
Abstract
Background:
While ureteric stent removal remains a frequently performed endourological procedure stent migration either proximally or distally can present the endourologist with a significant intraoperative dilemma. In cases where the stent is of large calibre or impacted into the mucosa of the ureter, retrieval may prove refractory to traditional approaches.
Objective:
To present a further novel procedure: The Whiston Snare Technique for Loop Extraction of Stents (WHISTLES) which allows for intraureteric assembly of a tightening loop through a ureteric catheter thus permitting safe retrieval of a migrated stent.
Methods:
We describe the procedure as it was performed and have recreated the steps in a laboratory environment. This demonstrates an adaptation of existing materials readily found in most urological theatres and is not a prototypical device.
Results:
The procedure was successfully performed to allow extraction of the migrated ureteric stent.
Conclusion:
WHISTLES is a reproducible method for the retrieval of migrated ureteric stents where traditional techniques have failed.
Level of evidence:
5
Introduction
Ureteric stent insertion is a common endourological procedure.1,2 Stents are used to relieve intrinsic or extrinsic obstruction, in ureteric identification during abdominal procedures, 3 following stone surgery 4 and renal transplantation. 5 Complications include trigonal irritation, haematuria, sepsis, encrustation and migration.2,6–9 The implications of the ‘forgotten stent’ are documented in the literature. 10 Inadvertent placement during stone surgery has been reported. 11
One desired feature for ureteric stents is that they are easy to remove. 12 A pain-free method of ureteric stent removal with minimal or no anaesthetic is ideal. 2 Migration, although uncommon, happens both proximally and distally: 13 between 2% and 4.8% of all ureteric stents migrate proximally.14,15 It is thought to happen when the stent is too short for the ureter.14,16 Retrieval of a proximally migrated ureteric stent is an essential skill for an endourologist.
Methods for ureteroscopic removal of ureteric stents include forceps extraction, ureteric dilators and baskets.8,15,17,18 Fogarty catheter insertion and inflation in the lumen of the stent to allow for traction is also described. 19 Snare techniques are used in the percutaneous, antegrade removal of ureteric stents by using a goose neck snare. 13
Ureteroscopic instruments may not have enough purchase to provide satisfactory traction for removal of larger calibre migrated stents. Bagley and Huffman 15 demonstrated that a three-prong grasper did not have sufficient grip to capture stents larger than 4.8CH/Fr. When the lumen of the stent is embedded in the ureteric wall or surrounded by inflamed ureteric mucosa, there may not be a surface with a small enough diameter to grasp. 15 Equally, in this situation, traditional snares will not be able to successfully loop around the stent due to no free distal end.
Having encountered this problem intraoperatively, we devised a new technique of stent removal with a loop: The WHISTLES Technique. This procedure demonstrates a safe way of creating an intraureteric loop for retrograde removal of migrated stents which have proven difficult with standard extraction techniques. We used and modified existing materials which are routinely found in the urological armamentarium.
Technique
A 56-year-old female with cervical malignancy had been managed with bilateral long term 8.5CH/Fr 24 cm Gyrus ACMI double pigtail stents for extrinsic ureteric compression. She attended for routine stent exchange with antibiotic cover. Rigid cystoscopy revealed both distal ends of the stents curled in the bladder. A 0.035 in × 150 cm sensor guidewire was placed with X-ray guidance to the left renal pelvis alongside the stent. The original stent was removed and replaced with a 8.5CH/Fr 24 cm stent. When advancing the stent into the left ureteric orifice the distal end was lost.
A 6.4CH/Fr Semi-Rigid ureteroscopic retrieval was attempted with a zero-tip basket and ureteric biopsy forceps. The stent was too large in diameter to grasp with the distal end buried in the mucosal lining of the left ureter. We assembled a snare intraureterically under ureteroscopic and fluoroscopic control to enclose the stent inside a loop to overcome the lack of a free distal end. This successfully allowed us to (a) retrieve the impacted left stent and (b) exchange it with another 8.5 CH/Fr 24 cm ureteric stent. The right side was exchanged without incident. We did not take the patients consent for intraoperative photography, so we have recreated the steps in the following (Figure 1).
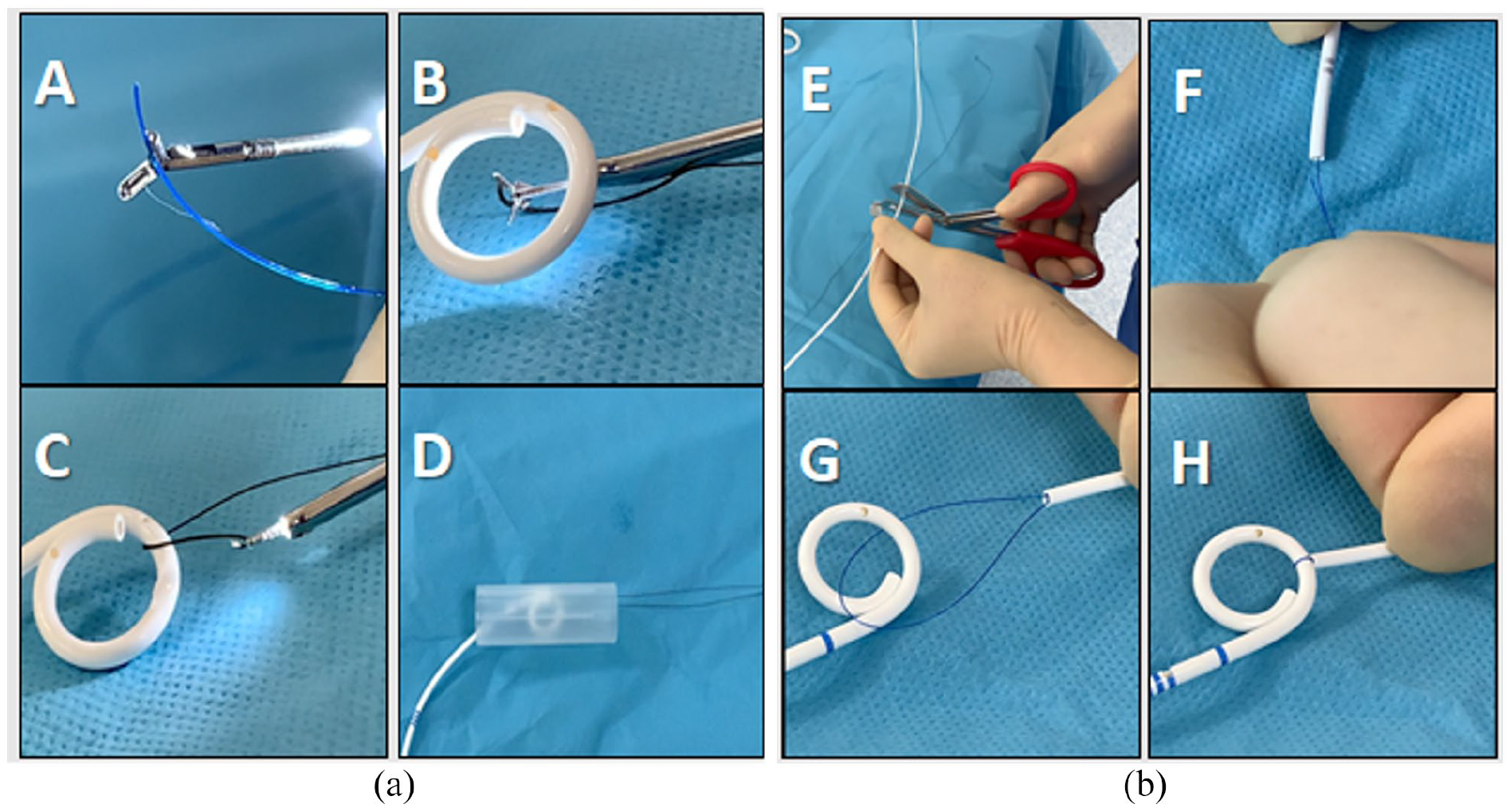
(a) Demonstration of steps A–D. (b) Demonstration of steps E–H.
A 6.4CH/Fr semi-rigid Olympus ureteroscope with ureteroscopic biopsy forceps were used. A long Prolene 1 suture, with the needle removed was placed up to the level of the stent via the biopsy forceps held at the end of the scope (A). The suture was placed on one side of the obstructed stent (B), released from the forceps and the ureteroscope manoeuvred to the other side of the stent which allowed the same end of suture to be grasped with the forceps. This created a loop with the stent in the middle (C).
The ureteroscope was then completely withdrawn from the ureter and bladder under vision with one end of the suture still enclosed within the forceps. This permitted both ends of the suture to protrude through the urethral meatus (D).
Using a 6CH/Fr Boston Scientific open-ended ureteric access catheter with the distal 10 cm cut off (E), both ends of suture were threaded into the lumen (F). The catheter was slid along the thread until pushed against the stent under fluoroscopy (G), creating a capture noose (H). By keeping sufficient tension on both the ureteric catheter and suture, this facilitated removal of the impacted stent distally through the left ureteric orifice.
Discussion
Multiple innovative endourological techniques have been described to facilitate easier access to the bladder, ureter and kidney in cases of unfavourable anatomy, surgically reconstructed urinary reservoirs or in unexpected intraoperative situations.20–24
Khan et al. 25 have described a ‘Lasso’ technique using 0 silk suture. This differs from WHISTLES as it (a) does not require the use of an access catheter and uses silk rather than Prolene sutures. In addition, (b) the procedure relies on the traction of the silk suture alone to remove the migrated stent unlike our technique which by (c) using the access catheter has an in-built tightening mechanism of the Prolene suture around the stent. In addition, our method demonstrates a way of achieving the same outcome without the risk of losing vision when removing the ureteroscope from the ureter, which is reassuring when faced with unexpected intraoperative events like stent migration.
Fischer et al. 8 have described a technique to reposition a migrated ureteric stent using a cystoscopically inserted guide wire passed through the stent into the renal pelvis and then manipulated to permit antegrade passage down the ureter, grasped in the bladder and following clamping at the external meatus was repositioned.
A similar method of providing tension has been described when trying to straighten a guidewire during flexible cystoscopic ureteric stenting. Here, the authors used a shortened 16CH/Fr ureteric dilator to encase and straighten the guidewire. This method differs to our technique in that the ureteric dilator does not enter the ureter. 26
Conclusion
Migrated ureteric stents are challenging to retrieve. We present a novel method of creating an intraureteric loop, which can be tightened around a stent, thus permitting safe retrieval of large-calibre impacted ureteric stents. This demonstrates an adaptation of existing materials, and as such is not a novel medical device. We believe WHISTLES to be an easily reproducible procedure using equipment that is readily available in most endourology units.
Footnotes
Conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.
Guarantor
A.S.
Contributorship
TPNH wrote the initial draft of the paper, performed the literature search and obtained photography. MSF edited the document at all stages, coined the ‘WHISTLES name’, assisted with the literature review and approved the final manuscript. AS developed the technique and identified it as being important for adding to the urological literature, performed the procedure for photography and approved the final manuscript.