
Abstract
We report five cases of middle-aged men with low testosterone levels and erectile dysfunction (ED) who were successfully treated with varicocelectomy with long-term follow-up. All five patients presented to our clinic with ED. Upon initial physical examination, each patient had varicoceles on his scrotum, and two consecutive morning samplings showed testosterone levels below 400 ng/mL. Age at varicocelectomy was from 40 to 53 years. Four patients underwent microscopic subinguinal varicocelectomy, whereas one patient underwent inguinal varicocelectomy. After surgery, testosterone increased in all cases, and the normal testosterone level was maintained during follow-up (16–60 months). In addition, all cases reported improvement of ED after surgery. In our clinical cases, microscopic varicocelectomy increased serum testosterone levels and improved erectile function, and this increase and improvement continued up to a follow-up of 60 months. Varicocelectomy would be a good option to treat testosterone deficiency in men with varicocele.
Introduction
Low serum testosterone levels in men are associated with erectile dysfunction (ED), decreased libido, decreased lean muscle mass, cardiovascular diseases, diabetes, and osteoporosis. 1 Several reports have proven the beneficial effects of testosterone replacement on muscle strength, osteoporosis, and anaemia, as well as sexual function in men with low serum testosterone. 1 Recently, it was reported that varicocele repair improves serum testosterone levels in older men (aged 40 or more) who have both varicocele and low testosterone levels during a mean 6.8-month follow-up, 2 whereas limited information regarding long-term efficacy is currently available. We report five cases of middle-aged men with low testosterone levels and ED who were successfully treated with varicocelectomy with long-term follow-up.
Case reports
This study was approved by the institutional review board (IRB number: 11100176-202104-HR-004). From March 2012 to December 2019, a total of 41 middle-aged men underwent microsurgical varicocelectomy by one urologist (J.H.L.). From among them, we included five men who were followed up for at least 12 months after the surgery in this study.
All five patients presented to our clinic with ED. Upon initial physical examination, each patient had varicoceles on his scrotum, and two consecutive morning samplings showed testosterone levels below 400 ng/mL. 2 Medications – such as testosterone replacement or clomiphene citrate, or surgical repair of the varicocele – were recommended, and all five patients chose the surgical option.
Table 1 shows the patients’ characteristics. Age at varicocelectomy was from 40 to 53 years. Cases 1 and 2 were obese, and Case 5 was overweight according to the Korean body mass index classification. 3 All had left Grade 1–3 varicoceles, and Case 2 had a testicular size discrepancy (testicular size difference of at least 4 mL). Four patients underwent microscopic subinguinal varicocelectomy, whereas one patient (Case 3) underwent inguinal varicocelectomy due to tight and low external rings. All surgeries were successfully done without any complication. After surgery, testosterone increased in all cases, and the normal testosterone level was maintained during follow-up (16–60 months). In addition, all cases reported improvement of ED after surgery (Figure 1). No complications, such as hydrocele or atrophy of the testicle, were found. In terms of testicular size discrepancy in Case 2, the testicle size did not return to normal upon physical examination at the last visit.
Patient Characteristics.
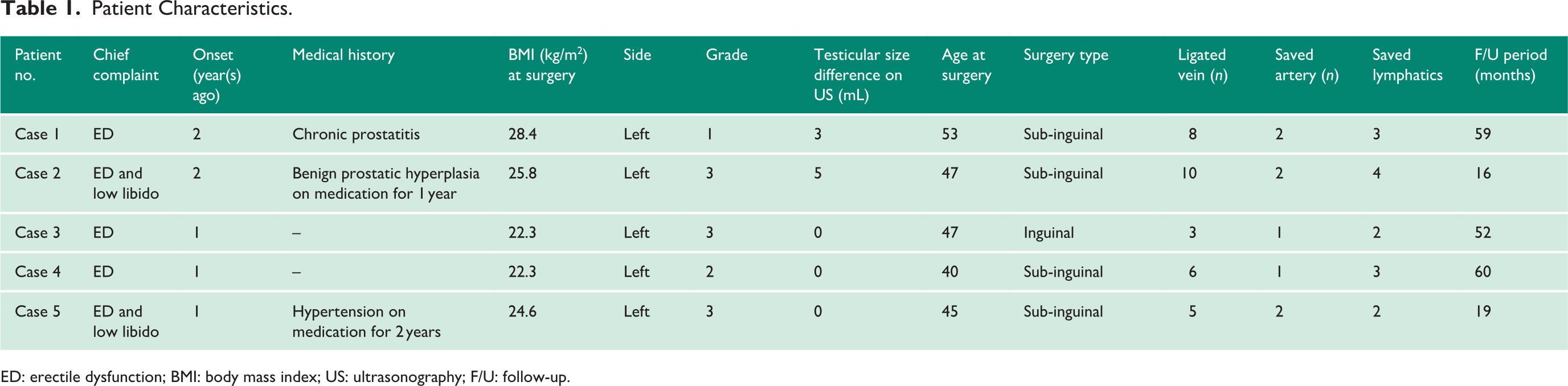
ED: erectile dysfunction; BMI: body mass index; US: ultrasonography; F/U: follow-up.
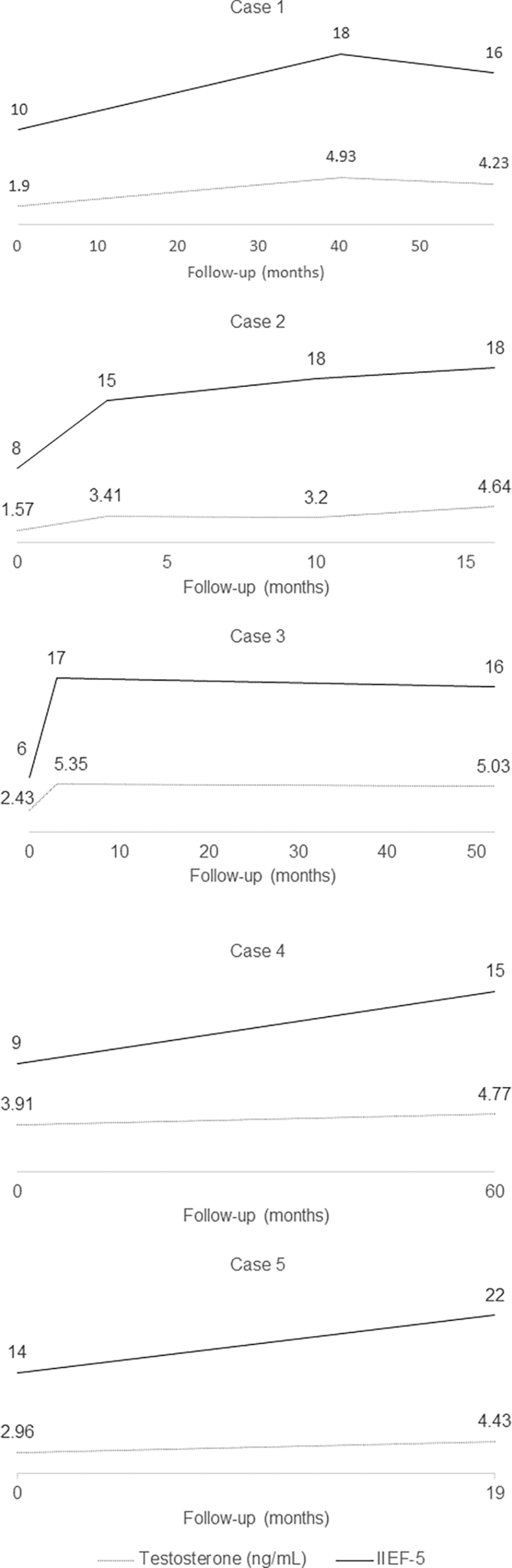
Changes in testosterone and IIEF-5 score after varicocelectomy.
Discussion
Varicocele might result in dysfunction of Leydig cells and subsequently lead to decreased testosterone production. In testis biopsy of patients with idiopathic varicocele, a decreased tubular diameter, cytoplasmic vacuolization in Leydig cells and atrophy have been found, and these results support the previous theory. 4 The exact mechanism by which varicoceles cause dysfunction of Leydig cells is unclear. However, alterations in the testicular thermal environment due to defects in a countercurrent heat exchange mechanism to cool the arterial blood are one possible explanation. 5 In addition, oxidative stress and related damage to Leydig cell mitochondria can be the other underlying mechanisms. 6 It has been suggested that in infertile men with varicocele and a subsequent decrease in serum testosterone, microsurgical varicocelectomy significantly increases the serum testosterone level. 7 In addition, it has been reported that surgical repair of varicoceles is also effective in increasing testosterone, even in the old-age group (40s or more), during a mean follow-up of 6.8 months. 2
To the best of our knowledge, there are no data regarding the long-term efficacy of varicocelectomy in middle-aged men. Our data showed that after surgery, testosterone increased in all cases and that a normal testosterone level was maintained during long-term follow-up (16–60 months). Microsurgical varicocelectomy might be a minimally invasive surgery and relatively safe surgery when performed by an experienced andrologist. In addition, in contrast with androgen replacement therapy, one-time surgery might provide a long-term ‘fix’ in hypogonadal men. 8 Therefore, we believe that our data suggest that microscopic varicocelectomy could be offered to men with both varicocele and testosterone deficiency (TD) as an alternative to testosterone replacement. 8
In terms of the relationship between ED and varicocele, scant data are available. In a population-based study, the odds ratio of ED for the untreated varicocele group was higher than the odds ratio of ED for the treated varicocele group (odds ratio (OR) = 1.92, confidence interval (CI) = 1.52–2.43) versus (OR = 3.09, CI = 2.67–3.49). 9 In another study, the International Index of Erectile Function-5 (IIEF-5) score significantly improved after surgery in patients with hypogonadism, infertility, and varicocele (17.1 ± 2.6 to 19.7 ± 1.8, p < 0.001). 10 In our long-term results, the IIEF-5 score increased, and erectile function was maintained until the last follow-up. We think that our results suggest that varicocelectomy might improve ED, especially in middle-aged men with low testosterone and ED.
The prevalence of varicocele increases with age because the venous valve becomes less competent. 11 In addition, TD and/or ED in men also increases with age. In our clinical cases, microscopic varicocelectomy increased both the serum testosterone level and IIEF-5 in middle-aged men, and this improvement was maintained up to a follow-up of 60 months. We believe our data suggest varicocele repair might be a good option to treat men with TD, especially those who previously had varicocele and side effects of androgen replacement therapy. To confirm this, a large prospective long-term longitudinal study will be needed.
Footnotes
Conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.
Guarantor
J.H.L. is the guarantor of this article.
Contributorship
Conception, design and acquisition of data – J.H.L. and Y.W.P.; drafting the article and revising it for intellectual content – J.H.L. and Y.W.P.; final approval of the completed article – J.H.L. and Y.W.P.