
Abstract
Seminal vesicle abscess (SVA) is a rare pathology. We review the literature and present the case of a 54-year-old presenting with an SVA treated successfully with percutaneous transgluteal drainage and subsequently, transrectal ultrasound (TRUS)-guided transrectal drainage.
Introduction
Seminal vesicle abscesses (SVAs) are rarely found in clinical practice and as a result there are no specific guidelines for their management. 1 Its diagnosis can be difficult given the wide range of symptoms it can present with. 1 Treatment includes conservative management with intravenous (IV) antibiotics or drainage, for which there are multiple potential approaches.1,2
Case history
A 54-year-old otherwise well male presented to the Emergency Department (ED) with a 1-week history of irritative lower urinary tract symptoms (LUTS) and intermittent frank haematuria with associated fevers and chills. He had been started on oral cephalexin by his general practitioner (GP) 2 days prior. The patient had no previous history of UTI (urinary tract infection) or STIs (sexually transmitted infections) and had one sexual partner.
On examination, the abdomen was soft, non-tender. Digital rectal examination showed a smooth, enlarged, non-tender prostate. Scrotal exam demonstrated an enlarged, erythematous, left hemiscrotum with a tender epididymis and spermatic chord.
His white cell count (WCC) was 19, neutrophils 15.2, C-reactive protein (CRP) 211, prostate-specific antigen (PSA) 86 with normal renal function and electrolytes. A urine MCS (microscopy, culture, sensitivity) obtained from the GP grew fully susceptible Escherichia coli. The initial computed tomography of kidneys, ureters and bladder (CT KUB) showed a possible SVA and subsequent CT abdomen pelvis with IV contrast (Figure 1) demonstrated an enlarged left seminal vesicle measuring 5 cm × 5 cm × 6 cm anteroposterior (AP) × craniocaudal (CC) × transverse (TR) and diffuse bladder wall thickening suggestive of a left SVA. There was no abnormality of the kidneys, no hydronephrosis/hydroureter and no prostatomegaly.

CT images of seminal vesicle abscess.
The patient was started on IV ceftriaxone and IV fluids. He was initially afebrile but subsequently spiked a temperature of 39°C on transfer to the ward. He continued on IV antibiotics and remained stable and afebrile on the ward. There was a progression in size of the SVA despite IV antibiotics on a repeat CT 3 days later. Magnetic resonance imaging (MRI) pelvis (Figure 2) was performed confirming an increase in size of the left SVA to 5 cm × 7.4 cm × 6.4 cm (AP × CC × TR) with associated left epididymitis but no prostate abscess. A CT-guided percutaneous transgluteal pigtail drain was inserted and yielded 3 mL of pus which grew again fully susceptible E. coli on culture and was negative for malignancy.

MRI images of seminal vesicle abscess.
The patient remained well and was discharged after 1 week with oral ciprofloxacin. However, there was only been a mild reduction in the size of the collection on repeat CT a few days later despite an improvement in inflammatory markers. There had been minimal output from the drain since the procedure. Therefore, the patient was then admitted electively for a TRUS-guided transrectal drainage of the left SVA draining 10°mL of pus and was discharged the following day.
The pus from the surgical drainage grew Enterococcus faecium resistant to amoxycillin and ceftriaxone. The patient was started on a 3-week course of linezolid. There was a marked improvement on repeat CT 3 weeks (Figure 3) after the TRUS drainage leaving only soft tissue thickening and a trivial amount of internal fluid. On follow-up, the patient remained well with no pain or urinary symptoms.

Follow-up CT post TRUS drainage.
Discussion
SVAs are a rare finding with 45 cases reported to our knowledge since 1986. Diabetes mellitus, long-term catheters, urological instrumentation/surgery and congenital anatomical anomalies are potential predisposing factors to SVAs.1,3,4 It is usually preceded by acute bacterial prostatitis, a UTI or epididymitis.1,5 Although our case had a UTI beforehand, we were unable to clearly identify a precipitating cause for his abscess.
It can present with a range of different symptoms such as fever, irritative LUTS, haematuria and testicular, inguinal, abdominal or perineal pain and occasionally erectile dysfunction. 1 This is likely due to its location close to a number of anatomical structures such as the prostate, rectum, urinary bladder, urethra and peritoneum. 6 SVAs can be diagnosed using CT, ultrasound (US), pelvic MRI and fluorodeoxyglucose-positron emission tomography (FDG-PET) scans. 3 TRUS allows simultaneous drainage of the abscess making it both diagnostic and therapeutic. 3 CT is the most commonly used imaging modality in the diagnosis of SVA. Characteristics of an SVA on CT include seminal vesicle enlargement, hypodensities within the seminal vesicle, and adjacent fat stranding. 7 MRI is considered gold standard given its superior tissue contrast, multiplanar capabilities and greater spatial resolution when compared to CT and TRUS. 7
Consistent with a pathogenesis of urinary tract infections, E. coli is the most common causative organism. 3 In our case, E. coli was the initial organism and was consistent with his preceding UTI. However, the subsequent E. faecium grown following the TRUS drainage is likely a healthcare-associated pathogen secondary to the transgluteal and TRUS drainage of the SVA. It is imperative to have adequate prophylactic antibiotic cover given the potential need for multiple procedures to manage an SVA.
There is no gold standard for the management of SVAs and a range of approaches can be considered as seen in historical cases. It is noteworthy that drainage of SVA abscesses can be difficult due to their central pelvic location and will be guided by factors such as individual patient anatomy, presence/absence of prostate enlargement and previous pelvic surgery. A combination of drainage routes may be required as in this case (e.g. percutaneous, transrectal, transurethral, transperineal) using CT or US guidance.
Zagoria et al. successfully drained 40 cc from an SVA abscess via a transurethreal approach resulting in full resolution. 8 Smith et al. described successful percutaneous transvesicle drainage for an SVA abscess involving both CT and fluoroscopic guidance to place a double pigtail stent with one pigtail located in the abscess and the other in the bladder allowing internal drainage of the abscess. 9 However, the procedure had to be performed in two stages without the guidewire being dislodged during transport between fluoroscopy and CT as well as another procedure (cystoscopy) being later required to remove the stent. 9 Sağlam et al. reported transrectal and transperineal US-guided drainage of six SVAs. 2 All six patients’ cultures grew E. coli and at 1-month follow-up had full resolution of the abscesses. However, transperineal drainage can be irritative and transrectal drainage has the risk of rectal flora contamination. 5
Bayne et al. favoured a transgluteal approach due to the low risk of complications. 5 They drained approximately 18 cc of pus from the abscess, and after 72 h, it had completely resolved. This contrasts to our experience of transgluteal drainage which yielded only 3 cc of pus and ultimately required transrectal drainage to achieve resolution. Transgluteal drainage has some practical limitations on the size of catheters which can be inserted safely, as the risk of neurovascular injury increases. Smaller catheters may not adequately drain very viscous material as in this case. Successful laparoscopic drainage has also been previously described. 4
Conservative management with IV antibiotics alone has been effective in some antecedent cases although it is unclear how large those abscesses were.10,11 However, formal surgical drainage is usually necessary due to the multiloculated nature of the abscess. 12 In our case, there was little improvement following the initial radiological guided drainage, again likely due to the smaller drain size and loculated nature of the abscess. TRUS-guided drainage was decided as the follow-up procedure as it allows simultaneous evaluation and drainage of the abscess. 2 It proved effective in definitively treating the SVA.
Summary of drainage techniques for seminal vesicle abscesses in literature.
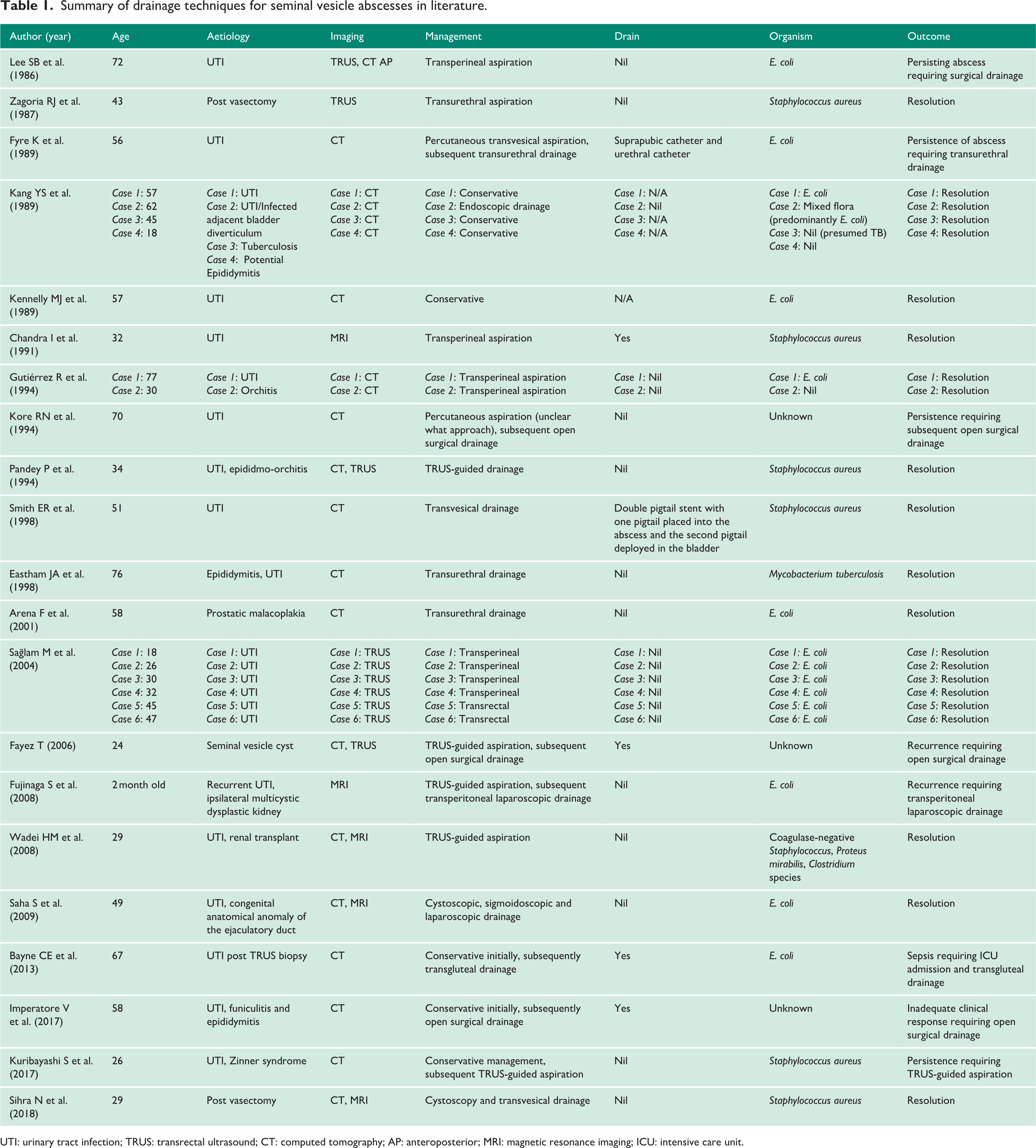
UTI: urinary tract infection; TRUS: transrectal ultrasound; CT: computed tomography; AP: anteroposterior; MRI: magnetic resonance imaging; ICU: intensive care unit.
Conclusion
SVAs are an extremely uncommon finding with no defined management guidelines given its rarity and the multiple surgical and radiological drainage approaches available.
Footnotes
Conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.
Guarantor
S.S.
Contributorship
Finín Cotter wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.