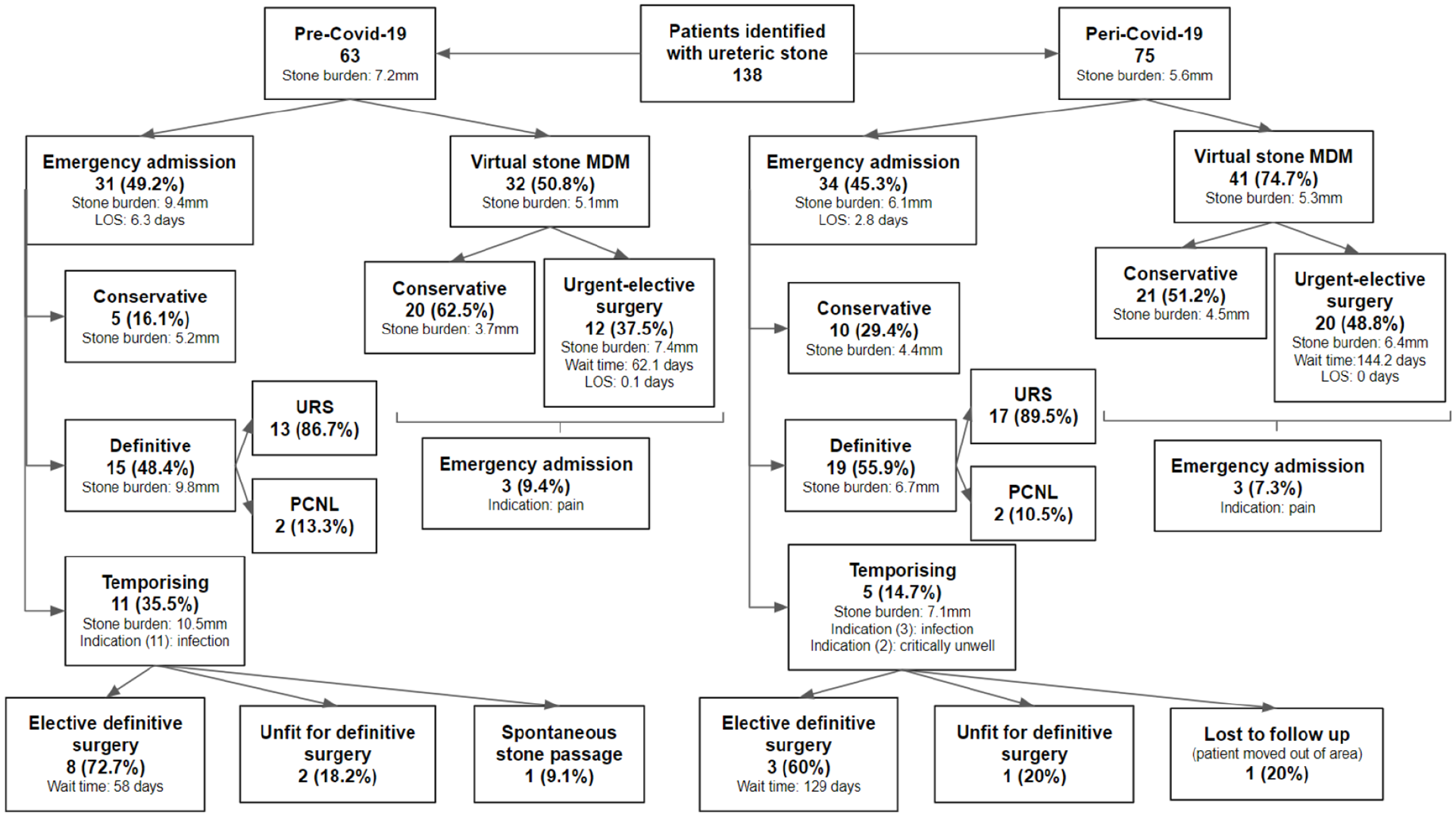
Flowchart demonstrating the management of all patients included in this review.
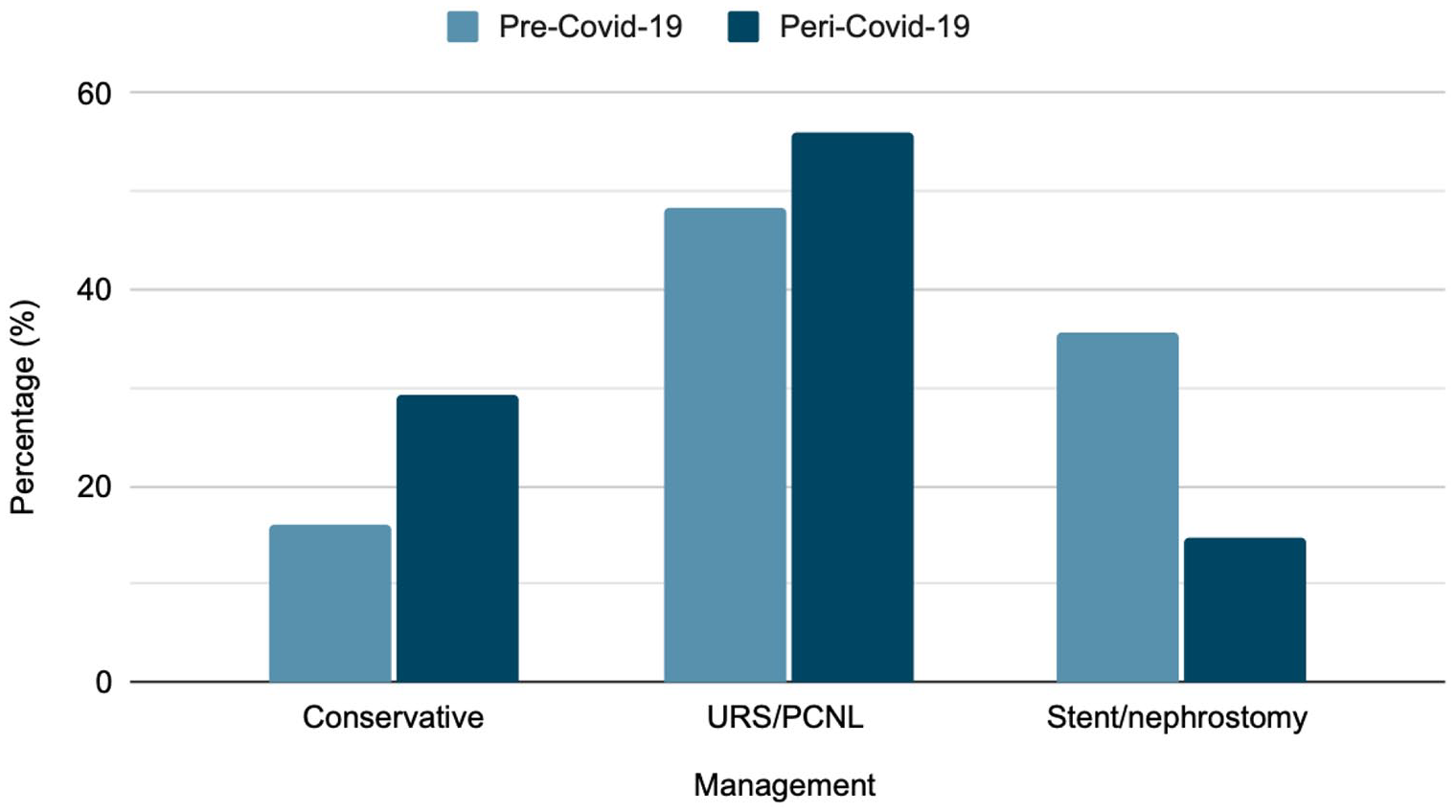
There were 75 patients identified as having ureteric stones peri-COVID-19, also shown in Table 1 and Figure 2. Thirty-four patients had emergency urology admissions, with an average total stone burden of 6.1 mm and an average LOS of 2.8 days. Ten patients of these (29.4%) were managed conservatively. Nineteen patients (55.9%) were managed directly with URS or PCNL, waiting on average 1.5 days for their first procedure, with an SFR of 89.5%. The remaining five patients (14.7%) underwent temporising procedures alone. For three patients, this was due to infection and two being critically unwell. The average wait time for follow-up elective definitive procedure was 129 days. There were 41 patients referred to the virtual stone clinic peri-COVID-19. Twenty-one patients (54%), with an average total stone burden of 4.5 mm, were treated conservatively. Twenty patients (46%), with an average total stone burden of 6.4 mm, were booked for urgent-elective surgery. The average wait time was 144.2 days, no patient stayed in hospital overnight and there was a SFR of 100%. Three patients were admitted as an emergency following virtual stone clinic advice due to ureteric colic. Comparison between the management of patients managed pre- and peri-COVID-19 is shown in Graphs 1 and 2.
Discussion
The COVID-19 pandemic has had a significant impact on the health-seeking behaviour of many people with avoidance of healthcare facilities despite serious and life-threatening conditions, such as stroke and heart disease,5–8 as well as reduced presentations with renal colic and other acute urological issues.5–10 Delayed presentation for renal colic was also evidenced by much higher creatinine level. 11 Our study however found that a 19% higher number of patients presented during the pandemic, which may be due to different health-seeking behaviours between populations, or the relatively fewer COVID-19 infection rates in our region compared to other areas of the United Kingdom and many European countries. 12 Alternatively, the higher numbers could be explained by the good weather in our region during this time period, as there is a proven correlation between warm weather and increased presentations of kidney stones. 13 It is reassuring that our patients continued to seek medical attention warranted by ureteric stones, and therefore reduced the risk of serious morbidity associated with untreated ureteric obstruction.
The pandemic led to the publication of surgical prioritisation guidance from the Royal College of Surgeons (RCS) and the British Association of Urological Surgeons (BAUS) 3 as shown in Table 2. This highlighted the importance of ureteric stones as a urological emergency or urgent condition. Ureteric obstruction associated with infection, or stones associated with uncontrolled pain or renal impairment, were listed in the highest priority groups, meaning intervention should be undertaken within 72 hours. It was also stipulated that uncomplicated ureteric stones should only be waiting up to 1 month before their definitive management. This is in contrast to certain low-risk urological cancer operations being permitted to be postponed for up to 3, or more than 3 months. The pandemic may have therefore in some ways improved the management of ureteric stones, due to a heightened alertness of the most efficient use of resources and more efficient patient management. 8 This COVID-19-specific guideline led to minimal change in our centre which follows an established primary management protocol for ureteric stones as shown in Figure 1. This is mostly in keeping with guidance as per BAUS, 14 NICE, 15 and EAU 16 though their recommendations are for URS or ESWL in the first instance for the treatment of stones. However, in our department, as the endourologists can perform their own access for PCNL, coordination with the interventional radiology department is not required. Patients can therefore undergo primary PCNL or the procedure can be converted to PCNL ‘on-table’ when required for patients with complex stone burden or if antegrade renal or ureteric access is needed.
Excerpt from the surgical prioritisation guidance published by the Royal College of Surgeons (RCS) and the British Association of Urological Surgeons (BAUS) for the COVID-19 pandemic. 3
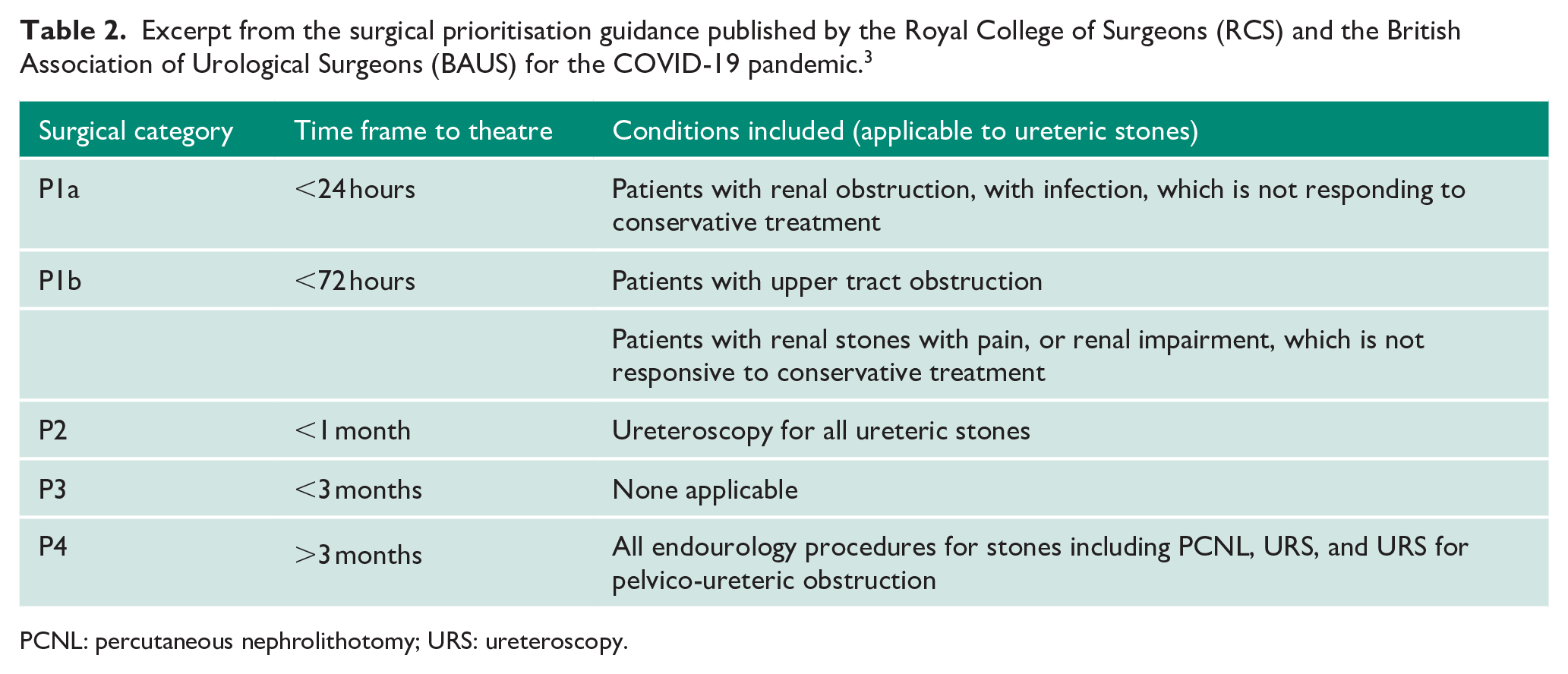
PCNL: percutaneous nephrolithotomy; URS: ureteroscopy.
During the study, a total of four patients underwent primary PCNL with potentially infected obstructed systems. This group included two patients from each of the study periods, pre-COVID-19 period (n = 2) and peri-COVID-19 (n = 2). This practice differs from current treatment guidelines due to the possible increased risk of postoperative sepsis. Our practice is to admit patients with renal colic and evidence of infection for temporising drainage or primary definitive management if infection has been controlled and the risk of post-operative sepsis mitigated. All of these patients had been treated for infection and observations had normalised. Other situational and patient factors were taken into account, including co-morbidities and competing risks of multiple procedures. Decisions regarding treatment options were discussed in a multi-disciplinary team environment. Definitive treatment was undertaken cautiously by experienced endourologists, with low irrigation pressure and the aim to change to simple drainage if there was evidence of frank pus or increasing concern about the risks of sepsis. Urine cultures were reviewed prior to theatre for all patients, and they had all been on antibiotics for at least 24 hours. None of these patients had any complications after their procedure.
Patients admitted for emergency management of their ureteric stones waited a similar time duration for their initial procedure (pre-COVID-19 = 1.2 days; peri-COVID-19 = 1.5 days; p = 0.43, CI: −0.94 to 0.40). This is thought to be because our department had already established dedicated CEPOD theatre sessions for urological emergencies, allowing for early definitive management.
The average LOS, however, did differ with pre-COVID-19 being more than double per-COVID-19 (6.3 days vs 2.8 days, respectively). Pre-pandemic patients were monitored to ensure resolution of any infective symptoms before intervention. During the pandemic, due to the cancellation of many elective cases, there was increased availability for emergency cases on the CEPOD operating list thus patients underwent intervention much quicker. Also, their LOS was minimised during the pandemic as it was likely due to an increased effort to reduce hospital inpatients and potential exposure to COVID-19, and increase bed availability. 17 This demonstrates that definitive management of acutely presenting ureteric stones can be managed fully within a matter of days alongside processes geared towards efficient patient discharge, in line with GIRFT recommendations.
Despite this, there was a marked increase in waiting time for patients who were referred for urgent-elective surgery from our virtual stone clinic with patients waiting 129 versus 28 days pre-pandemic. Those awaiting definitive stone treatment following an emergency admission with a temporising treatment had more than doubled (144.2 vs 62.1 days). While there is no clearly defined time period within which a ureteric stone should be removed if not passed spontaneously, it is generally agreed that the upper limit should be between 6 and 12 weeks.18,19 The delay likely reflects the additional complexities in arranging for elective hospital admission during a pandemic. The suspension of elective surgery during the pandemic has increased waiting list times 20 and will make time-dependent operating a challenge for health services going forward. An area for further review would be to assess whether patients who waited longer for their procedures came to any harm as a result. This could contribute to defining the time period within which ureteric stone procedures should be performed.
The SFRs in the elective patients was 100%; however, patients who had emergency procedures had lower rates at 88.2%. This is uncommon and there is good evidence that primary URS is as effective as a delayed procedure. 21
An alternate method for treating ureteric stones is ESWL, which is recommended as first-line treatment by BAUS 14 and NICE. 15 Experience gained from the COVID-19 pandemic has allowed for the development of local planning strategies in case of future epidemics, including the optimisation of theatre capacity, to ensure urgent and emergency caseload can continue with as little disruption as possible, and the addition of ESWL facilities for ureteric stones to increase treatment capacity.
There are limitations to our study, as our patient numbers are from a single-centre and are low volume. It has also been conducted retrospectively. Our data have been collated from all stone referrals to urology; however, there may be some cases managed solely in the emergency department who were not referred, and therefore missed.
Conclusion
Our study shows that patients who underwent primary surgery during their first emergency admission had their definitive treatment quicker during the COVID-19 pandemic. However, patients listed for elective procedures waited longer in the peri-COVID period.
Footnotes
Conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Contributorship
The study was conceived by S.M., background and literature research was by C.L. and L.W. Data were collected by C.L. and A.M. C.L. wrote the first draft, which was reviewed and edited by L.W. and S.M. Supervision and expert opinion was provided by S.M. and G.W. All authors reviewed and approved the final version of the manuscript.