
Abstract

Case report
A 55-year-old man presented to the emergency department with a three-day history of right lower quadrant pain. He had no urinary or bowel symptoms. His surgical history was significant for a pelvic fracture and a bladder rupture requiring repair following a road traffic accident at the age of 24. He had a long history of erectile dysfunction due to type two diabetes, for which he had tried two oral medications, intracavernosal injections and a vacuum constriction device with no success. He subsequently underwent insertion of an AMS penile prosthetic device seven years prior to his presentation. At the time of insertion, the reservoir was placed extra-peritoneally in the right iliac fossa, with the pump located in the right scrotum. His postoperative course at the time was uncomplicated. There were no complications involving the prosthesis in the following seven years. On examination of the patient in the emergency department, he was tender in his right iliac fossa. There was no pain on activation or deactivation of the prosthesis.
The patients’ white cells were mildly elevated, primarily a monocytosis. His C-reactive protein was also slightly elevated. Given the patients’ history of previous abdominal surgery, and the relatively acute onset of symptoms in the right iliac fossa, initially the differential diagnosis included appendicitis, small-bowel obstruction secondary to adhesions or colitis. A computed tomography (CT) scan of the abdomen and pelvis showed minimal fat stranding and trace fluid surrounding the implant tubing in the right hemipelvis tracking forward to the right anterior abdominal wall (Figure 1). Once the CT images were available, the diagnosis of a migrated penile prosthesis reservoir was made. There had been no displacement of the pump or cylinders.
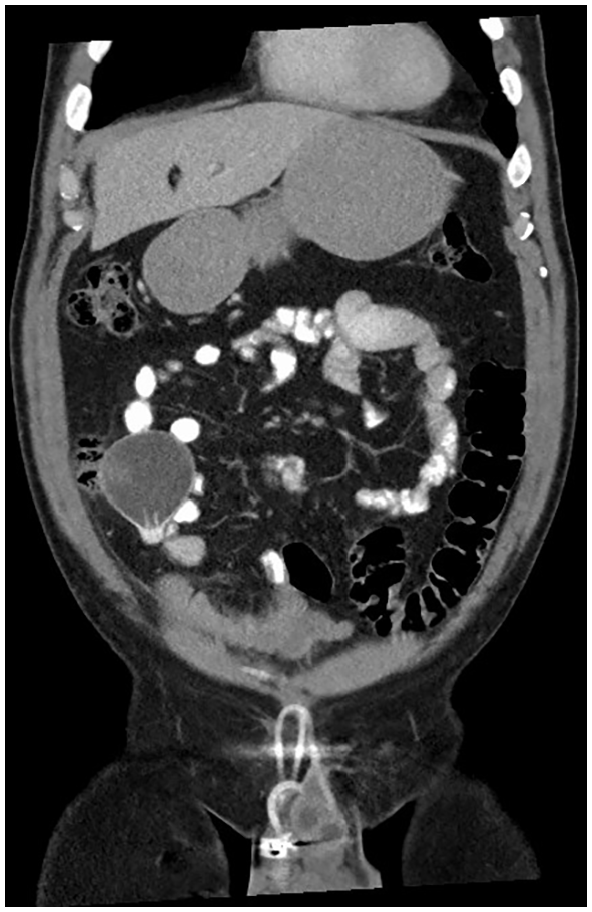
Coronal computed tomography scan showing ectopic location of the reservoir in the abdomen.
Given that there was no evidence of prosthetic infection, it was decided that the most appropriate course of action would be to remove the reservoir. The decision was made to leave the cylinders in place to allow for a replacement device to be inserted by an andrology subspecialist in the future, as the patient had been satisfied with the prosthesis prior to this presentation. The preferred management was for urgent removal of the reservoir during the same admission. However, the patient requested the operation be delayed for family reasons due to a dependent child. As the patient was not acutely unwell, he was discharged. The patient was subsequently admitted six weeks later for elective laparoscopic removal of the reservoir. After minimal dissection of omental adhesions in the right lower quadrant, the reservoir was identified extending anteriolaterally to the caecum (Figure 2). It appeared partly deflated. The tract was dissected in the anterior wall, and the tubing was cut flush with where it exited the peritoneum in the right inguinal region. The lower port site was extended, and the reservoir was removed through it. The patient was discharged home the day after his operation. He is currently awaiting review in a specialist andrology centre regarding re-insertion of a new reservoir. He has not had any further abdominal pain in the nine months since the prosthesis removal.
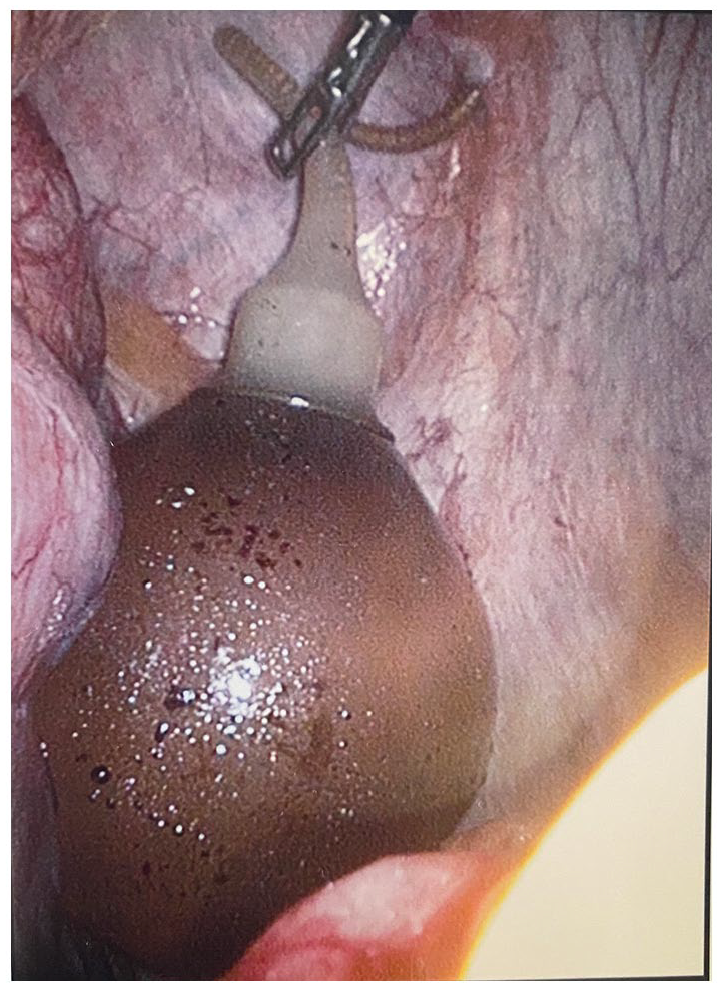
Intraoperative image of reservoir balloon.
Discussion
Erectile dysfunction (ED) is defined as the inability to attain or maintain an erection. It is a common problem, estimated to affected approximately 20% of men. 1 There is a strong correlation with increased age, with prevalence rising to >50% in men aged between 40 and 70. 2 The risk factors for ED are similar to those for cardiovascular disease and include diabetes, smoking, dyslipidaemia, obesity and increasing age. Conservative management measures include weight loss and smoking cessation. Medical management most commonly involves the use of phosphodiesterase inhibitors such as sildenafil. For patients who do not respond sufficiently to oral pharmacotherapy, intracavernosal prostaglandin E1 injections can be used. Some patients prefer not to use intracavernosal injections and can be offered vacuum erection assistance devices as an alternative. For patients who fail to respond to all of the above therapies, insertion of a penile prosthesis is the treatment of choice. Patient satisfaction following insertion of a penile prosthesis has been reported to be as high as 90%. 3
Penile prostheses have been documented in use from as early as the 16th century. A variety of materials have been used in these prostheses over the years, progressing from rib cartilage and bone in the mid-1930s to acrylic implants in the 1960s. 4 These implants were placed within Buck’s fascia but outside the corpora cavernosa, with many patients experiencing complications and implant extrusion as a result. A major development in their design came in 1973, when Scott et al. described the use of intracavernosal, inflatable silicone cylinders. 5 This was the first description of an inflatable penile prosthesis (IPP). Over the years, the design was refined and adjusted to a multicomponent IPP, such as the one seen in this case. These multicomponent IPPs typically consist of a pump located in the scrotum, a reservoir, which is usually filled with water, located in the abdomen and intracavernosal cylinders.
A number of recognized complications of prosthetic devices have been documented in the literature. Glans hypermobility can occur with inadequate prosthesis sizing or positioning. 6 Haematomas may develop postoperatively, most commonly in the scrotum. 7 Patients with pre-existing corporal fibrosis are at increased risk of both corporal crossover and corporal perforation. 6 Urethral, bladder or vascular injuries are more rare complications, but can occur during placement of the prosthesis. Erosion of the urethra, glans or other surrounding structures by the prosthesis is also a recognized complication. 8 The risk of postoperative infection is between 1% and 4%. 8 However, this risk increases in patients with spinal cord injuries, those undergoing revision IPP placement and those with a history of penile reconstruction. 6 Infection is a potentially disastrous complication that often results in the removal of the prosthesis. The Mulcahy salvage technique, whereby the infected implant is removed, the wound is thoroughly washed out and a new implant is inserted is the current management of choice for this complication, although in selected patients, prolonged courses of antibiotics may have success. 9 Perhaps the most serious postoperative complication that can occur is glandular ischaemia, which can lead to penile gangrene and organ loss and requires urgent removal of the prosthesis. 10
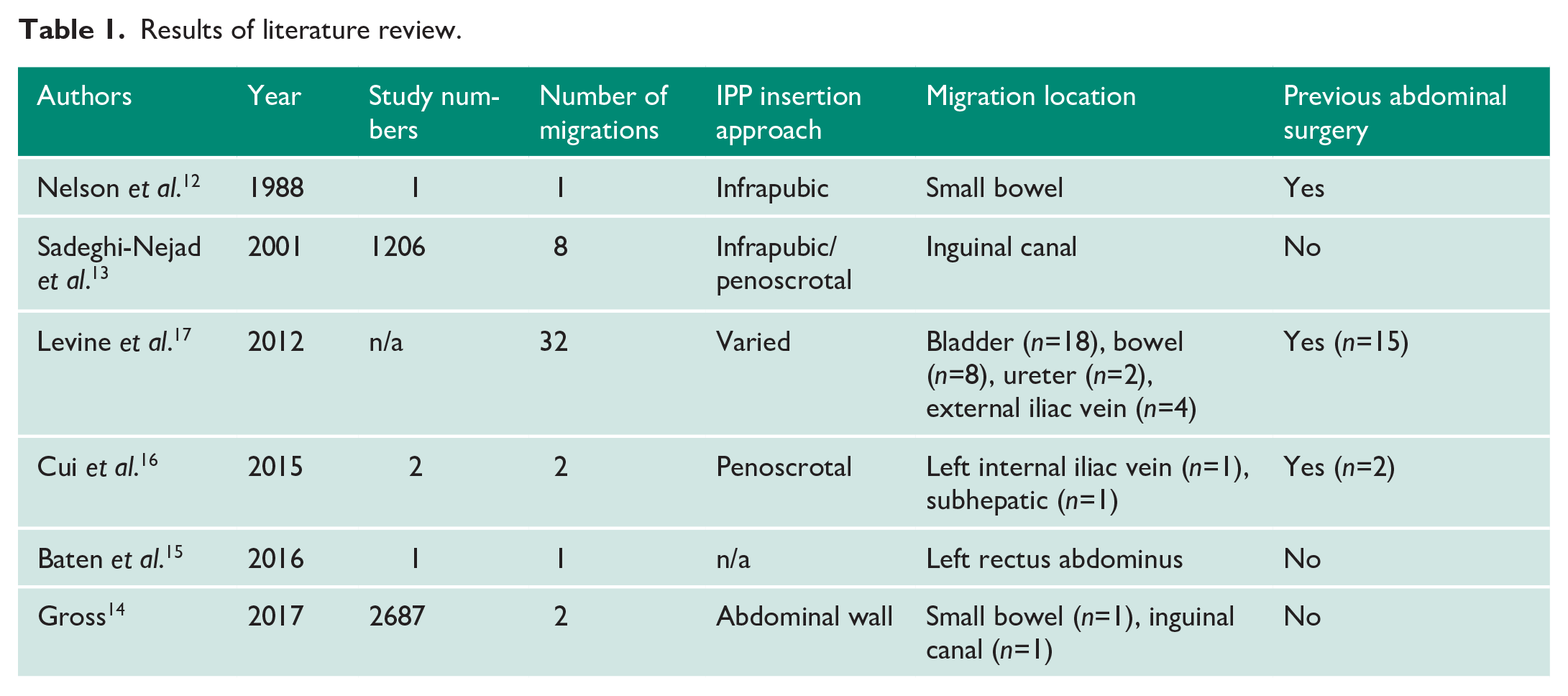
We conducted a review of the literature in order to identify other cases of peritoneal migration, the findings of which are summarized in the Table 1. Traditionally, the reservoir is placed into the space of Retzius using a scrotal or infrapubic approach, with placement of the reservoir in the paravesical space after piercing through the transversalis fascia at the deep inguinal ring. 11 A case in which the patient presented with small-bowel obstruction 18 months after IPP placement necessitated resection of 15 cm of small bowel. 12 This patient had undergone previous cystectomy, with the IPP placed into the space of Retzius via an infrapubic incision. In a case series reporting on 1206 cases of IPP placement, eight (0.7%) cases of reservoir herniation through the inguinal canal occurred. 13 Almost all of these were in penoscrotally placed prostheses. Most occurred in the early postoperative period and were associated with coughing or vomiting. Alternative locations in use for reservoir placement include subcutaneous or submuscular placement anterior to the transversalis fascia. 11 A retrospective analysis of 2687 patients undergoing reservoir placement within the abdominal wall musculature found two patients with peritoneal migration: one of these had the IPP inserted anterior to the transversalis fascia, and one posterior. 14 One patient presented with symptoms of small-bowel obstruction 11 months after the operation, whilst in the other patient the migration was discovered incidentally during a right inguinal hernia repair. The authors identified low body mass index (BMI) and tobacco use as common characteristics of these patients, which may have increased their risk of migration. Baten et al. also reported on a case of reservoir migration from the right pre-peritoneal space to the left rectus abdominus muscle. 15 In a case series by Cui et al., two cases of IPP migration were reported: one in a patient with a history of bilateral inguinal hernia repair who had his prosthesis placed via a penoscrotal approach, and the other in a patient who had a history of prostatectomy whose prosthesis migrated to a subhepatic location. 16 Levine et al. conducted a review of the literature, identifying 19 cases of erosion into the bladder and eight of erosion into the bowel. 17 Of note, all of the patients who experienced IPP erosion into bowel had previously undergone abdominal surgery.
Results of literature review.
The case we have described above is unusual for both the migration intraperitoneally from the right iliac fossa and for the length of time taken for this complication to develop. Our patient had no indication of any issue with the prosthesis prior to his presentation with abdominal pain, with the prosthesis functioning normally for seven years post insertion. The patient in our described case had undergone previous open bladder rupture repair following a traumatic injury. From our review of the literature, it would appear that previous lower abdominal surgery increases the risk for prosthesis migration, potentially due to alteration of the pre-peritoneal space. Whilst tobacco use and low BMI were identified as possible risk factors in one case series, this was not mentioned in any other reports, and our patient did not have these risk factors. Furthermore, although our patient had diabetes, this was not mentioned as a risk factor in any literature we encountered. It is therefore our opinion that patients who have had previous abdominal procedures who are being counselled regarding potential prosthesis insertion should be advised about the higher risk of prosthesis migration, given the high prevalence of these risk factors in the published literature.
Footnotes
Acknowledgements
None.
Conflicting interests
The authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethical approval
Tallaght University Hospital does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patients for his anonymized information to be published in this article.
Guarantor
A.P.N.
Contributorship
All authors contributed to the manuscript and to the care of the patient. R.G.C. conceived the case report. A.P.N. drafted the manuscript and obtained the images used. M.M. and R.G.C. revised the manuscript and made important intellectual contributions. All authors approved the final version of the manuscript submitted for publication