
Abstract
Objective:
Testicular metastasis in prostate cancer is a rare entity. We aimed to report the case where this rare condition was diagnosed with Gallium prostate-specific membrane antigen–positron emission tomography/computed tomography (68Ga-PSMA-PET/CT).
Subjects/patients and methods:
A 68-year-old male with a prostate adenocarcinoma presented with testicular metastasis. The patient was diagnosed with 68Ga-PSMA-PET/CT, and bilateral inguinal orchiectomy was performed. Herein, our case is presented, and a short review of the literature is carried out.
Conclusion:
68Ga-PSMA-PET/CT is an effective imaging method for detecting rare metastases.
Level of evidence:
4
Introduction
Prostate cancer is the second most common cancer in men. According to GLOBOCAN data, it is the sixth most common cause of death. 1 Prostate cancer treatment is tailored according to risk groups, and treatment approaches include radical prostatectomy, radiotherapy, endocrine therapy and watchful waiting. 2
Prostate cancer most frequently metastasizes to regional lymph nodes and the skeletal system. Although rare, lung, liver, peritoneum, adrenal gland and brain metastasis can be seen. 3 Testicular metastasis is very rare in prostate cancer and is presented as case reports in the literature. Testicular metastasis was detected incidentally with bilateral orchiectomy, in the past, in advanced disease. 4 In the literature, the rate of testicular metastasis in prostate cancer is given as 4%. 5 With the abandonment of bilateral orchiectomy and the replacement of endocrine agents instead, the probability of incidentally detecting testicular metastasis has decreased.
Herein, we report a 68-year-old patient with a solitary testicular metastasis of prostate cancer after curative radiotherapy, diagnosed with Gallium prostate-specific membrane antigen–positron emission tomography/computed tomography (68Ga-PSMA-PET/CT). We also present a literature review of testicular metastases diagnosed with 68Ga-PSMA-PET (Table 1). To the best of our knowledge, this is the 10th case to be reported.
Review of cases published of testicular metastasis diagnosed with 68Ga-PSMA-PET/CT.
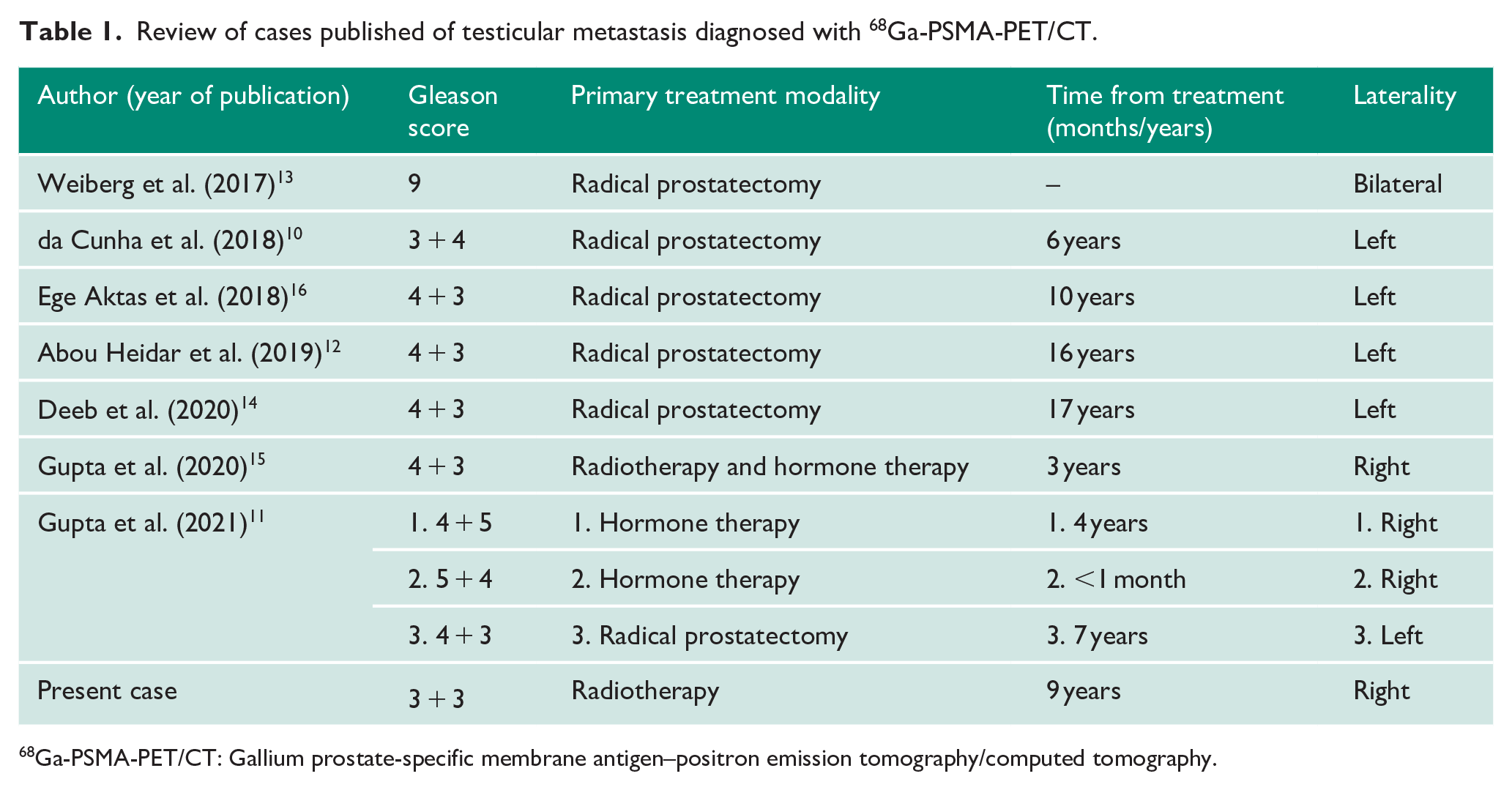
68Ga-PSMA-PET/CT: Gallium prostate-specific membrane antigen–positron emission tomography/computed tomography.
Case presentation
A 59-year-old Caucasian male was admitted to the hospital with polyuria in 2012. Digital rectal exam revealed a diffusely enlarged prostate, and his prostate-specific antigen (PSA) level was 28.8 ng/mL. A prostate biopsy was performed and revealed an adenocarcinoma of the prostate with Gleason score (GS) of 6 (3 + 3, Group 1). Pelvic magnetic resonance imaging (MRI) performed for local disease staging; the tumour was limited to the prostate. Patient staged as T2N0M0 according to TNM (tumour, node, metastasis) staging AJCC (American Joint Committee on Cancer) 8th edition. Subsequent chest–abdomen CT and bone scan confirmed the prostate lesion with no evidence of distant metastasis. The patient was considered as high-risk prostate cancer due to his pre-diagnosis PSA level. Neo-adjuvant androgen deprivation was started for 3 months, followed by prostate radiotherapy. External radiotherapy was applied with intensity modulated radiation therapy (IMRT) technique (54 Gray in 28 fractions to the prostate, distal–proximal seminal vesicles, 76 Gray in 38 fractions to the prostate and distal seminal vesicles). Afterwards, the androgen deprivation was continued for another 2 years. Routine follow-up procedures were carried out, and biochemical relapse was detected on February 2021 with a PSA of 2.2 ng/mL. 68Ga-PSMA-PET/CT performed as a restaging scan. It revealed that increased 68Ga-PSMA uptake with maximum standard uptake value (SUVmax) of 14.8 was detected in the soft tissue lesion, measured 17 mm × 20 mm, in the posterior testis in the right scrotum (Figure 1). Thereupon, bilateral inguinal orchiectomy was performed with the differential diagnosis of primary testicular tumour and metastatic lesion. Pathology revealed metastatic adenocarcinoma in the right testicle. Macroscopic examination of the operative specimen revealed a greyish-white irregular tumour in the testis, without extension to the peritesticular tissues. There was lymphovascular invasion and rete testicular involvement in the pathology report. The epididymis and the spermatic cord showed no infiltration. At the third month follow-up after treatment, PSA was 0.01 ng/mL.
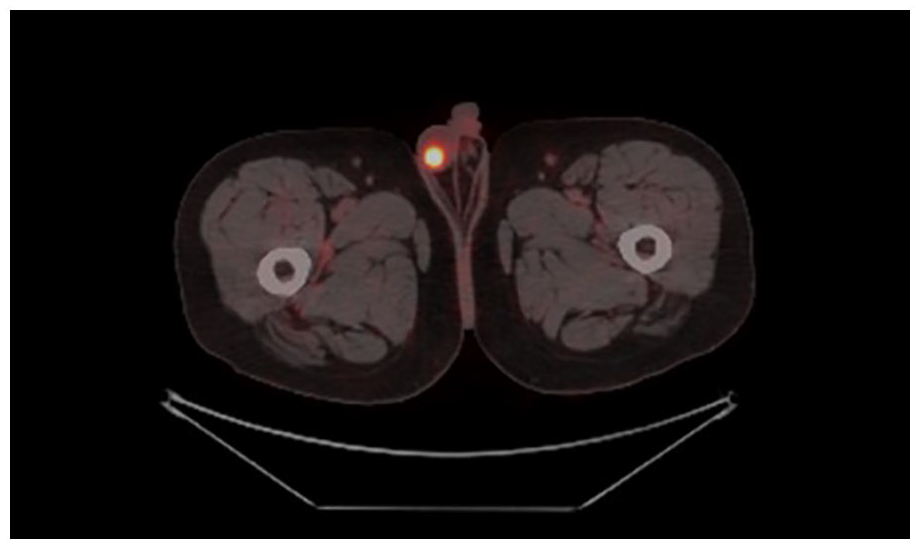
68Ga-PSMA-PET/CT images showed increased uptake in the right scrotum.
Discussion
Testicular metastasis of prostate cancer is a scarce phenomenon. In the autopsy series of 1589 cases conducted by Bubendorf et al., 6 haematogenous metastasis was observed in 35% of the cases. The most common areas of metastasis are bones and the liver. Testicular metastasis was observed in only 0.5% of the cases. Four mechanisms have been proposed for testicular metastasis to occur. These are (1) a retrograde venous extension, (2) a retrograde lymphatic extension, (3) arterial embolism and (4) through the lumen of the vas deferens. 6
Detection of this rare phenomenon is also difficult. Often, it was detected incidentally after bilateral orchiectomy or in autopsy series. When the case reports in the literature are examined in detail, it is seen that metastasis is usually detected by ultrasound when it is symptomatic. This may mean that the disease progresses in the time until it gives symptoms.
68Ga-PSMA-PET/CT is promising for the early diagnosis of such rare metastases. Prostate-specific membrane antigen (PSMA) is a surface protein which highly expressed in prostate cancer cells. 7 Hence, the 68Ga-PSMA ligand has recently emerged as a promising PET tracer. 68Ga-PSMA-PET/CT has been shown to be more sensitive in detecting pelvic lymph nodes and distant metastasis compared to other tracers and is now considered as standard. 8 This new technique provides the opportunity to detect distant and local recurrences with high sensitivity, even at low PSA values in patients with prostate cancer. 9 Since it is a new technique, the number of cases in which testicular metastasis is detected with 68Ga-PSMA in prostate cancer is limited.10 –16 Literature review via PubMed, MEDLINE and Embase database was carried out, and nine published cases published in English were identified between 2017 and August 2021 (Table 1). Of these reports, eight were treated with primary radical prostatectomy, and one with radiotherapy and hormone therapy. Recurrence was encountered between 1 month and 17 years after primary treatment. Our case is the second case in the literature, in which primary radiotherapy was applied.
Testicular metastasis is seen as a symptom of advanced disease and often accompanies multiple metastases.17,18 There are also cases in the literature presenting with solitary testicular metastasis. 19 Testicular metastasis is associated with poor prognosis and often less than 12 months survival.20,21 This poor prognosis can be attributed to the fact that testicular metastases are usually found together with other organ metastases. However, since it is rare, the effect of testicular metastasis on prognosis is not clear. In our case, there was no metastatic lesion other than the testis in 68Ga-PSMA imaging. Considering that 68Ga-PSMA-PET/CT is crucial in the early diagnosis of oligoprogressive disease, the presentation of our case with solitary testicular metastasis can be attributed to the use of 68Ga-PSMA. Thanks to early detection, survival can be prolonged with early diagnosis and treatment in cases with testicular metastasis.
Conclusion
In conclusion, testicular metastasis could be detected in the early period of PSA relapse with 68Ga-PSMA. Our case report highlights the success of 68Ga-PSMA even in unexpected metastatic foci. Therefore, we consider our report to be an important contribution to the literature.
Footnotes
Conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Hacettepe University does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.
Guarantor
G.O. is the guarantor of the paper.
Contributorship
G.O. and M.T.Y. wrote the first draft of the manuscript. All authors reviewed and edited the manuscript, and approved the final version of the manuscript.