
Abstract
Since Partin introduced the analysis of prostate-specific antigen, clinical T-stage and Gleason scores to estimate the risk of progression in men with localised prostate cancer, our understanding of factors that modify this risk has changed drastically. There are now multiple risk stratification tools available, including look-up tables, risk stratification/classification analyses, regression-tree analyses, nomograms and artificial neural networks. Concurrently, descriptions of novel biopsy strategies, imaging modalities and biomarkers are frequently published with the aim of improving risk stratification. With an abundance of new information available, incorporating advances into clinical practice can be confusing. This article aims to outline the major novel concepts in prostate cancer risk stratification for men with biopsy confirmed prostate cancer. We will detail which of these novel techniques and tools are likely to be adopted to aid treatment decisions and enable more accurate post-diagnosis, pretreatment risk stratification.
Introduction
Prostate cancer is the most common male solid cancer in the world. In developed countries prostaqte-specific antigen (PSA) testing/screening has increased our estimates of incidence. 1 In the UK, the incidence of localised prostate cancer at presentation has increased over the last decade, while the rate of metastatic disease at presentation has decreased. 2 However, the impact that PSA testing and subsequent treatment of localised disease has had on prostate cancer-specific mortality (PCSM) is questionable3,4 and there is therefore a drive to manage men with less invasive therapy or surveillance alone. 5 Risk stratification tools have repeatedly been shown to outperform clinicians at identifying the correct men in whom to pursue these more conservative management strategies. 6
New classification systems
Caras and Sterbis grouped risk stratification tools into those predicting the likelihood of cancer before biopsy, those predicting the behaviour of biopsy-confirmed cancer after diagnosis but, before treatment or surveillance, and nomograms predicting behaviour after treatment. 7 This article will focus on approaches to risk stratification of men with biopsy-confirmed prostate cancer, prior to treatment.
Currently, men with localised prostate cancer are risk stratified according to their PSA at diagnosis, clinical stage and Gleason grade at biopsy. In the UK, the National Institute for Health and Care Excellence (NICE) has published a scoring system that groups men according to the risk of prostate cancer recurrence following treatment. In brief, there are three groups: low-risk, for men with a PSA less than 10 ng/ml, Gleason score of 6 or less and clinical stage T1–T2a; the intermediate-risk group for men with a PSA of 10–20 ng/ml, Gleason score of 7, or clinical stage T2b; and a high-risk group for men with a PSA greater than 20 ng/ml, Gleason score of 8–10 or clinical stage T2c or greater. However, these guidelines draw on studies that have never been assessed against PCSM. Indeed, the PSA cut-off points are replicated from D’Amico’s work in 1998, using biochemical recurrence (BR) as a surrogate for aggression, which does not always predict PCSM.8,9 Another early attempt at allocating risk, the Kattan nomograms, predicted the presence of indolent cancers based on a study of clinical stage, Gleason grade, PSA and cancer volume in biopsy specimens. 10 However, the majority of patients in this study underwent radical prostatectomy and again outcomes were measured against BR. Furthermore, clinical staging has not consistently been shown to associate with PCSM in the UK. For example, although Reese et al. demonstrated that clinical staging predicted BR after radical prostatectomy in American men, 11 Selvadurai et al. showed that clinical staging could not predict adverse histology on repeat biopsy for UK men undergoing active surveillance. 12 There have been no UK based studies to show that the above criteria can predict PCSM. Despite this, with some relatively minor changes, the above clinical parameters are incorporated in over 20 risk stratification tools. 13 Many of these tools are validated in populations of men outside the UK, who are undergoing radical prostatectomy and are measured against surrogate markers other than PCSM.
In 2005 Cooperberg et al. described the cancer of the prostate risk assessment (CAPRA) score. 14 The score indicates risk on a 1–10 scale by using age and PSA at diagnosis, the percentage of biopsy cores which contain cancer, Gleason score at biopsy and clinical stage to assign points. Although the score was initially validated against predicting BR following radical prostatectomy, it has subsequently been shown to predict the risk of bone metastases and PCSM in over 10,000 American men with localised cancer considering all treatment options. Cooperberg et al. showed that for each increase in CAPRA score, there was a statistically significant increased risk of prostate cancer-specific morbidity or mortality. 14 However, only 6% of men undertook active surveillance/watchful waiting in their cohort, despite 49% of patients having a CAPRA score of 2 or less.
National and international consortia have also acted on evidence to suggest that increasing the number of risk categories can improve pretreatment risk stratification. The National Comprehensive Cancer Network (NCCN) has recently updated its risk stratification guidelines to incorporate the amount of disease present in prostate biopsy cores and include a new very low-risk group. The purpose of the very low-risk group is to highlight patients who are suitable for surveillance strategies rather than aggressive treatment. The drive for creation of the new group came from studies such as that conducted by Miller et al., showing that approximately 40% of cancers diagnosed in the USA were over-treated. 15 Furthermore, in 2008 Beasley et al. showed that splitting the intermediate group into low-intermediate and high-intermediate groups also improved pretreatment risk stratification. 16 However, these conclusions were due to the high-intermediate group having reduced BR rates when given adjuvant androgen deprivation therapy while the low-intermediate group received no benefit.13,16
NICE, therefore, highlights that clinical risk stratification tools may not be representative of outcomes in the UK, not least because of the differences between PSA screened populations and ours, and differences in the way men are treated. 17 A recent study from our institution has addressed this and tested the NICE risk groups and a new model in a large UK population. This study demonstrated poor concordance for the NICE groups in predicting PCSM but a significantly improved performance by using a more refined risk stratification system. 18
Imaging
With advances in magnetic intensity and functional multiparametric imaging (mpMRI), including dynamic contrast enhanced sequences, diffusion weighted imaging (MR-DWI), magnetic resonance spectroscopy (MRS) and dynamic contrast enhanced MRS, the usefulness of magnetic resonance imaging (MRI) has increased drastically. However, variations in protocols and a lack of diagnostic criteria have impeded the widespread adoption of mpMRI. The recent joint publication of the prostate imaging – reporting and data system version 2 by the American College of Radiology and European Society of Uroradiology will help standardise the acquisition, interpretation, and reporting of prostate mpMRI 19 enabling MRI to be incorporated in the pretreatment prostate cancer pathway to assess the stage and risk of localised prostate cancer. 20
Using MRI, Somford et al. were able to predict extra-prostatic extension at radical prostatectomy in a cohort of 183 men accurately in 73.8% of cases, with negative predictive value highest in men in the low-risk group. 21 Subsequently, Marcus et al. described the addition of mpMRI to the NCCN risk stratification tool and found that MRI correctly upstaged 12/71 men. Interestingly, the majority of upstaged patients were previously classified as intermediate risk. 22
Moreover, the apparent diffusion coefficient (ADC), calculated from DW-MRI, has been shown to correlate with prostate cancer aggression23–25 and Hambrook et al. demonstrated that MR-DWI was able to identify prostatic lesions that were more representative of final pathology following prostatectomy when compared to standard 10-core transrectal ultrasound-guided (TRUS) biopsy. 26 The use of MRI to risk-stratify prostatic lesions non-invasively is exciting; however, at present ADC values were not significantly discriminative for tumours in the transition zone or for low-risk tumours20,23 but further investigation is warranted.
Biopsy approach
Currently, 10–12-core TRUS biopsy is standard practice in the initial biopsy setting, despite having been shown to miss around 30–45% of prostate cancers.27–29 Saturation (>20 cores) rectal or transperineal biopsies have been advocated to improve the accuracy of clinically significant prostate cancer diagnosis. However, in a systematic review, Eichler et al. demonstrated that the addition of further cores (18–24) did not detect significantly more cancers and may have a poorer side effect profile, 30 and a survey of urologists in the UK revealed that saturation biopsy is infrequently used in the initial biopsy setting. 17 Advances in mpMRI have led to an increasing adoption of MRI-guided biopsies to improve cancer detection and subsequent risk stratification. Pinto et al. used fusion MRI-guided biopsies to demonstrate an improved efficiency of diagnosis (fewer number of cores needed to detect prostate cancer), although the authors were unable to demonstrate a change in the rate of detection. 31 In 2013, Moore et al. conducted a systematic review of MRI-guided biopsies and standard TRUS biopsy and similarly revealed no difference in the detection of clinically significant cancer while confirming the ability of MRI-guided biopsies to detect cancer with fewer cores. 32 These initial results are exciting but mixed and require further investigation. In particular, studies determining the value of MRI-guided biopsy compared with TRUS biopsy in relation to long-term outcomes are needed.
Histological classification
Since 1966, the Gleason grading has summed the two most common grade patterns, each scored from 1 to 5 according to glandular architecture, to produce a Gleason score. In 2005 the International Society of Urological Pathology (ISUP) updated the Gleason scoring system. 33 The 2005 ISUP changes were broadly aimed at limiting the scope of glandular architecture pattern 3 while widening the scope of pattern 4.33,34 Therefore cancers that were previously graded 3 were subsequently graded as 4. Indeed, Greenburg et al. demonstrated that the adoption of 2005 ISUP scoring led to an increased incidence of intermediate and high-risk prostate cancer while low-risk prostate cancer incidence remained stable in the UK. In 2014, the ISUP committee updated guidelines to grade prostate cancer, largely to overcome the fear that patients had when assigned a cancer diagnosis but with a Gleason score of 6. 35 The novel grade groups assigns a prognostic score of 1–5 according to the glandular pattern (see Table 1). The lead author showed these groups to be a more accurate predictor of BR in American men undergoing radical treatment. 36 Most recently, we proposed a new risk stratification system incorporating PSA at diagnosis, clinical T stage and the novel ISUP grouping system, which improved the prediction of PCSM in a new diagnosis cohort of UK men. These findings were based on a cohort of 10,139 men with 789 prostate cancer deaths over a median of 6.9 years. 18
ISUP 2014 scores with their equivalent Gleason score and associated glandular appearance.
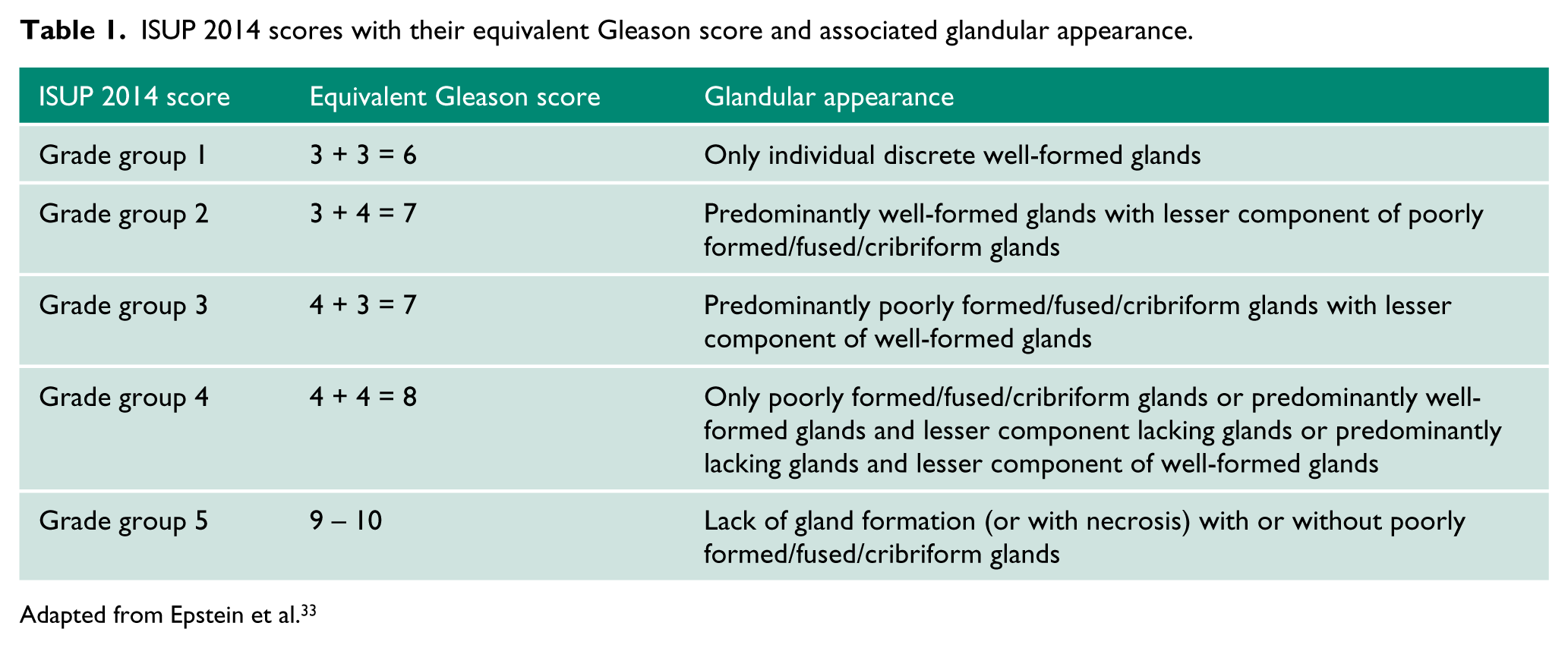
Adapted from Epstein et al. 33
Biomarkers
Numerous prognostic immunohistochemical biomarkers have been proposed for use at the prostate biopsy stage. However, the majority were developed using prostatectomy cohorts (and often prostatectomy specimens), with biochemical recurrence as the endpoint. 37 Despite this, Ki67, a marker of cellular proliferation, has shown promise. 38 Staining for Ki67 has been shown to be predictive of PCSM in both surgically 39 and radiotherapy 40 treated men and predictive of the need for intervention in men undergoing active surveillance, 41 although the numbers were small. Further larger studies are required to validate and incorporate immunohistochemical markers into risk stratification of men at diagnosis.
The use of genetic analysis to predict outcomes in prostate cancer is actively being investigated. Again, many studies use prostatectomy samples, in which the amount of tissue available makes genetic analysis easier, to develop assays. Through advances in genetic analysis and polymerase chain reaction methods, we now have the capability to detect genetic variants from small amounts of material found in biopsy specimens, and several diagnostic aids are available, for example, Oncotype Dx, 42 Prolaris, 43 Dechipher, 44 etc. Many of these assays assess the likelihood of aggressive cancer by analysing the expression of genes from isolated RNA.
In 2015, Cullen et al. used the Oncotype Dx assay to assess the expression of 12 cancer-related genes from biopsy extracted RNA in 93% of 431 racially diverse men with intermediate (or less) NCCN risk stratification. 45 An increasing assay score (on a scale from 0 to 100) predicted adverse final pathology, BR and metastatic recurrence with hazard ratios per 20 score units of 3.3, 2.9 and 3.8. However, the number of men who developed metastasis was small (n=5). 45 Klein et al. utilised the Decipher test consisting of a 22-gene panel RNA analysis in 57 men who underwent prostatectomy who were followed up for 8 years. 44 The Decipher test reclassified 46% of men from their NCCN classification. However, again, the number of events was low (8/57) and when Decipher’s results were analysed in isolation, the number of men who developed metastasis with Decipher low, medium and high-risk scores were one, five and two. 44 This raises the important question of how best to incorporate novel markers to clinical risk stratification strategies. In 2013, Cooperberg et al. demonstrated the importance of combining the Prolaris cell-cycle–progression (CCP) score with the CAPRA score. In a cohort of 413 American men undergoing prostatectomy, the authors found that the combined CCP-CAPRA score had an improved ability to predict BR, when compared to the CCP score or the CAPRA score alone. 46 However, they were not able to assess PCSM or clinical metastasis due to the low number of events and used the CCP score from only the dominant region of the prostate gland.
Clearly more work needs to be done, not least in diversifying the patient populations in which biomarker studies have been conducted. An additional major challenge will be to take our understanding of the above risk stratification criteria, borne out of our experience in treating all-comers with prostate cancer, and relate this to our novel understanding of prostate cancer as a highly heterogeneous cancer, with five 47 or indeed seven 48 distinct molecular subtypes.
Summary
Risk stratification of men at a pretreatment stage is becoming increasingly important and the era of using Gleason grading, PSA and clinical staging alone to stratify men into one of three risk categories is coming to an end. Novel risk stratification tools will aim to classify men into five (or more) categories including a very low-risk group, and the splitting of the intermediate-risk group into an intermediate low and intermediate high-risk group.13,18 In the near future one can envisage the incorporation of additional information, including MP-MRI findings and genomic profiling scores to stratification tools, resulting in more accurate risk stratification, leading to improved decision making at the pretreatment stage.
Footnotes
Acknowledgements
None.
Conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
Not applicable.
Informed consent
Not applicable.
Guarantor
VJG.
Contributorship
KMP and VJG researched the literature. VJG conceived the study. Both authors reviewed and edited the manuscript and approved the final version of the manuscript.