
Abstract
While early treatment of primary prostate cancer is very effective, the incidence of primary prostate cancer continues to rise and therefore the detection of men with high-risk non-metastatic prostate cancer and their subsequent management is becoming increasingly important. There continues to be no molecularly-targeted or chemotherapeutic options with proven, statistically significant survival benefit in this setting. However, there are indications that further risk stratification using molecular features could potentially help distinguish indolent from aggressive prostate cancer, ultimately providing biological markers that could guide a more personalised approach to therapy selection.
Keywords
Introduction
Prostate cancer is the second most common cancer in men.1–3 Nearly 90% of prostate cancers are clinically localised at the time of diagnosis.4,5 The clinical course of localised prostate cancer is highly variable. While many patients have indolent cancers (cured with initial therapy, or observed and treated on progression), other patients have aggressive cancer that will recur after initial treatment. It is estimated that around 15% of all prostate cancer diagnoses could be classified as ‘high-risk’ disease. 6 The 10-year survival rate for men with high-risk prostate cancer has been reported to range from 65% to 91%, and an increasing aggregate of high-risk features correlates with worse outcome. 7 For a full review of the classification and therapy of high-risk prostate cancer, readers are directed to a review by Chang and colleagues. 8
Systemic chemotherapy in addition to definitive management to reduce the chance of recurrence and ultimately death from cancer has a proven role in certain tumour types such as breast, colorectal, bladder or lung cancers. Chemotherapy is given before (neoadjuvant) or just after (adjuvant) definitive therapy (surgery and/or radiotherapy). Often the overall benefit to the treated population may appear numerically small, for example; five-year overall survival (OS) rates for patients with bladder cancer increases by around 5% following neoadjuvant chemotherapy. 9 Comparatively few advances have been made to define additional systemic therapy for men with prostate cancer.
Localised prostate cancer is commonly risk stratified into low-, intermediate- or high-risk, most widely by the D’Amico classification using prostate-specific antigen (PSA) and histological criteria. 10 It is plausible that such classifications may not adequately define populations of men with prostate cancer for additional medical therapy, which has hampered clinical trial design. It is possible that clinical signals of activity from subgroups of patients might have been diluted in a heterogeneous, larger population of men with prostate cancer that did not require additional treatment. Advances in risk stratification may better define populations of men to enter into peri-operative studies; for example, the utility of genomic tests such as Prolaris and Oncotype DX are being investigated to support treatment decisions for men with prostate cancer.
Androgen ablation has been the mainstay of medical treatment for men with prostate cancer since the 1940s. However, drug therapy for men with late-stage ‘castration-resistant’ prostate cancer (CRPC) has altered markedly in the last decade. Several drugs (i.e. cabazitaxel, abiraterone, enzalutamide, alpharadin, sipuleucil T), with varying mechanisms of action, have been approved based on improved OS within randomised clinical trials. Also, reflecting a new paradigm of early systemic treatment, recent and compelling evidence has altered clinical practice. Multiple studies have confirmed docetaxel chemotherapy given to men with hormone-sensitive prostate cancer improved overall survival.11–14
Current neoadjuvant and adjuvant hormonal therapy practice
The role of neoadjuvant hormonal therapy prior to prostatectomy has not been well established15,16 and the clinical trial data have been reviewed by McKay and colleagues. 17 Furthermore, the morphological changes induced by neoadjuvant androgen ablation may complicate assessment of surgical margins and capsular involvement. 18
Adjuvant androgen-deprivation therapy (ADT), after radical prostatectomy (RP), is restricted to cases with positive pelvic lymph nodes. Trials in this setting report mixed findings; for example a study by Messing et al. 19 demonstrated improvement in OS for patients treated with immediate ADT (hazard ratio (HR) 1.84; 95% confidence interval (CI) 1.01–3.35). However, a subsequent meta-analysis of 731 men with positive nodes failed to demonstrate a survival benefit of ADT initiated within four months of RP compared to observation. 20
For patients that are treated with radiotherapy, neoadjuvant or adjuvant ADT combined with radiation therapy (RT) are part of current standard practice for men with intermediate and high-risk localised prostate cancer. 21 Improved OS and cancer-specific survival data from multiple studies22–26 have reinforced the recommendation that men without significant comorbidities should be offered six months of ADT before, during or after radical external beam radiotherapy. Consideration of continuing ADT for up to three years should be made in men with high-risk disease alone, supported by data suggesting improvements in OS of up to 13% compared to short-term suppression.27–29
Adjuvant and neoadjuvant chemotherapy
The role of neoadjuvant chemotherapy has not been established in the treatment of prostate cancer when given with or without androgen deprivation. 17 Previous, small, phase 2 studies have investigated single-agent docetaxel or combination therapy, e.g. docetaxel and estramustine or estramustine and etoposide.30–33 In general, authors conclude neoadjuvant chemotherapy may have a role in treatment of high-risk or locally advanced prostate cancer. However, evidence of survival benefit from randomised clinical trials has yet to be reported. Maturation of data within the Phase III GETUG 12 and SWOG (NCT00430183) trials is awaited. Early results reported from GETUG 12 support an improvement in relapse-free survival following docetaxel chemotherapy.34,35
Adjuvant chemotherapy to treat men with prostate cancer also remains contentious. For example, the RTOG 9902 trial compared ADT and RT vs. ADT and RT followed by chemotherapy (paclitaxel, estramustine and etoposide) for men with localised, high-risk prostate cancer. This study reported increased toxicity with no OS benefit from the investigational arm.36,37 The RTOG 0521 study compared outcomes in 562 men with high-risk, localised prostate cancer treated with two years of androgen suppression plus RT, with or without the addition of adjuvant chemotherapy (docetaxel and prednisone). Preliminary results reported a trend to improved OS at four years (93% vs. 86%) for men treated with adjuvant docetaxel; a short OS assessment was incorporated and additional follow-up to determine long-term benefits was recommended. 38 A further study, SWOG 9921, that compared adjuvant therapy (ADT alone or combined with mitoxantrone) was terminated early due to a safety issue.
Adjuvant and neoadjuvant targeted therapies
To date, early prostate cancer treatment decisions are still based almost exclusively on histological architecture (Gleason score)39,40 PSA levels 41 and local disease extent. 42 We are yet to realise the potential of personalisation of therapy with targeted treatments in prostate cancer.
Prior to addressing the full scope of potential in (neo)adjuvant targeted therapies, addressing new ways of targeting the androgen receptor should be discussed first. Markers of biological response and resistance have been reported in small studies of neoadjuvant ADT. In a study by Mostaghel et al. 43 evaluating the effect of neoadjuvant ADT on gene expression in RP samples from men with localised prostate cancer, chemical castration was found to reduce tissue androgens by 75% and reduce the expression of several androgen-regulated genes (e.g. NDRG1, FKBP5 and TMPRESS2). However, androgen receptor (AR) and PSA gene expression were not suppressed, suggesting that suboptimal suppression of the AR axis at the tumoural level may lead to resistance in a low androgen environment. A different study by Mostaghel et al. 44 looked at the correlation between tissue androgen levels (dihydrotestosterone and testosterone) and change in tumour volumes after three months of various combinations of neoadjuvant hormonal therapies, but found none. These studies serve to emphasise the need for novel therapies targeting complete suppression of the AR axis, to aid in improving local and systemic control of intermediate to high-risk prostate cancer.
Gonadotropin-releasing hormone (GnRH) antagonists such as degarelix 45 offer an alternative to luteinising hormone-releasing hormone (LHRH) agonists, as a result of immediate competitive binding to GnRH receptors. Abiraterone is also being assessed in the neoadjuvant setting in combination with an LHRH agonist, and preliminary results have shown that tissue androgens were significantly more suppressed with abiraterone and pathologic responses were favourable. 46 In another study, androgen signalling and proliferation suppression was again more profound with the combination of abiraterone plus an LHRH agonist, compared to LHRH monotherapy. 47 Similarly, investigations into enzalutamide are ongoing.
Better understanding of prostate cancer biology and the ability to adapt therapy to specific patients and their cancers remains the subject of active research, reviewed by Fraser and colleagues. 48 Recent studies show that prostate cancer can be stratified according to molecular signatures.49–53 The genetic changes associated with aggressive prostate cancer, when present in early tumours, herald the onset of early biochemical relapse. 54 The Cancer Genome Atlas (TCGA), 55 a comprehensive molecular analysis of 333 primary prostate carcinomas, has revealed a ‘molecular taxonomy’ in which 74% of analysed tumours fell into one of seven subtypes defined by specific gene fusions (ETS family, SPOP, FOXA1 or IDH1) or molecular defects in signalling pathways such as PI3K, mitogen-activated protein kinase (MAPK) or DNA repair. This effort though still leaves 26% of tumours unclassified. Similarly, the CamCap study group also undertook a comprehensive, integrated analysis of genomic and transcriptomic data from a study of 482 tumour, benign and germline samples, including 259 men with primary prostate cancer. 56 Five distinct molecular profiles for primary prostate cancer were identified that were predictive of biochemical relapse, based on the integrative analysis of transcript levels and somatic copy number alterations (CNAs). Other studies have also used whole-genome sequencing to characterise tumour heterogeneity and improve our understanding of how the subclonal architecture and diversity of tumours changes during metastasis and progression to lethality.57–59 Building from these studies, work is ongoing to develop personalised or precision medicine treatment for men with prostate cancer.
Published studies to date have focussed on targets that may be more relevant in CRPC and usually have been performed in populations without the aid of biomarker selection to enrich the patient population for those most likely to benefit. Examples include studies targeting angiogenesis and vascular endothelial growth factor receptor (VEGFR) (with agents such as bevacizumab, sunitinib and thalidomide), EGFR (gefitinib and cetuximab), platelet-derived growth factor receptor (PDGFR) (imatinib), clusterin (OGX-011 or custirsen) and immunotherapeutics (Sipuleucel-T and Ipilimumab).60–72 With all agents, results have been variable, but most promising with targeting of clusterin and immunomodulation; however, they raise important and unresolved issues in regards to appropriate lengths of treatment, and need for predictive biomarkers of response in the setting of prohibitive costs.
A paucity of representative pre-clinical models related to early human prostate cancer makes it attractive to study a drug’s effects in the ‘window’ prior to radical therapy. Ongoing clinical studies from several groups, including ours, may provide further insights (see Table 1). NCT00430183 is a large (>700 patients) study which has completed recruitment and will compare the outcome for patients who have been treated with neoadjuvant docetaxel. The other studies listed are mostly smaller, Phase 1 and 2 studies looking for signals of activity. For example, in addition to the data from the prostate TCGA described above, aberrant PI3k pathway signalling has been detected in 42% of primary and 100% of metastatic prostate cancers.73,74 Loss of PTEN and activation of the PI3k/mTOR pathway are observed in aggressive primary disease.75,76 The effects in prostate cancer tissue of rapamycin (an mTOR1 inhibitor) have been studied. The drug was safe and inhibited mTORC1 signalling; however, no effects on tumour proliferation were detected. 77 The CaNCaP02 study (Table 1) is investigating the pharamcodynamic effects of AZD2014 (a dual mTORC1 and 2 inhibitor) for men with intermediate- or high-risk prostate cancer. Inhibition of both mTOR complexes may potentially offer improved therapeutic advantages, and results are awaited.
Recruiting neoadjuvant studies (from www.clinicaltrials.gov, accessed December 2015).
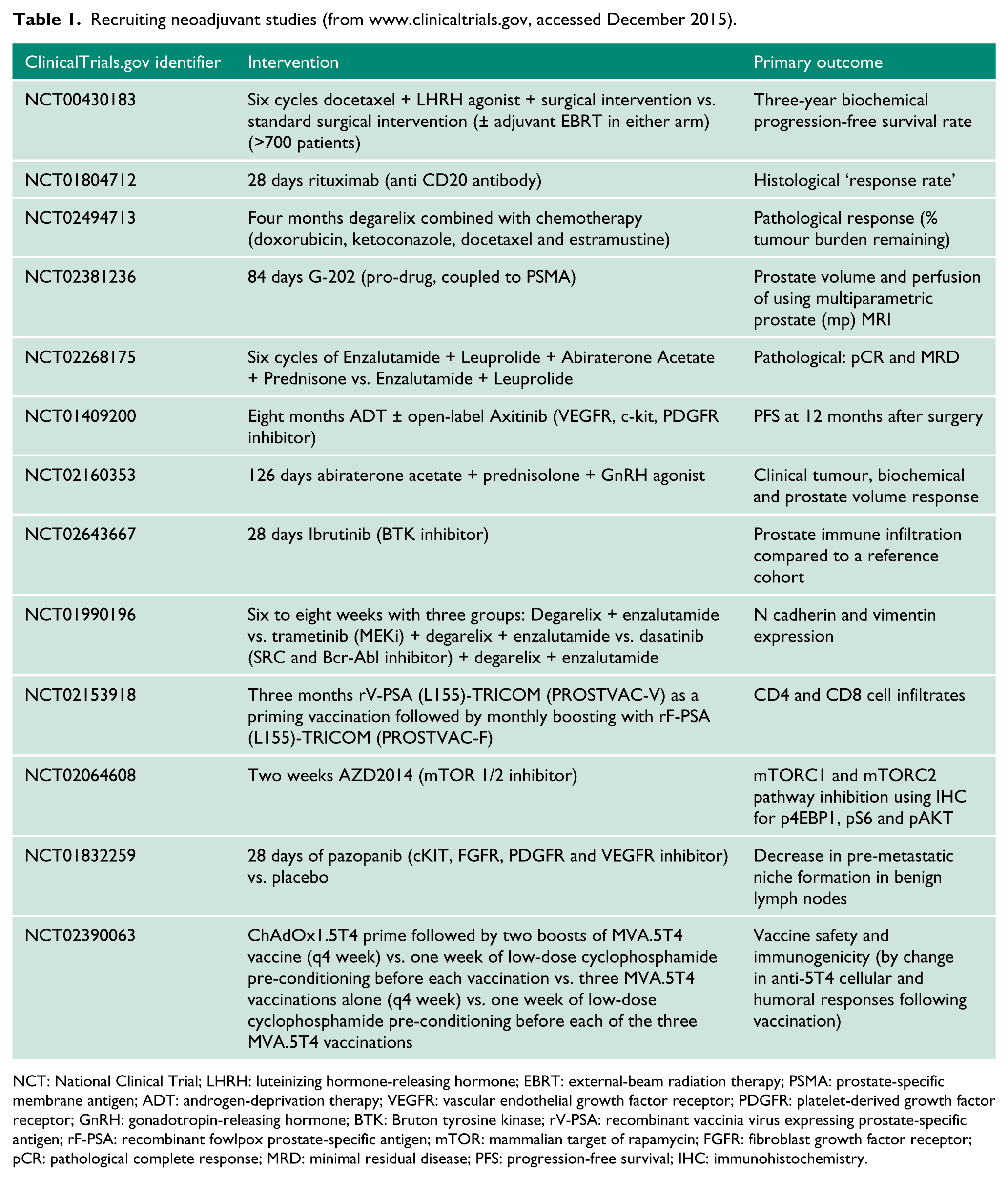
NCT: National Clinical Trial; LHRH: luteinizing hormone-releasing hormone; EBRT: external-beam radiation therapy; PSMA: prostate-specific membrane antigen; ADT: androgen-deprivation therapy; VEGFR: vascular endothelial growth factor receptor; PDGFR: platelet-derived growth factor receptor; GnRH: gonadotropin-releasing hormone; BTK: Bruton tyrosine kinase; rV-PSA: recombinant vaccinia virus expressing prostate-specific antigen; rF-PSA: recombinant fowlpox prostate-specific antigen; mTOR: mammalian target of rapamycin; FGFR: fibroblast growth factor receptor; pCR: pathological complete response; MRD: minimal residual disease; PFS: progression-free survival; IHC: immunohistochemistry.
Additional, more immediately actionable opportunities for targeted therapy might exist. An estimated 19% of primary prostate cancers have defects in ‘DNA repair pathways’. Exciting data from the ‘TOPARP’ study 78 confirmed olaparib (PARP inhibitor) treatment was clinically effective when given to men with metastatic CRPC, selected on the basis of defects in DNA repair genes (including BRCA1/2, ATM, Fanconi’s anaemia genes, and CHEK2). A further window study, using olaparib (CaNCaPO3), has been developed and is scheduled to open to recruitment later in 2016.
It is worth noting the variety of endpoints that are employed within the studies listed in Tables 1 and 2. One of the challenges for investigators in this field remains defining and obtaining consensus on what are adequate surrogate endpoints for prostate cancer relapse, or alternatively, clinically relevant endpoints such as OS will have to be used (even if the studies take longer to complete). Surrogate endpoints such as pathological complete response (pCR) rate, validated in other solid tumours to correlate with improved survival, have not been proven in prostate cancer. 17 Advances in technology may improve this situation; for example, it is possible to measure circulating tumour DNA (ctDNA) in a variety of clinical settings including prostate cancer. With further refinement it will be interesting to see if measuring ctDNA, or perhaps another circulating marker, might more adequately monitor the response to drug treatment.
Recruiting adjuvant studies (from www.clinicaltrials.gov, accessed December 2015).
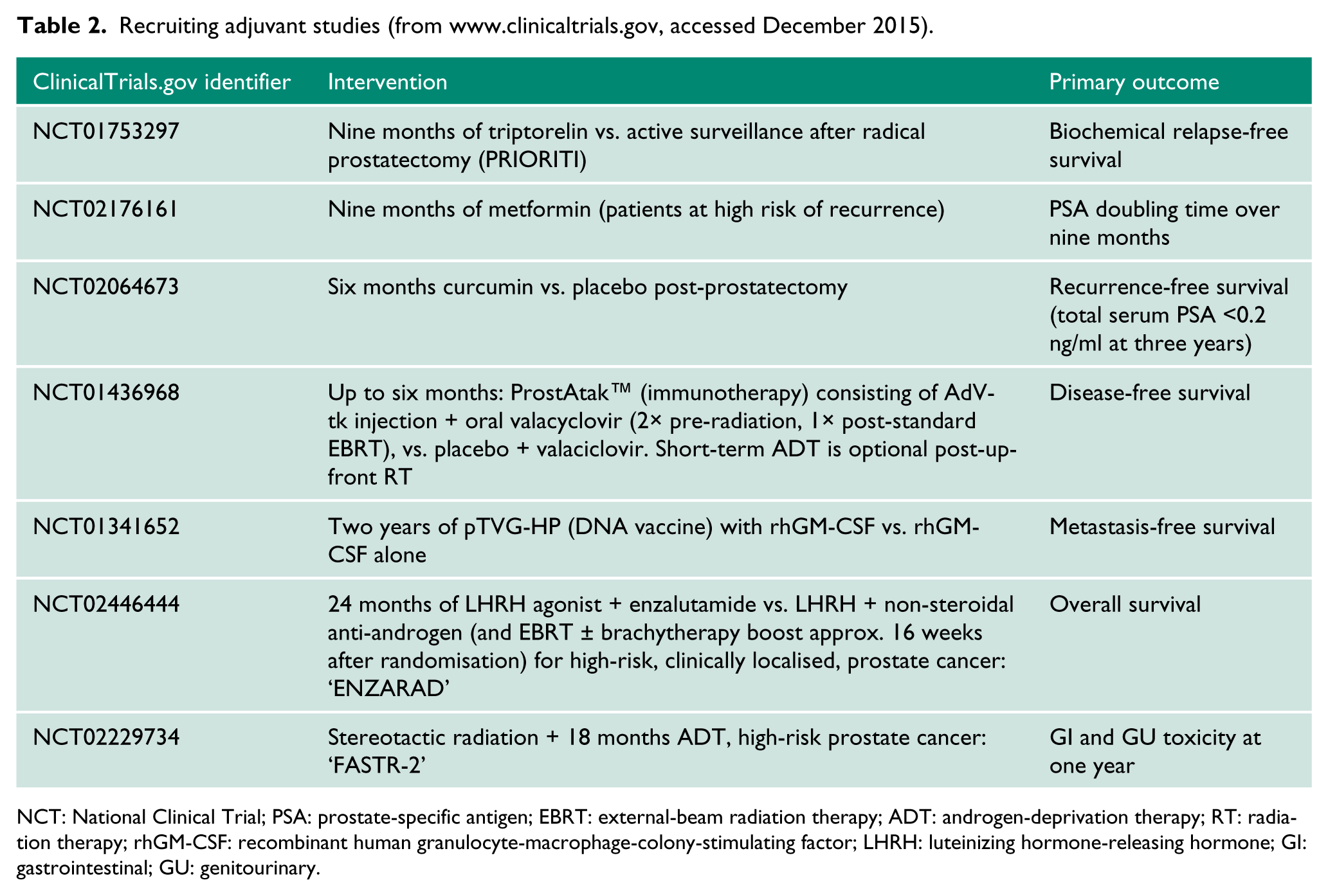
NCT: National Clinical Trial; PSA: prostate-specific antigen; EBRT: external-beam radiation therapy; ADT: androgen-deprivation therapy; RT: radiation therapy; rhGM-CSF: recombinant human granulocyte-macrophage-colony-stimulating factor; LHRH: luteinizing hormone-releasing hormone; GI: gastrointestinal; GU: genitourinary.
Conclusion
As the incidence of primary prostate cancer rises in the United Kingdom, 79 the detection of men with high-risk non-metastatic prostate cancer and their subsequent management is becoming increasingly important. Over the last decade, there has been a significant shift in the management of prostate cancer, including studies that confirm the benefits of radical treatment in a number of publications. 80 Building on results for men with CRPC, docetaxel has recently been proven active for men with hormone-sensitive prostate cancer and the results of studies with more recently approved drugs for prostate cancer in the (neo)adjuvant setting are awaited. Furthermore, advances in the biological understanding of prostate cancer and novel drug development will hopefully broaden the armamentarium beyond agents proven or predicted to be effective in CRPC.
While it is clear that early, radical treatment of primary prostate cancer is very effective, it remains difficult to identify those patients who are likely to relapse and to treat them appropriately. 56 Further risk stratification, for example, utilising molecular features, could potentially help distinguish indolent from aggressive prostate cancer, ultimately providing biological markers that could guide a more personalised approach to therapy selection.
Key points
An increasing proportion of men diagnosed with prostate cancer in the United Kingdom are presenting with non-metastatic disease.
Early treatment of primary prostate cancer is very effective, and radical treatment has been clearly shown to be beneficial in this group of patients in a number of publications.
As yet, there continues to be no molecularly targeted or chemotherapeutic options with proven, statistically significant survival benefit in this setting.
Identification of men with prostate cancer that is likely to relapse and to treat them appropriately remains an unmet clinical challenge. However, there are indications that further risk stratification using molecular features could potentially help distinguish indolent from aggressive prostate cancer.
Using molecular features to personalise treatment could allow us to optimise precision treatment of primary prostate cancer.
Footnotes
Acknowledgements
None.
Conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
Not applicable.
Informed consent
Not applicable.
Guarantor
SP.
Contributorship
Both SSK and SP researched the literature and analysed the current evidence. SSK prepared the first draft of the manuscript. Both SSK and SP reviewed and edited the manuscript and approved the final version of the manuscript.