
Abstract
Purpose:
To determine whether there is any effect of weather parameters on the incidence of renal colic patients presenting to emergency rooms (ERs) during the hottest season in Israel.
Materials and Methods:
This retrospective multicenter study involved all ER admissions related to renal colic in nine centres throughout Israel between 2010 and 2017. The collected data included the date of ER visits, the patients’ age and sex, and the weather features of ambient temperature, wind velocity, noon heat index, and barometric pressure. Multivariable logistic regression analyses identified predictors of increased ER visits for renal colic.
Results:
There were 85,501 renal colic-related ER visits during the study period, involving 62,935 (74%) males and 22,566 (26%) females (p < 0.005). The mean ± standard deviation (SD) age of the males and females was 50 ± 5.8 and 48 ± 19.6 years, respectively (p = 0.1). Most of the ER arrivals were in the 31- to 50-year-old age group (37%, 31,508) (p = 0.02). The maximal ambient temperature (odds ratio (OR) = 2.213, 95% confidence interval (CI) = 2.148–2.279, p < 0.0001), lower heat index (i.e. low humidity; OR = 0.880, 95% CI = 0.872–0.887, p < 0.0001) and increased wind velocity (OR = 1.165, 95% CI = 1.149–1.182, p < 0.0001) had a significant linear effect on ER visits for renal colic events.
Conclusion:
Conditions that increase sweat evaporation during the hottest months, including a decreased heat index and increased wind velocity, correlated with more ER visits for renal colic events, probably due to dehydration associated with elevated sweat evaporation.
Level of evidence:
Not applicable
Introduction
The etiology of kidney stones is multifactorial, and the rate of stone formation is reportedly affected by geographic and seasonal differences. 1 Many studies have reported on weather factors that influence the incidence of renal colic events.1–9 While the majority of those reports concentrated on the link between increased ambient temperatures and renal colic events, there have been mixed conclusions on the effect of other weather parameters.
Israeli weather during the warmer months of the year is relatively stable. Almost 60% of the country experiences hot and dry desert weather, while about 20% of the country, along the central Mediterranean coast, is hot and humid. Israelis are well prepared for the summer with over 90% of households and businesses fully air conditioned, as are all government buildings and all means of public transportation in accordance with mandatory building and traffic regulations. 10 We hypothesised that heat exposure would consequently be lessened and that the effects of outdoor weather on the occurrence of renal colic events would therefore be mitigated. The purpose of the current study was to investigate the complex interaction and the impact of various weather parameters on the regional rate of emergency room (ER) admissions related to renal colic during the warm season in Israel.
Materials and methods
Study design
Following institutional review board approval in all participating centres, we performed a retrospective, multicenter analysis of all ER visits for renal colic between 2010 and 2017. The records of patients who visited the ER were retrieved from the respective database of each hospital by means of the International Classification of Disease 10th Version codes ‘calculus of kidney’, ‘calculus of kidney with calculus of ureter’ and ‘renal colic’. By protocol each patient is given a code after being evaluated in the ER by a physician following an imaging study (non-contrast computerised tomography or ultrasonography), blood workup and urinalysis. The following data for each ER visit were collected: age, sex and date of visit.
The hospitals taking part in the study were selected from three distinct Israeli regions: northern, central and eastern regions. These were specifically chosen due to the large cities surrounding these centres, providing medical services to the surrounding communities as well as the climatic differences between the three regions.
With the assistance of the Israeli meteorological service, weather data were gathered from three highly populated regions in Israel: Northern Israel, Central Israel (the coastal plain) and Eastern Israel. The following meteorological data were collected for each day: maximum ambient temperature, noon heat index, mean sea level barometric pressure, wind velocity and precipitation. Ambient heat index at noon was expressed in terms of ‘apparent temperature’ (AT), an index which combines temperature and humidity 11 and it was calculated by means of the heat stress equation. 12 The seasons were defined according to meteorological definitions according to calendar months: spring (1 March–31 May), summer (1 June–31 August), fall (1 September–30 November) and winter (1 December–28 or 29 February).
Statistical analysis
Descriptive analyses (mean with standard deviation (SD)) were applied for continuous variables, proportions for discrete variables and comparative tests that included the chi-square test for discrete variables and the Kruskal–Wallis test for continuous variables. Multivariable logistic regression analyses were performed to identify factors predicting ER visits for renal colic during the summer months. A priori covariates included age, sex, geographical region, season, maximum ambient temperature, heat index, wind speed and precipitation. Goodness of fit was assessed with the Lemeshow and Hosmer method. The statistical tests were two-tailed and a p-value <0.05 was considered statistically significant. All analyses were conducted with SPSS software version 23.0 (SPSS Inc., Chicago, IL).
Results
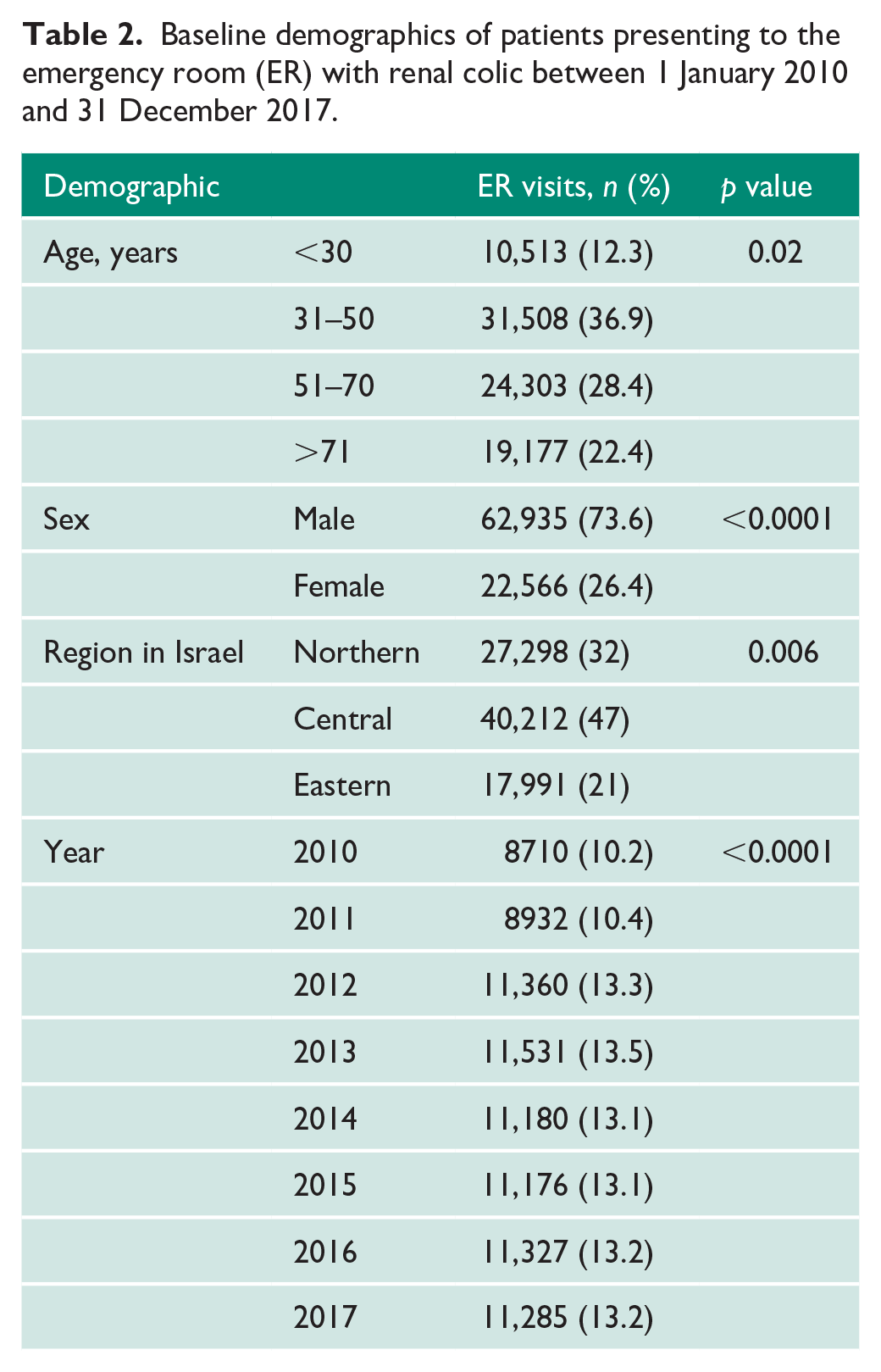
Seasonal and regional differences of various weather parameters are presented in Table 1. Between 1 January 2010 and 31 December 2017, there were 85,501 ER visits in 10 hospitals in Israel for renal colic events. Males represented 74% (62,935) of the total ER visits, while 26% (22,566) were females (p < 0.005). The 31- to 50-year age group (37%, 31,508) was the most commonly affected among both males and females (p = 0.02) (Table 2). The gender distribution at this age group was 77% (24,537) males and 23% (7097) females (p < 0.005). The percentage of ER referrals for renal colic in the Central, Northern and Eastern regions was 47% (n = 40,212), 32% (n = 27,298) and 21% (n = 17,991), respectively (p < 0.005) (Table 2). Most of the visits to the ER for renal colic occurred during the summer months (28 %(n = 24,365), p = 0.04) (Table 1 and Graph 1).
Emergency room visits and average meteorological seasonal changes in three regions in Israel between 2010 and 2017.
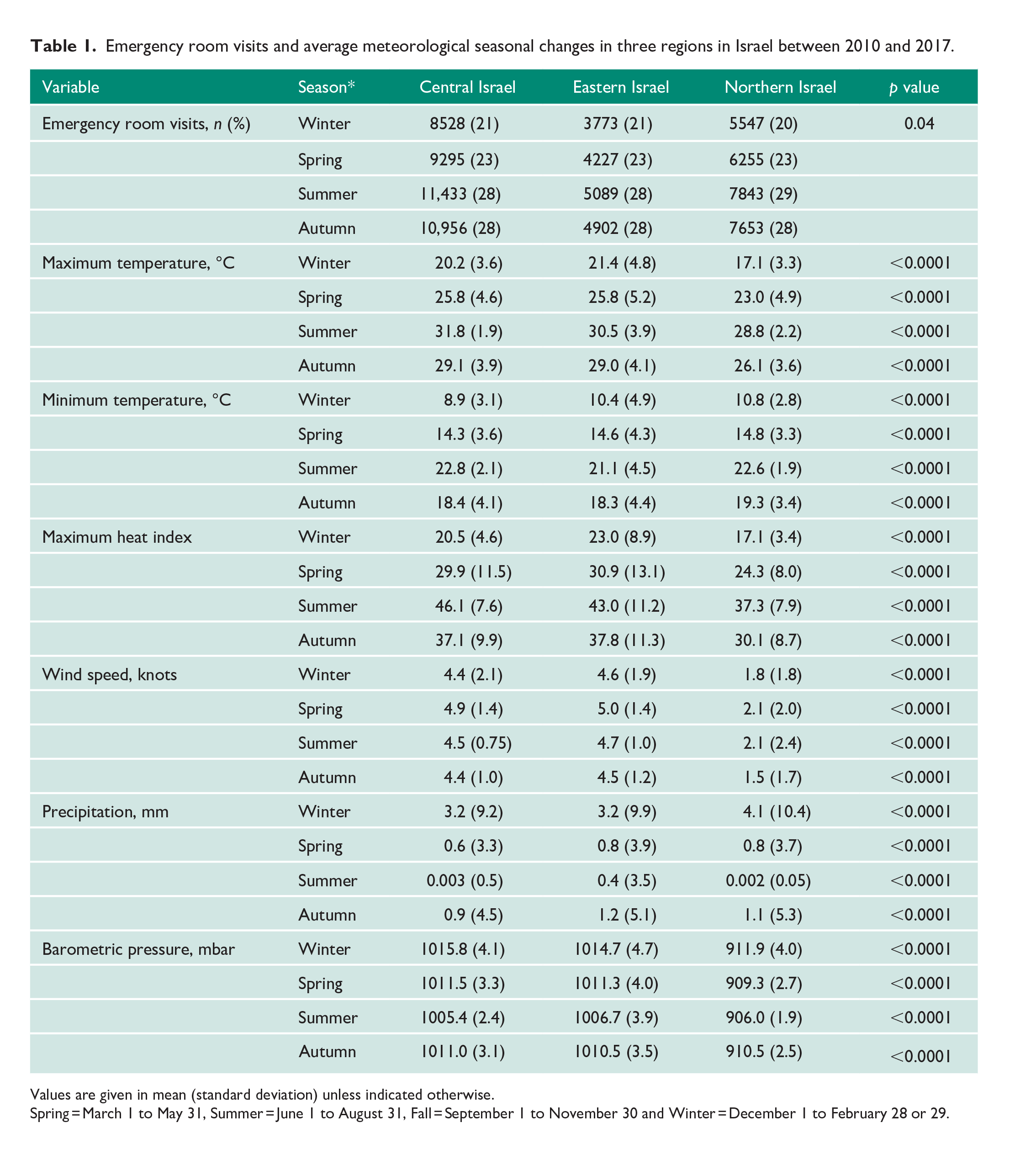
Values are given in mean (standard deviation) unless indicated otherwise.
Spring = March 1 to May 31, Summer = June 1 to August 31, Fall = September 1 to November 30 and Winter = December 1 to February 28 or 29.
Baseline demographics of patients presenting to the emergency room (ER) with renal colic between 1 January 2010 and 31 December 2017.
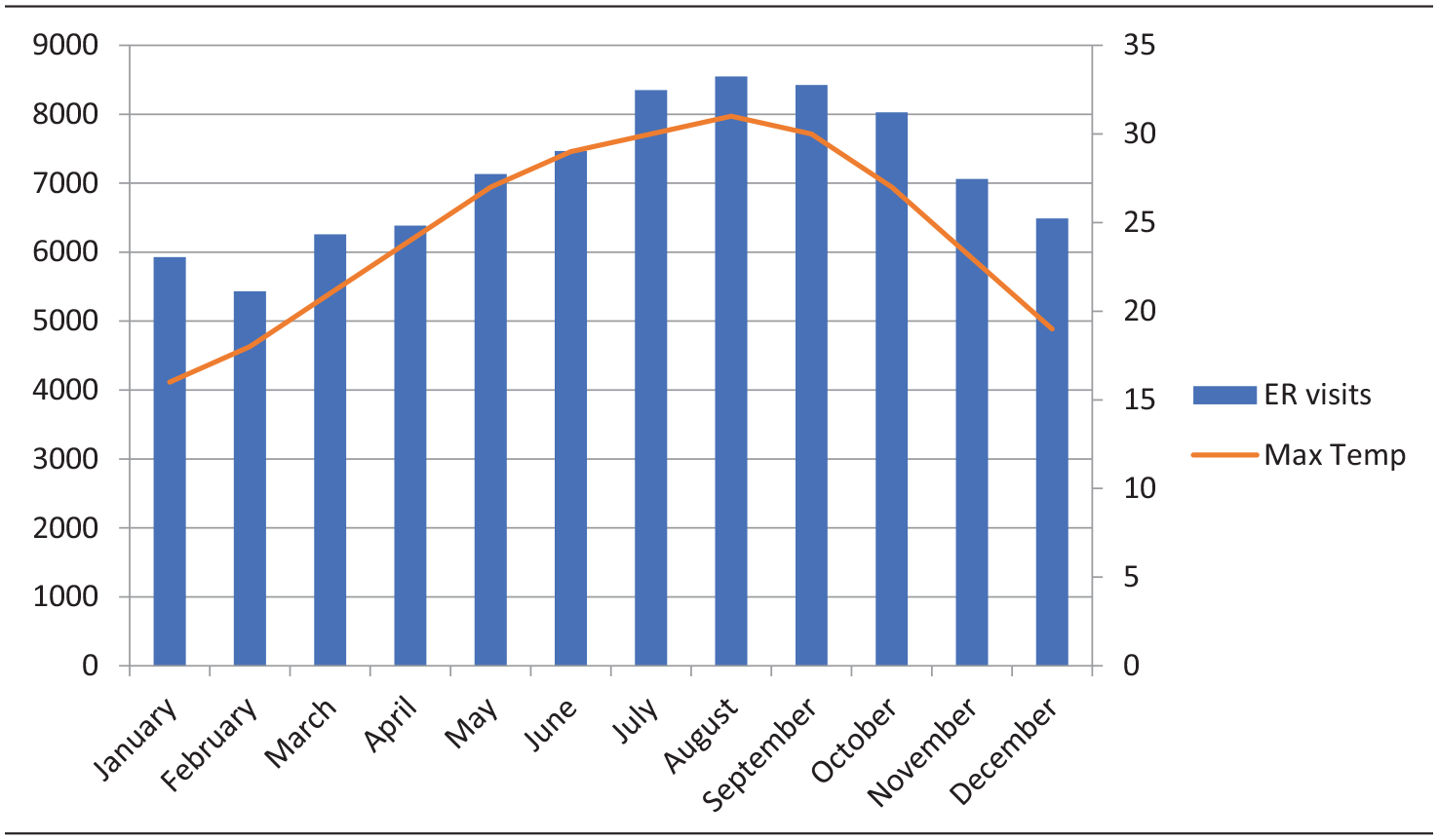
ER visits and mean maximum monthly temperatures between 2010 and 2017.
A multivariable logistic regression model for analysing predictors of patients presenting to the ER for renal colic during the summer months demonstrated that there was a 6.9% (odds ratio (OR) = 1.069, 95% confidence interval (CI) = 1.059–1.079, p < 0.0001) increase in ER referrals for each year (2010–2017). Furthermore, a high ambient temperature (OR = 2.213, 95% CI = 2.148–2.279, p < 0.001), a lower AT index (OR = 0.880, 95% CI = 0.872–0.887, p < 0.001) and increased wind velocity (OR = 1.165, 95% CI = 1.149–1.182, p < 0.0001) were independently associated with an increased risk of renal colic (Table 3). An analysis of the winter months revealed a small yearly decrease in the incidence of renal colic (OR = 0.927, 95% CI = 0).
Multivariable logistic regression models predicting emergency room visits for renal colic during the summer months (June–August) 2010–2017.
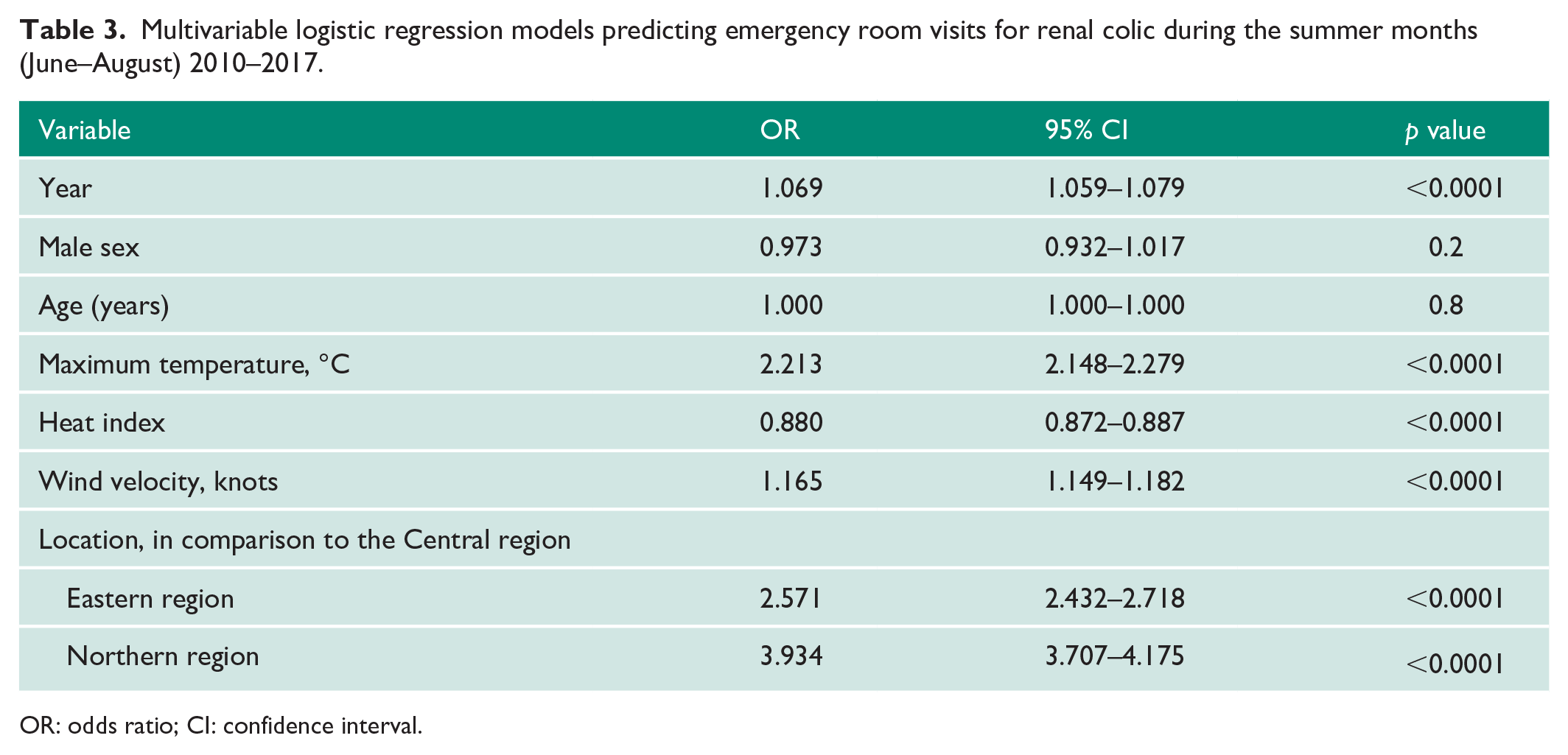
OR: odds ratio; CI: confidence interval.
Discussion
An increase in temperature is commonly believed to increase the rate of renal colic events. However, if the baseline temperature is high, as are the condition in Israel during the summertime, do fluctuations of temperature still have an effect? The current study shows that even in the hot summertime and despite air-condition utilised in most places, elevated ambient temperature increases are still associated with an increased rate of renal colic events. Interestingly, we observed a yearly increase of 6.9% ER visits for renal colic during the summer months, and a parallel decrease during the winter months. Other weather parameters were also associated with the rate of renal colic events. An increase in wind velocity was associated with a rise in ER visits for renal colic. For every one-point increase in the heat index during the summer season, the risk of renal colic decreased by 11.2%. This would seem paradoxical, but we hypothesise that with an elevated heat index, there is less evaporation whereupon dehydration actually decreases. A study by Greenleaf and Sargent 13 found that gross sweat loss correlated with increased mean water intake. Contrarily, as the heat index decreases but the ambient temperature remains elevated, the human body still evaporates fluids but perspires less, leading the person to be unaware of the fluid loss and therefore leading to decreased consumption of fluids, resulting in dehydration. This association is further highlighted by the differences seen between the three geographic regions evaluated in the current study. The mean heat index in the Central shoreline area of Israel was significantly higher compared to the indices of the northern and eastern regions. The multivariable logistic regression for predicting presentation to the ER during the summer months demonstrated that people in the drier Northern (OR = 3.934, 95% CI = 3.707–4.175, p < 0.0001) and Eastern regions of Israel (OR = 2.571, 95% CI = 2.432–2.718, p < 0.0001) are more likely to present to the ER with renal colic compared to people in the more humid Central region. Supporting the idea of increased evaporation as the driving force behind increasing renal colic events is our finding that increased wind velocity is an independent predictor for renal colic events.
Mixed results have been published on the effects of humidity. While some studies reported on a correlation between elevated relative humidity and renal colic,7,8,14 other studies reported the opposite.4,15 In our study, we elected to investigate the heat index rather than relative humidity. The higher the heat index, the hotter the weather is perceived, since sweat does not readily evaporate and cool the skin. 11 When the relative humidity is high, the rate of perspiration from the body decreases, leading the body temperature to increase. On the contrary, when the relative humidity decreases, the rate of perspiration increases. The heat index increases as the ambient temperature and relative humidity increase. We hypothesise that as wind velocity increases, the patient may be unaware of sweat evaporation and fluid loss, which might lead to dehydration and subsequently increased renal colic events.
While dehydration seems to be the major mechanism by which weather conditions impact the rate of renal colic, the sequence of events leading to the passage of a stone into the ureter is unclear. Lag times between elevated temperatures and an increase in renal colic events varied in several trials, ranging from 0 to 93 days.2,4,8,9,15–18 We hypothesise that the weather has a short- and long-term impact on the incidence of renal colic. Long-term dehydration is clearly associated with an increased risk of new stone formation and, subsequently, an increased risk of renal colic given enough time for stone formation. However, there appears to be a yet unknown mechanism by which acute, short-term dehydration is associated with an increased risk that an existing asymptomatic renal stone will migrate into the ureter. It is possible that local body movements are more directly transmitted to the collecting system when no urine is present to buffer them and that they may dislodge an existing stone.
In Israel, approximately 21% of the population are Muslims. The majority of these fast during the Ramadan period. Sagy et al. 19 reported on a significant association between renal colic events and fasting Muslims during the holy month of Ramadan. This, in our view, further emphasises the strong coloration between dehydration and renal colic events. Unfortunately, in the data collected during this study, we were not able to assess whether patients fasted during the holy month of Ramadan and comment on its effect on ER visits due to renal colic.
The main limitation is the retrospective nature of the study with its inherent selection bias. Second is the limited descriptive data on the characteristics of the patients admitted to the ER, mainly history of urolithiasis and comorbidities. Third, we did not have information on patient fluid intake, urine output, patient occupation and socio-economic status. Finally, the data on ER visits due to renal colic as well as the weather data are from specific demographic areas of Israel and may not represent the country as a whole. However, we believe that the large number of patients from several distinct geographical regions provide valuable data to verify that conditions that increase sweat evaporation during the hottest months, i.e. a decreased heat index and an increased wind velocity, correlate with renal colic events.
Conclusion
It is apparent that weather is significantly associated not only with the formation of renal calculi but also with the incidence of renal colic. Weather factors other than temperature such as heat index and wind velocity are also associated with renal colic incidence. Despite the common use of air-condition during the summertime, elevated temperatures increase the rate of renal colic events by an unknown mechanism. Further investigation of this phenomenon is important in view of global warming.
Footnotes
Conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by Rabin Medical Center ethics committee, approval number given by ethical board – RMC-0438-17.
Guarantor
D.G.
Contributorship
D.G. wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.