
Abstract
Objective:
The National Health and Nutrition Examination Survey (NHANES) has demonstrated an upward trend in prevalence of kidney stones (KSs) in the past 30 years. We aim to report the current prevalence of KSs.
Methods:
Research was based upon a cross-sectional analysis of response to the 2007–2014 NHANES. The prevalence of self-reported KS history was calculated using weights and design factors reported by NHANES. Four cycles of NHANES data were analyzed separately (2007–2014), and KS-prevalence trends in adult individuals for different age groups were compared. Analysis was performed using SAS ver.9.4.
Results:
The prevalence of KSs was 10.1% for the last 2013–2014 NHANES cycle. The highest prevalence of KSs was observed in males older than 60 years, at 17.8%, followed by males 40–59 years old at 12.6%. This trend changes in the 20–39-year-old age group, wherein females had a higher prevalence than males—7.5% for females compared to 4.5% in males. Females in the study showed a steady increase in KSs prevalence through the study cycles: 6.6% in 2007 to 9.5% in 2013 (p < 0.05). The increase in females ages 20 to 39, almost doubled in prevalence: 3.9 to 7.5%, from 2007 to 2013 (p < 0.05). Females older than 60 years of age have remained stable, with prevalence of 8.9% in 2007 to 9.8% in 2013. Males showed a slight decrease in prevalence from 2007 to 2014, from 12.7% in 2007 to 11.4% in 2014. Prevalence in males and females older than 60 years old were relatively stable.
Conclusions:
Prevalence of KSs has remained stable in males and has increased in females. Females of child-bearing age showed the most significant increase. For this specific group, there has been a steady increase in the last seven years.
Level of evidence:
IV
Background
The prevalence of kidney stones (KSs) continues to rise. 1 This phenomenon has been observed throughout developed and underdeveloped countries. 2 Possible theories supporting these findings include genetic predisposition, 3 diabetes and gout, 4 changes in body mass index and obesity, a poor diet, 5 climate changes,6,7 environmental and work hazards.8,9 The annual cost of KSs, inflation-adjusted for 2014, has been estimated at US$2.81 billion. Due to the positive correlation between obesity and KSs prevalence, the cost of KS is projected to increase to US$1.24 billion per year by 2030. 10 We aim to analyze the latest National Health and Nutrition Examination Survey (NHANES) data to investigate this trend in the USA.
Methods
This is an IRB approved analysis of the NHANES cycles starting in 2007–2014. NHANES is a stratified, multistage probability survey of the non-institutionalized US population. The prevalence of self-reported history of KSs by using each cycle’s NHANES data cross-sectionally was analyzed.
Study population
The setting of the analysis is based on a survey type of data acquisition of the last two cycles of the NHANES results: 2011–2012 and 2013–2014. Additionally, 2007–2014 data was analyzed to give temporal trends. The population included males and females of different age groups. Risk factors such as obesity with KS history were identified in the population of patients who responded during the medical examination component. The NHANES data regarding KSs asked specifically: “Have you ever had kidney stones?” The NHANES data is organized in three age-group cohorts as such: 20–39, 40–59 and above the age of 60. For our data to be congruent with the Centers of Disease Control (CDC) we used the same age cohorts in adult participants of the NHANES.
Outcomes
Participants of the 2007–2014 NHANES data population were identified for the analysis based on a positive answer to questions regarding KSs history. This demonstrates the life-long history of self-reported KSs or point prevalence. In this manuscript the term “prevalence” will be used to describe the population studied.
Covariates
Age, gender and ethnicity were included from the 2007–2014 NHANES cohorts. Individuals were divided into three age groups: 20–39, 40–59 and over 60. Ethnicity/race categories included non-Hispanic whites, non-Hispanic black, Mexican-American, other Hispanic, and other race/multiracial.
Statistical analysis
This is a cross-sectional analysis of response to the 2007–2014 NHANES. Prevalence of self-reported KS history was calculated using weights and design factors reported by NHANES. The data was adjusted for the US population from 2007 to 2014 using the weights, a built-in feature of the data designed, calculated and provided by NHANES, so that we may use prevalence to estimate the whole population. The trends of KS prevalence in males and females in different age groups were compared using the Z-Test, adequate for large sample size population studies. All statistical analyses were conducted using SASv.9.4.
Results
Prevalence of KSs was reported at 3.2% in 1980 9 , 5.2% in 1994 10 , 8.8% in 2010 and 10.1% in 2014 (Figure 1). The total number of participants from each cycle analyzed from NHANES, who answered the question regarding KS history, are as follows: 5935, 6218, 5560 and 5769 from cycles 2007–2008, 2009–2010, 2011–2012 and 2013–2014 respectively. The total number of subjects who had KSs or responded positively to the question: “have you ever had kidney stones?” were 539, 542, 458 and 535 from cycles 2007–2008, 2009–2010, 2011–2012 and 2013–2014 respectively. The weighted overall prevalence of KS disease in males was 10.9% (95% CI, 9.1–12.6) and 9.4% (95% CI, 7.6–11.1) in females for the latest reported NHANES data from 2013–2014 (Table 1).
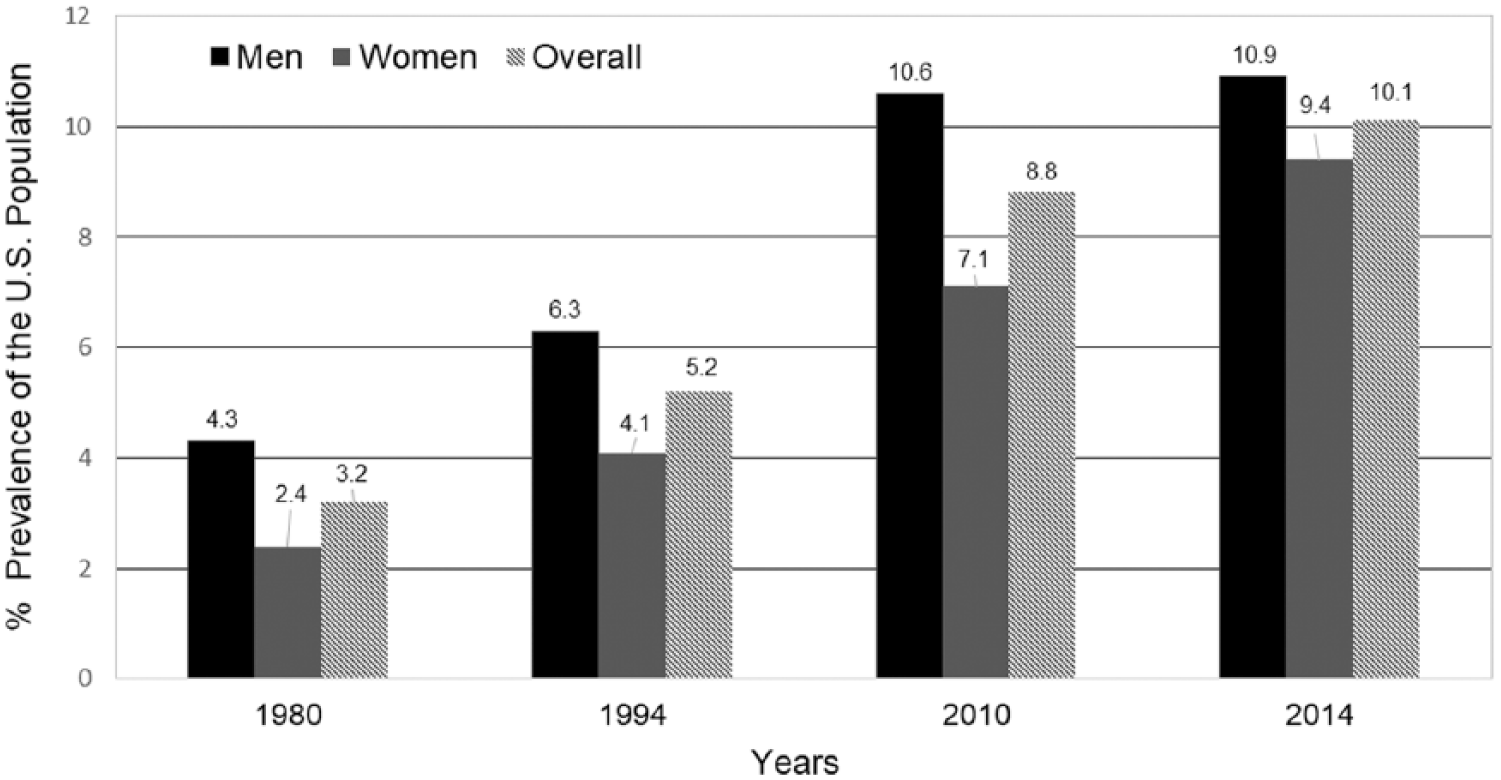
Prevalence of kidney stone disease in the last three decades in the USA: NHANES cycles from 1980–2014.
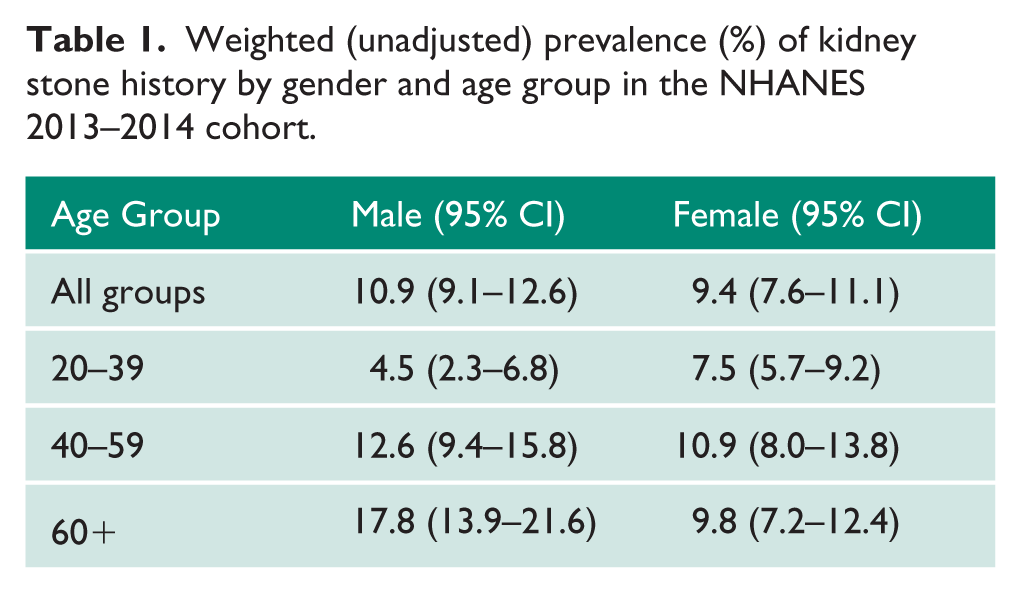
Weighted (unadjusted) prevalence (%) of kidney stone history by gender and age group in the NHANES 2013–2014 cohort.
Age
In males, the age-unadjusted prevalence of KSs was 10.9% (95% CI 9.1–12.6) and the age-adjusted prevalence was 11.4% across all ethnicities. In females the age-unadjusted prevalence was 9.4% (95% CI 7.6–11.1) and the age-adjusted prevalence was 9.5% across all ethnicities. Among males and females in the second and third decade of age, females had a higher prevalence than males at 7.5% (95% CI 5.7–9.2) v. 4.5% (95% CI 2.3–6.8) respectively. Males had a higher prevalence of KS when compared to females in their fourth and fifth decade of age, at 12.6% (95% CI 9.4–15.8) v. 10.9% (95% CI 8.0–13.8), as well as at and after their sixth decade of age, at 17.8% (95% CI 13.9–21.6) v. 9.8% (95% CI 7.2–12.4). In males, the highest prevalence of KS was observed after the sixth decade of age and in females it was observed at the fourth and fifth decade of age, at 17.8% (95% CI 13.9–21.6) and 10.9% (95% CI 8.0–13.8) respectively. Young males in their second and third decade of age, had the lowest prevalence of KS at 4.5% (95% CI 2.3–6.8), when compared to females in the same age group.
Ethnicity
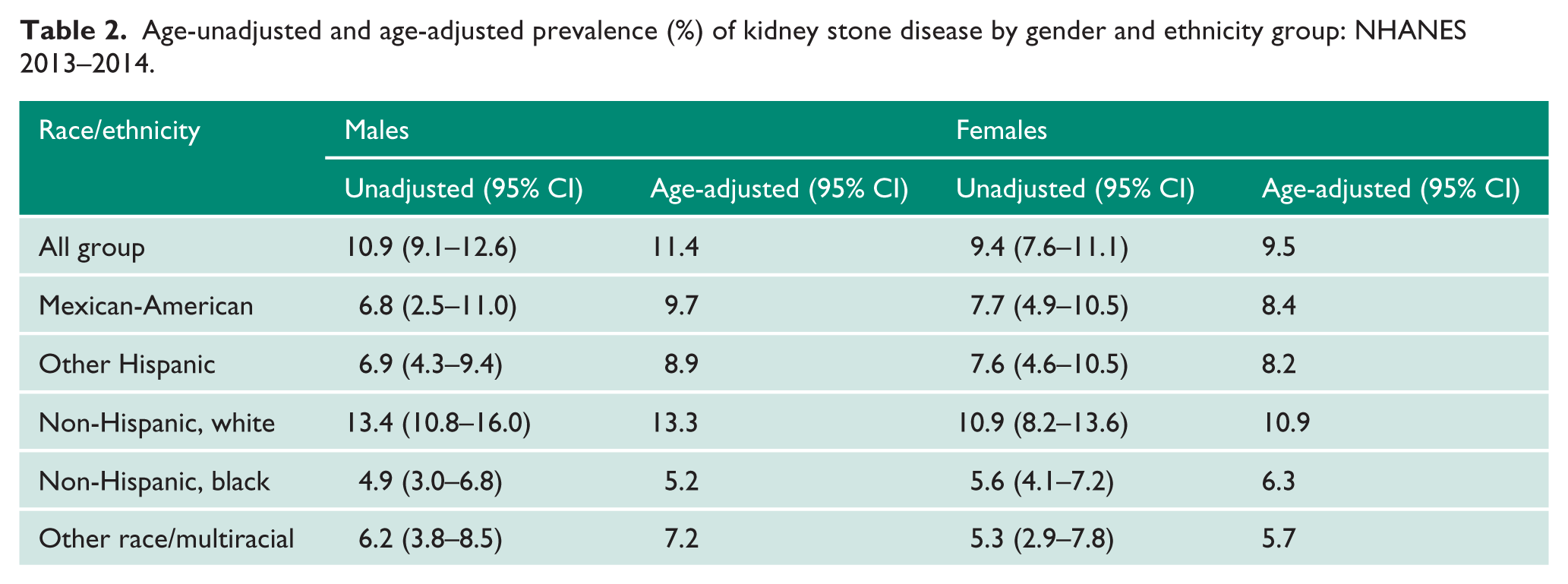
Among different races and ethnicities, after adjusting for age, non-Hispanic whites had the highest prevalence at 13.3%; the age-unadjusted prevalence was 13.4% (95% CI 10.8–16.0). In females, the age-adjusted and age-unadjusted prevalence were both 10.9—unadjusted with a 95% CI 8.2–13.6. In descending order, this cohort was followed by Mexican-Americans, with adjusted prevalence of 9.7%, and unadjusted prevalence of 6.8 (95% CI 2.5–11) in males and 8.4% in females; the unadjusted prevalence for this cohort was 7.7 (95% CI 4.9–10.5). On the other hand, the lowest prevalence was observed in non-Hispanic black individuals with the adjusted prevalence of 5.2% and unadjusted prevalence of 4.9% (95% CI 3.0–6.8) in males and 6.3% in females, with unadjusted prevalence of 5.6 (95% CI 4.1–7.2). This was the only ethnic population where both adjusted and unadjusted prevalence was higher in females than males (p < 0.001) (Table 2).
Age-unadjusted and age-adjusted prevalence (%) of kidney stone disease by gender and ethnicity group: NHANES 2013–2014.
Trends in genders and age groups
When comparing the prevalence of KSs in different age groups, there was a trend of decreasing prevalence of KSs in youngest group of males. Males demonstrated a downward trend in KSs prevalence from 5.5% in the 2007–2008 group to 4.5% in the 2013–2014 group (p = 0.31). Males in the fourth and fifth decade of age demonstrated a smaller difference but still showed a rather insignificant decrease in prevalence from 12.9 to 12.6% from 2007 to 2014 groups (p = 0.85). Males in the sixtieth decade of life demonstrated a decrease trend in prevalence from 20.4 to 17.8% from 2007–2008 to 2013–2014 group (p = 0.14). For males, this has shown an overall decrease in KSs prevalence from 2007 to 2014 from 12.7 to 10.9% (p = 0.027).
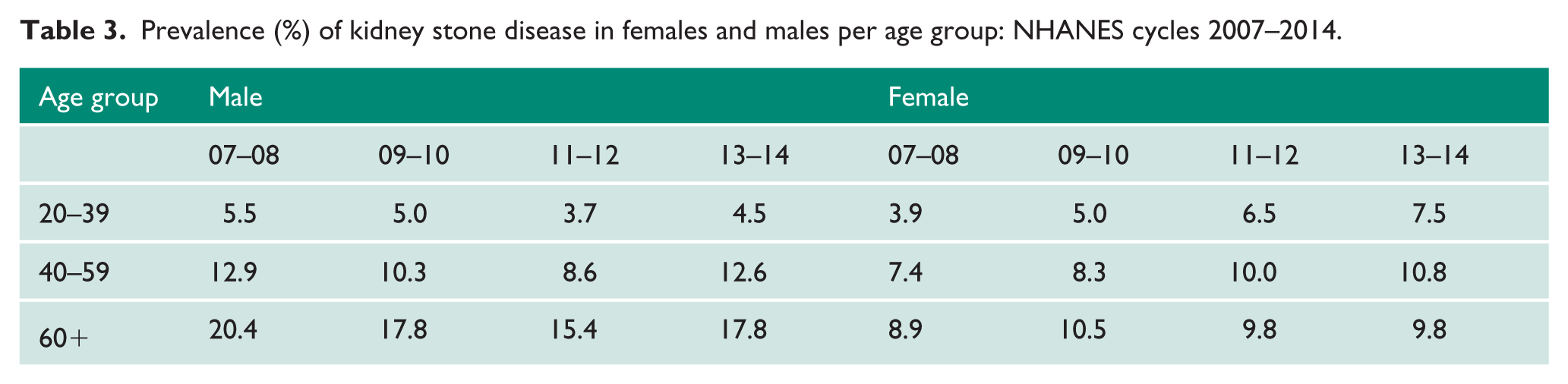
In females, we observed a steady, significant increase in prevalence of KSs, in the second and third decade of age or youngest cohort (Figure 2), with prevalence increasing from 3.9 to 7.5% from 2007 to 2014 (p = 0.0006). This trend steadily and consistently increased throughout the seven-year period. An increase was also observed in females in their fourth and fifth decade of age, from 7.4 to 10.8% (p = 0.0087). This cohort had a higher prevalence than the over 60 years of age cohort, a phenomenon which is not observed in the male population. After the sixtieth decade of age, an increase from 8.9 to 9.8% was observed from 2007–2008 to 2013–2014 groups (p = 0.47). Overall, there has been an increase in the prevalence of KSs in the female population from 6.6% in 2007 to 9.4% in 2014 (p = 0.0001) in younger women of childbearing age (Table 3).
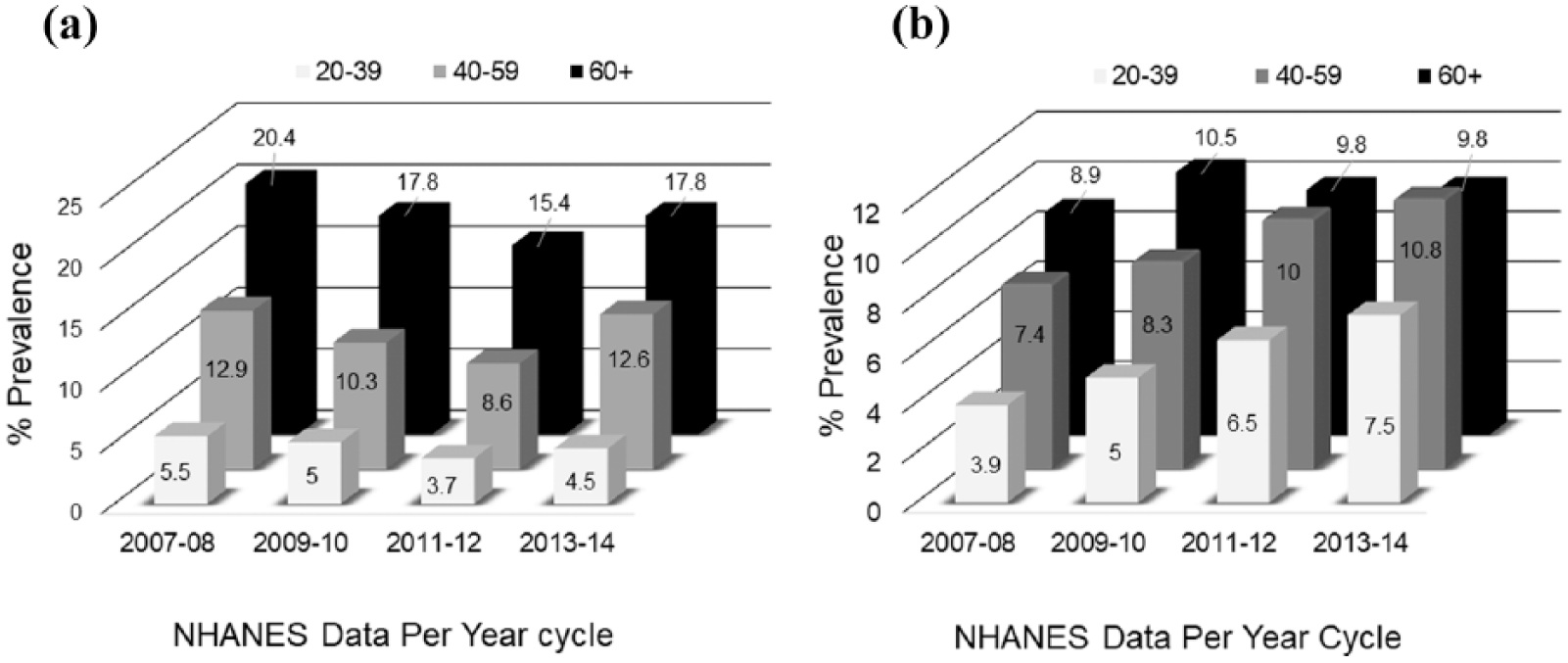
Kidney stones’ prevalence trends in (a) males and (b) females (NHANES).
Prevalence (%) of kidney stone disease in females and males per age group: NHANES cycles 2007–2014.
The prevalence of KSs across gender, ethnicity and age groups in the 2013–2014 NHANES cohort increased with obesity with OR of 1.79 (95% CI 1.47–2.18). It also increased with diabetes with OR of 1.60 (95% CI 1.33–1.92). Finally, gout was also found to increase the OR of having KSs by 1.33 (95% CI 1.01–1.77). The NHANES cycles analysis from 2007 through 2014 demonstrates a significant increase in KS in the younger female-population cohort compared to the other age group cohorts in both males and females. This trend is comparable to the obesity trend in the same age groups, which was reported by the CDC (Figure 3). The prevalence of obesity for females from the 2009–2010 cycle demonstrated an increased prevalence per decade of age; with the highest prevalence after the age of 60 (Figure 3(a)). The same patterns were observed in the female KS-former population (Figure 3(b)), in which the highest prevalence of KS formers were females in the sixtieth decade of age. In our study, we found that among males, KSs prevalence has reached a plateau; in the female population under the sixtieth decade of age, prevalence appears to be increasing consistently for the last decade. We discovered significant difference in trends of KSs prevalence in the most recent 2013–2014 cycle—a shift of prevalence increasing in younger females. This finding was significant in the 2011–2012 cycle, where for the first time, females of the twentieth and thirtieth decades of age had a higher prevalence of KS disease than their male cohorts —3.7 v. 6.5%—and this trend continued in 2013–2014 at 4.5 v. 7.5%. A similar trend was found in females in their fortieth and fiftieth decade of age. In 2011–2012, the prevalence was 8.6% in males v. 10.0% in females, but this trend changed in 2013–2014 with a higher prevalence in males at that age cohort (12.6% males v. 10.8% females). When considering the trends of obesity reported by the CDC, 11 we found that patterns of obesity and KS are similar in females. In the 2013–2014 cycle, the highest prevalence of obesity has shifted from the older than 60 years of age to females in the fortieth and fiftieth decade of age. 11 Although this pattern has been observed in previous cycles, the patterns of KSs in the 2013–2014 cycle was similar (Figure 3(c) and (d)).
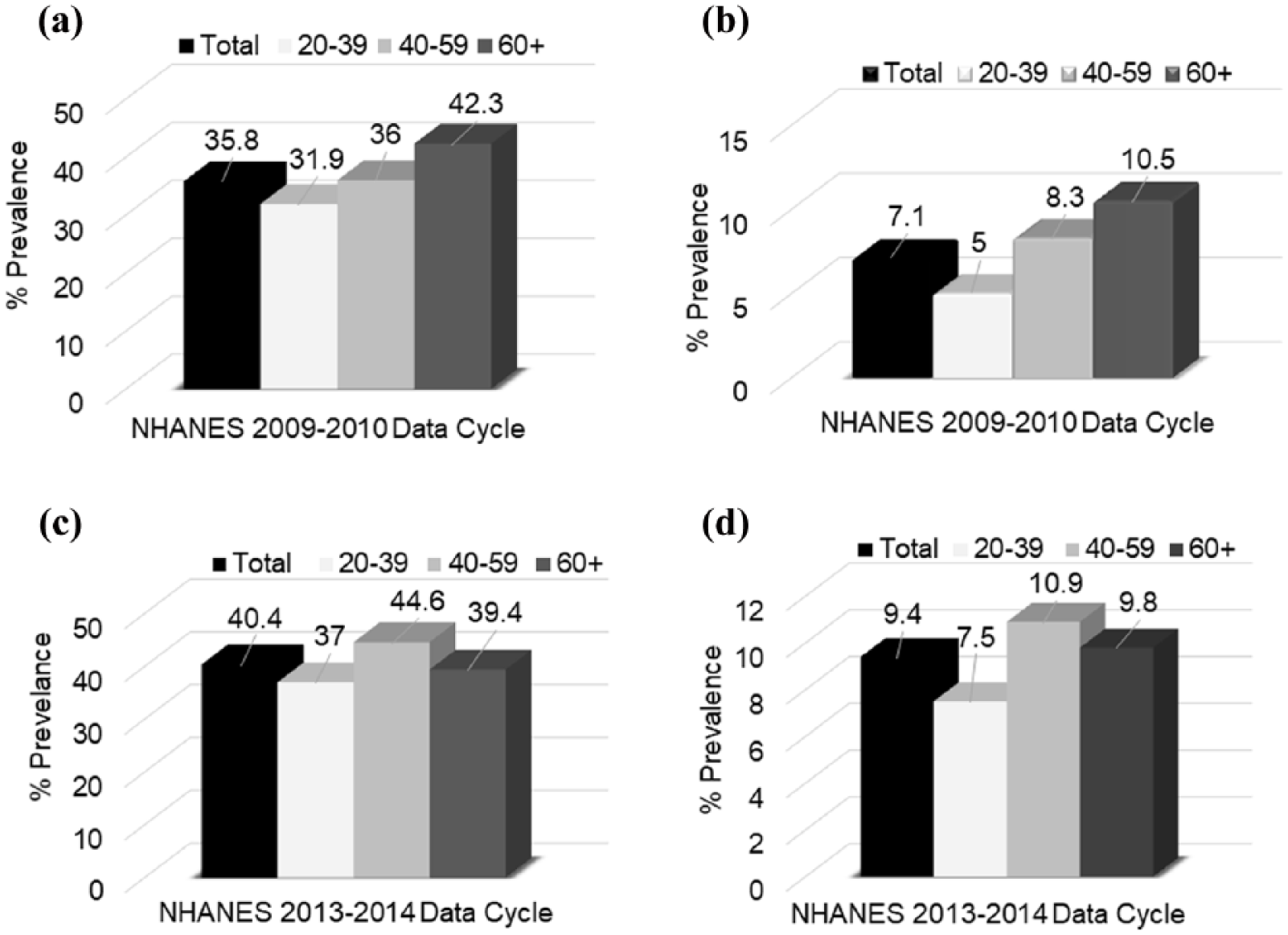
The comparison of obesity and kidney stone disease prevalence in the female population across age groups: NHANES 2009–2010 and NHANES 2013–2014. (a) Prevalence of obesity in females age 20–60+ in the NHANES 2009–2010 cycle. (b) Prevalence of kidney stone disease in females age 20–60+ in the NHANES 2009–2010 cycle. (c) Prevalence of obesity in females age 20–60+ in the NHANES 2013-2014 cycle. (d) Prevalence of kidney stone disease in females age 20–60+ from the NHANES 2013–2014 cycle.
Discussion
The overall prevalence of KSs has increased in the USA in the past 30 years.12,13 The steady increase in prevalence is correlated to the significant cost in KS-related spending. 14 The Urologic Diseases in America reported in 2012 that KSs is the costliest urologic disease in the USA when compared to the costs of other urologic diseases when aggregated together, including prostate cancer. 15
An increase in prevalence of KSs within other diseases, such as obesity and diabetes, 16 poses a significant economic burden on society, thus the importance of pathways for disease prevention17,18 The cost of KS care was estimated to be US$4 billion in 2007, and due to population growth alone, this is projected to increase by more than US$780 million by 2030.10,12,19 The presence of KSs also places individuals at a 50–67% higher risk of developing chronic kidney disease. 20 The multifactorial causality of KSs poses a challenge in the efforts to simplify its etiology. A proposed theory of KS formation has identified reactive oxygen species as a trigger of a cascade of molecular cellular mechanisms which, under certain conditions, induces cells to generate calcifications, not only in the kidney but also the vascular space.21–23 A family history of KSs has been associated with an increased risk of KS formation. 24 Risk factors for KSs include sarcoidosis, 25 renal tubular acidosis, 26 inflammatory bowel disease, 27 hyperoxaluria, 28 hypercalciuria, Dent’s disease 29 and cystinuria. 30 Hypertension, obesity and diabetes, and the metabolic syndrome 31 have also been associated with KSs. Obesity has been linked to increase in uric acid and calcium in urine as well as lower urine pH, which contribute to formation of KSs. 32 Physiologically, obesity promotes insulin resistance, which lowers urinary pH and increases urine acidification. Impaired urinary ammonium excretion and decreased urinary pH is a consequence of increasing insulin resistance in renal tubular cells. 33 Insulin activates the exchanger, which promotes ammonia to become trapped in the renal tubule as ammonia becomes bound to hydrogen ions and is converted to ammonium. 26 Diabetic KS formers were found to excrete significantly more oxalate than normal, 34 which increases the risk of calcium oxalate KSs.
Previous NHANES data reports take the relationship between obesity, diabetes and gout with KSs into consideration when assessing risks. Scales et al, reported KS risk was associated with gout and diabetes in multivariable regression analysis. A prospective study in three large cohorts with a 46 year-combined follow up, demonstrated that weight gain (BMI ≥ 30), after adjusting for age, dietary factors, fluid intake and thiazide use, increased the risk of KSs especially in females, with a relative risk of 1.90 and 2.09 in older and younger women respectively. Our data found increased odds of having KSs with obesity, diabetes and gout. We compared the female population KS trends with obesity trends in the USA. Although the trends of obesity patterns in men and women fluctuate within different NHANES cycles, we drew attention to the 2009–2010 NHANES cycle where a specific pattern in female obesity and KS prevalence are most alike. Despite short-term fluctuations, the larger pattern is visible over time, and it is consistent with the increase in obesity and KS disease in the younger female population. These observations suggest that the trends in the prevalence of KS disease may be associated with changes in BMI. However, due to the cross-sectional nature of the data, we cannot determine the direction of such correlation.
The most significant difference from the previous NHANES data reported since 1994 is the increasing prevalence of KSs in the younger female population. This prevalence increase was not found in the non-Hispanic white females, but in the minority younger female population, including the non-Hispanic black female population. This ethnic group is unique because non-Hispanic females have a significantly higher age-adjusted and age-unadjusted prevalence of KSs compared to the non-Hispanic black males. This is a new finding that points towards an increase in prevalence of KS disease in a minority female population group. Increased prevalence of KSs was also observed in the age-unadjusted female Mexican-American and other Hispanic groups compared to their male counterparts. The increase in prevalence of KSs in these minority female populations could explain the overall trend of increasing prevalence in younger women compared to their male cohorts.
Scales et al. took into consideration the possibility of treatment bias and gender-based practice variation. Women may be more likely to be treated as an inpatient for stone disease than males, and due to the cross-sectional nature of the NHANES dataset, it is difficult to test the above hypothesis. 35 However, current US trends have consistently demonstrated an increasing prevalence in the female population. Regarding obesity trends in the USA, the CDC report of obesity prevalence in the female non-Hispanic black and Hispanic individuals, to be higher compared to non-Hispanic white females. The shift in KS prevalence and the possible association of obesity in the minority younger female population may provide a scaffold for possible preventive measures in this specific population. 11 The limitations of our study include the cross-sectional nature of the NHANES database. Since the relationship of events and KS formation may not have a temporal relationship, it may not match the individual’s KS episode and other disease condition or events.
Conclusion
Prevalence of KSs has remained stable in males and has increased in females, with significant increase in females of child-bearing age. Further research is needed to address the increase in prevalence of KSs in the female population. It is possible that diet, life style, access to health care, working status, compliance to medical care and other factors may play a role in these findings.
Footnotes
Acknowledgements
None
Conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
IRB approved as exempted study for data analysis
Informed consent
Not applicable.
Guarantor
V.Y.B.
Contributorship
V.Y.B. researched literature and conceived the study, gaining ethical approval for the study and wrote the first draft of the manuscript. M.P. was involved in the protocol development and study design. Z.C. was involved in data gathering and data analysis. All authors reviewed and edited the manuscript and approved the final version of the manuscript.