
Abstract
Prostate-specific antigen (PSA) is widely used as a biomarker in the detection of prostate cancer and for decision making regarding treatment options, response to therapy, and clinical follow-up. Despite its widespread use, it is well recognised that PSA has suboptimal performance as a screening tool due to poor specificity, resulting in high negative biopsy rates and potential ‘over-diagnosis’ and ‘over-treatment’ of clinically insignificant cancers. In particular, PSA does not reliably distinguish either cancer from benign prostatic conditions, or ‘clinically significant’ from ‘indolent cancers’, and it is inaccurate in predicting disease burden and response to treatment. There is an urgent demand for novel biomarkers to address these clinical needs. This article provides an update on the novel candidate biomarkers in development, which have shown potential for improving the detection of clinically significant cases of this malignancy.
Introduction
Over 40,000 new prostate cancer cases are diagnosed annually in the United Kingdom (UK), and there are 10,000 prostate cancer-related deaths. 1 There are particular challenges to overcome regarding appropriate detection in individuals where treatment is warranted, whilst avoiding morbidity from unnecessary invasive investigations and treatment of ‘insignificant cancer’. ‘Over-diagnosis’ and ‘over-treatment’ of prostate cancer are well-recognised phenomena, and efforts are being made to minimise the numbers of men undergoing radical treatment if their tumour is unlikely to pose a threat. A particular challenge is to accurately predict the potential aggressiveness of newly diagnosed prostate cancer despite adjuncts such as the D’Amico Risk Classification. 2 Each of these areas of clinical need may benefit from novel prostate cancer biomarkers with performance characteristics surpassing those of prostate-specific antigen (PSA).
Principles of prostate cancer biomarkers
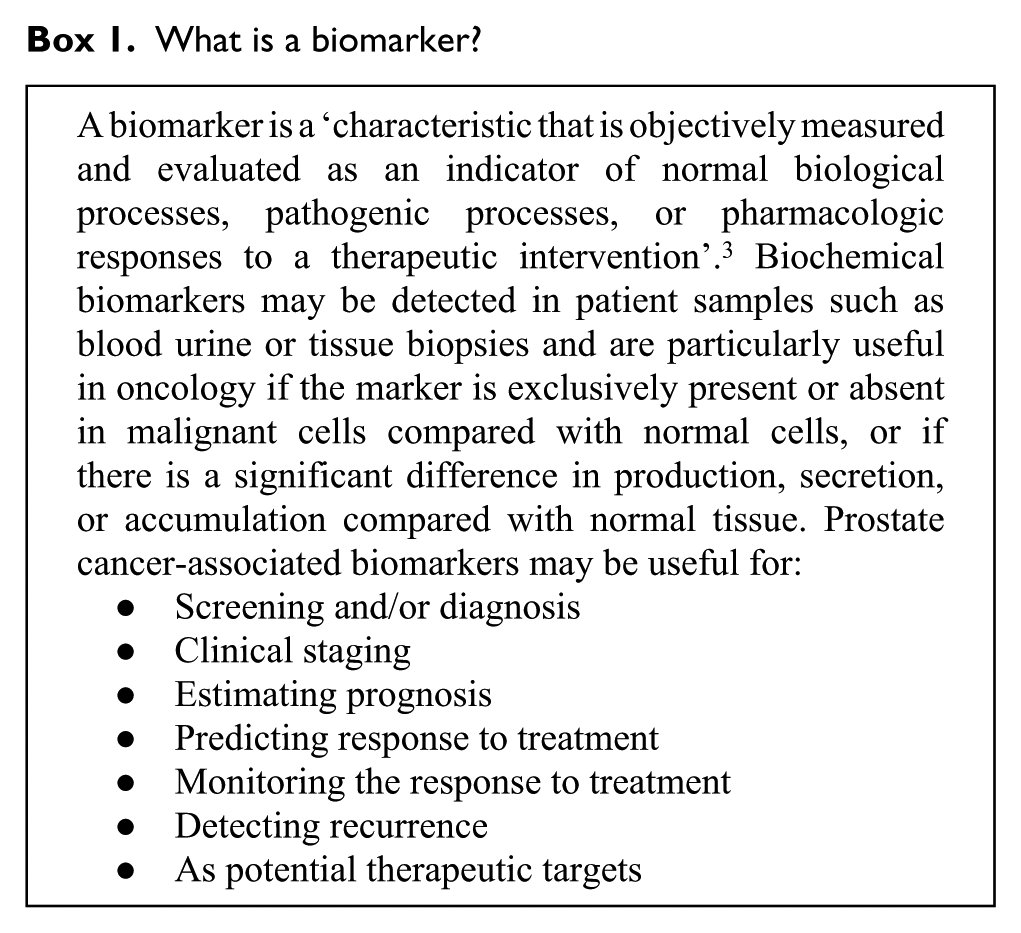
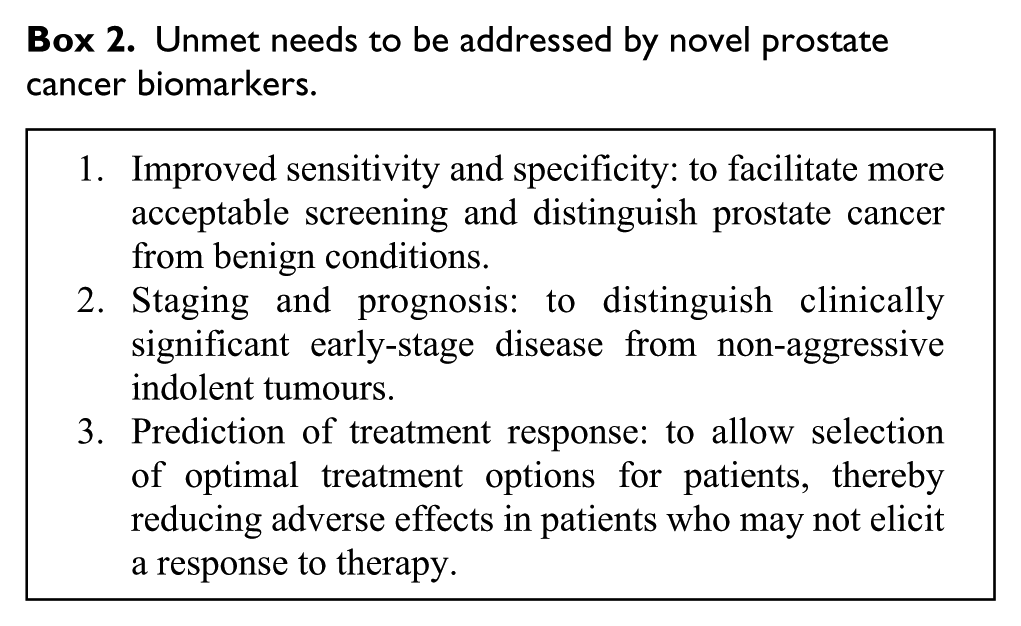
In cancer management, biomarkers may be used as indicators of the underlying disease state (Box 1). 3 An ideal biomarker test should be safe, easy to perform, acceptable to the patient, inexpensive and reproducible. There are particular unmet clinical needs with regards to prostate cancer detection (Box 2) including distinction of malignant from benign causes of a raised PSA, distinction of ‘clinically significant’ early-stage disease from ‘insignificant’ indolent tumours, and the prediction of response to treatment. Novel prostate cancer biomarkers need to provide improvements in these areas in order to prove clinically useful. This will be met only through rigorous pre-clinical studies and clinical evaluation prior to widespread use. A PubMed search of the term ‘prostate cancer biomarker’ reveals over 29,000 peer-reviewed publications, but to date few novel prostate cancer biomarkers are close to replacing PSA in regular clinical use. Numerous potential candidate biomarkers have been proposed (Table 1) including proteins and nucleic acids, and these can be detected with minimally invasive tests on urine or blood samples, or on tissue samples.
Prostate cancer biomarkers in clinical use and in development.
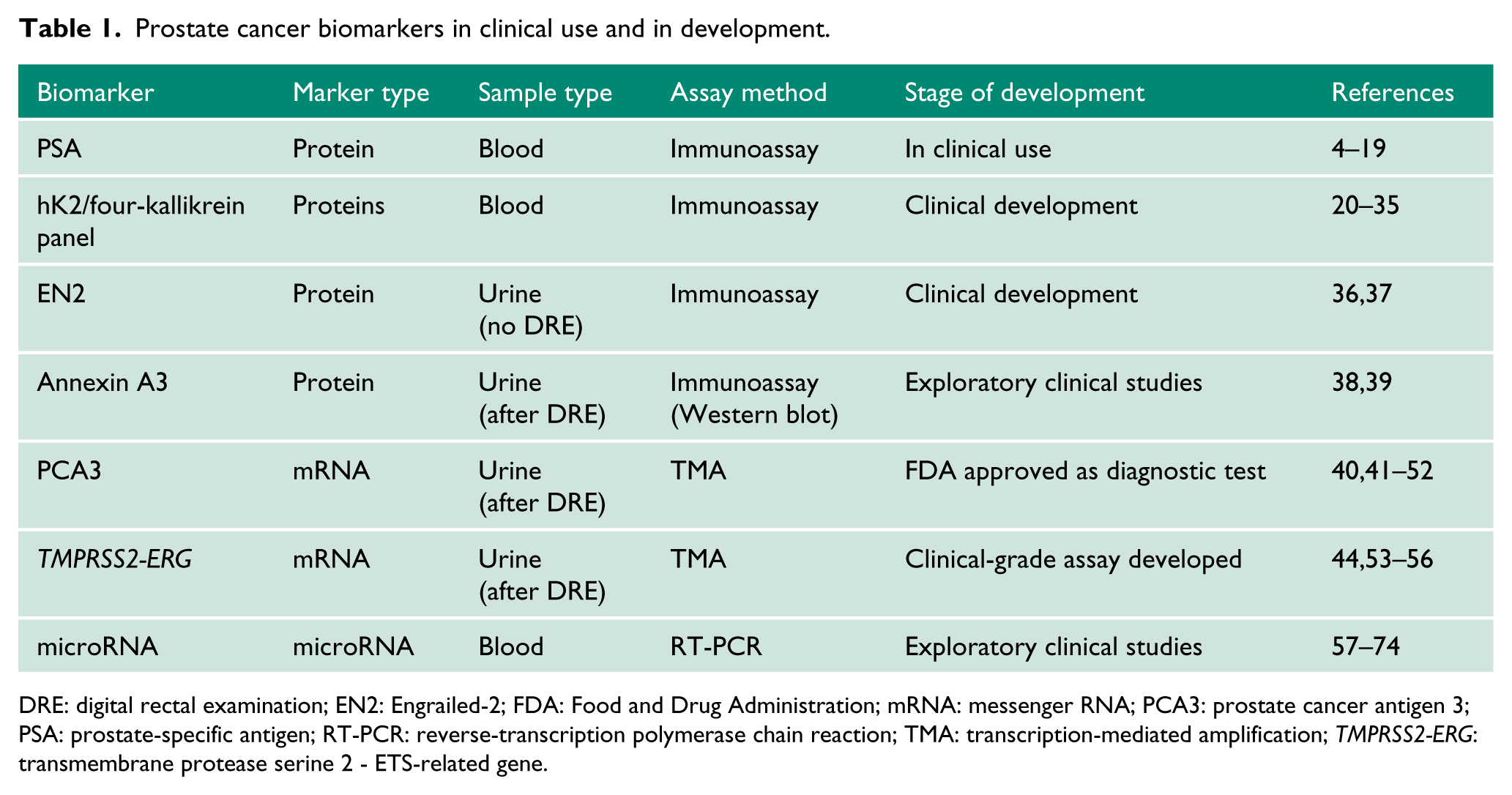
DRE: digital rectal examination; EN2: Engrailed-2; FDA: Food and Drug Administration; mRNA: messenger RNA; PCA3: prostate cancer antigen 3; PSA: prostate-specific antigen; RT-PCR: reverse-transcription polymerase chain reaction; TMA: transcription-mediated amplification; TMPRSS2-ERG: transmembrane protease serine 2 - ETS-related gene.
What is a biomarker?
Unmet needs to be addressed by novel prostate cancer biomarkers.
PSA
The discovery and purification of prostate-specific antigen (PSA) in 1979 75 revolutionised prostate cancer detection and management. PSA (human kallikrein 3, hK3, KLK-3) is a serine protease secreted by prostate epithelial cells into seminal fluid where it liquefies the ejaculate. 76 PSA is normally present at low concentrations in blood 77 but can be elevated by benign conditions and prostate cancer. Following United States (US) Food and Drug Administration (FDA) approval in 1986, PSA testing was used to monitor treatment response and identify disease relapse,78,79 and it has subsequently been used for prostate cancer detection, screening, staging and risk-stratification. In 1994 PSA was FDA approved for prostate cancer diagnosis, and this greatly increased testing in asymptomatic men with 35%–40% of men aged >65 years in the US undergoing testing by 1994. 80 Half of men aged 65–79 now undergo PSA screening in the US,81–83 and a million prostate biopsies are performed annually. 84
PSA testing has caused a stage-shift towards more newly diagnosed tumours being organ-confined, and PSA testing may be partly responsible for improving mortality rates. However, PSA-based screening can cause harms including ‘over-diagnosis’ and ‘over-treatment’ of ‘clinically insignificant’ tumours. As PSA is tissue-specific rather than cancer-specific, it has a poor specificity and positive predictive value particularly at ‘borderline’ PSA values of 3–10 ng/ml where the negative biopsy rate can be 60%–75%. 4 It is difficult to determine an absolute PSA threshold to trigger a biopsy; a substantial proportion of men with a PSA below 4 ng/ml, for example, have prostate cancer, and there is no threshold below which there is no risk of cancer.5,6 Several PSA refinements have been investigated including free/total PSA ratio 4 and PSA velocity.7–10
Whilst PSA testing can be used in screening programmes, the balance between benefits and adverse effects of PSA-based screening means further optimisation is necessary,11,12 and the numbers of men needed to screen and treat to save one life are currently unacceptably high. 13 The Göteborg Screening Trial suggests that PSA-based screening may appear more beneficial with longer follow-up; 14 however, in 2015 the UK National Screening Committee maintained its position to not recommend screening for prostate cancer. 15 Recent evidence suggests PSA might be an early indicator of risk of developing lethal prostate cancer many years before diagnosis, and a single PSA test at age 44–49 can risk-stratify patients at greatest risk of future clinically significant disease and identify these men for subsequent screening. 16 The PSA level at diagnosis is associated with tumour volume, stage and Gleason grade,17,78 therefore PSA combined with other factors can risk-stratify patients upon diagnosis.11,18,19 However, it is clear that there is a need for improved biomarkers above and beyond PSA.
Novel protein biomarkers
Most of the potentially novel prostate cancer biomarkers evaluated to date are proteins. Their quantification in blood samples involves relatively simple low-cost sample processing and well-established immunoassays such as enzyme-linked immunosorbent assay (ELISA). Well-performing protein biomarkers in blood samples are relatively uncommon, whilst biomarkers that necessitate evaluation in tissue samples are generally impractical for widespread pre-diagnostic use.
Additional kallikrein proteins
In addition to PSA, over a dozen other human kallikrein proteins have been identified, several of which have been evaluated as prostate cancer biomarkers. Of these, human kallikrein 2 (hK2) has reached the farthest stage of clinical development. hK2 is a serine protease which converts inactive pro-PSA to active PSA, and shares 80% of its primary structure with PSA.85,86 In contrast to PSA, hK2 is expressed more highly in malignant cells than benign epithelial cells, particularly in high-grade disease.20–24 Clinical studies suggest serum hK2 may help discriminate malignant from benign causes of a raised PSA.24–27
Recently there has been interest in developing a combined panel of kallikreins for prostate cancer detection and screening. 28 A panel of four kallikrein markers (total PSA, free PSA, intact PSA, and hK2) outperforms PSA testing in accurately detecting prostate cancer, and can potentially reduce the number of unnecessary false-negative biopsies undertaken in men with a raised PSA.29–34 For example an evaluation of the performance of the four kallikrein panel in the Prostate Testing for Cancer and Treatment (ProtecT) study in the UK demonstrated that use of this panel may potentially halve the number of unnecessary biopsies performed on men with an elevated PSA whilst missing only very few high-grade cancers. 35 This could therefore reduce the adverse effects of over-detection of low-risk, low-volume tumours.
An additional novel approach to improve the performance of PSA-based screening is to combine the results of three blood tests (tPSA, fPSA and [−2]proPSA) using the mathematical formula ([−2] proPSA/fPSA) × √tPSA) to calculate the ‘Prostate Health Index’ (phi). The phi result can improve the rate of prostate cancer detection compared with either tPSA or f/tPSA alone.87–94 Given the significant cost, invasiveness and potential adverse effects of undergoing a prostate biopsy, use of a multiple kallikrein panel may improve the cost-benefit ratio of a prostate cancer screening programme, and may replace PSA testing. Large-scale prospective evaluation of these panels of kallikrein markers is warranted.
Other protein biomarkers
Other protein biomarkers for prostate cancer are under evaluation (Table 1). Engrailed-2 (EN2) is a HOX gene family transcription factor expressed exclusively in malignant prostate tissue 36 and detectable in urine samples with a reported sensitivity and specificity of 66% and 88%, respectively, 36 and levels correlate with tumour volume and stage. 37 Annexin A3 is a calcium-binding protein reported to have a superior diagnostic performance than PSA when measured in urine samples following prostatic massage, thereby potentially reducing unnecessary biopsy in men with a PSA of 2–10 ng/ml.38,39 Further prospective evaluation of these and other potential novel prostate cancer biomarkers is needed before any of them may replace PSA testing in clinical practice. In particular, for any of these potential biomarkers to surpass PSA they will need to demonstrate improved performance detecting clinically significant cancers, rather than simply outperforming PSA with regards to the detection of any-grade prostate cancer.
RNA biomarkers
Abnormal gene expression is a hallmark of cancer, manifesting as either abnormal levels or mutated forms of messenger ribonucleic acid (mRNA) or non-coding microRNAs (miRNA) and long non-coding RNA (lncRNA). RNA can be detected in serum, urine or tissue samples.95,96 Quantification of RNA biomarkers is more complex and costly than for proteins, and detection and quantification requires reverse-transcription polymerase chain reaction (RT-PCR), therefore RNA assays are not commonly used in clinical practice. RNA is unstable and degrades quickly in bodily fluids, therefore patient samples require rapid processing. Transcription-mediated amplification assays have recently been developed for some RNA biomarkers and have the advantage of simpler sample processing procedures and assay protocols, providing greater feasibility for use in the clinic.40,53
Prostate cancer antigen 3 (PCA3)
PCA3 is a prostate-specific non-coding mRNA over-expressed by prostate cancer cells compared with benign prostate epithelium. 41 PCA3 is readily detected in fresh voided urine samples following prostatic massage. 42 A clinical-grade transcription-mediated amplification assay, ‘Progensa® PCA3’, gained FDA approval in 2012 and can be used to aid decision making regarding repeat biopsy in men with a previous negative biopsy. 40 While PCA3 has a better diagnostic performance than PSA,43–45 and its use may reduce the number of unnecessary biopsies,46,47 it does not add predictive value for Gleason score or tumour stage.48,49 In direct comparisons, the phi is a better predictor of significant prostate cancer at initial biopsy, and therefore more suitable for screening.50–52
Transmembrane protease serine 2 (TMPRSS2)-ERG fusion
Approximately half of all prostate cancers contain a chromosomal rearrangement resulting in fusion of the TMPRSS2 gene with the v-ets erythroblastosis virus E26 oncogene (ERG). 54 The resulting TMPRSS2-ERG gene fusion may play a role in the development of invasive prostate cancer. 55 The TMPRSS2-ERG mRNA transcript is detectable in urine after prostatic massage with a reported specificity of >90% for prostate cancer.53,56,97 A pre-biopsy TMPRSS2-ERG ‘score’ incorporating urinary TMPRSS2-ERG mRNA and PSA mRNA measurement has been associated with tumour volume and Gleason grade at subsequent biopsy and prostatectomy.53,56 A recent prospective multicentre evaluation demonstrated that measurement of pre-biopsy urinary TMPRSS2-ERG adds additional predictive value to both the ERSPC risk calculator and PCA3 in both the diagnosis of prostate cancer and prediction of Gleason score and clinical stage. 44
miRNA biomarkers
miRNA are non-coding single-stranded RNA 18–25 nucleotides long which regulate gene expression. Numerous miRNA are over- or underexpressed in prostate cancer, and these miRNA expression profile changes may be associated with epithelial-to-mesenchymal transition, cellular migration and invasion, angiogenesis, and metastasis.57,58 As a result of their small size, miRNAs are resistant to endogenous ribonucleases, and can be detected by RT-PCR in plasma, serum and urine samples.80,82 miRNA profiling of serum samples may therefore be clinically useful in distinguishing aggressive from non-aggressive cancers.
Studies have shown that miRNA profiles can distinguish men with localised prostate cancer, men with metastatic disease, and control individuals.59–70 However, these studies have primarily involved relatively small numbers of patients, and to date no large prospective evaluation of miRNA performance has been reported. Moreover, there have been inconsistent results between published studies, and this may be due to technical difficulties in the extraction and quantitation of miRNA, along with a lack of standard clinical protocols for phlebotomy, sample processing, miRNA extraction and quantitation.71–74 Further work is therefore required before miRNA profiling may be used clinically but the promising results of these early studies suggest a potential role for miRNA profiling in future prostate cancer detection.
Conclusions
The fact that so many potentially novel prostate cancer biomarkers have been evaluated, yet none has to date replaced PSA testing to detect this malignancy, illustrates the difficulty in translating scientific discoveries from bench to bedside for routine clinical use. Encouraging progress has been made with several novel biomarkers that might fulfil important unmet clinical needs, but thorough evaluation, demonstrating superior performance compared with existing standards of care, is required prior to the widespread clinical use of a new biomarker. It is likely that the use of novel biomarkers as part of a risk calculator will yield optimal predictive value, as has been demonstrated by incorporating the four-kallikrein panel, fPSA and PCA3 into the Prostate Cancer Prevention Trial Prostate Cancer Risk Calculator (PCPTrc) and the European Randomised Study of Screening for Prostate Cancer (ERSPC) multivariable prediction model.97–99 Such an approach may reduce the over-diagnosis and over-treatment of prostate cancer whilst simultaneously enabling clinicians to focus on high-risk cases of localised prostate cancer in those men most likely to benefit from radical intervention.
Footnotes
Acknowledgements
None.
Conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
Not applicable.
Informed consent
Not applicable.
Guarantor
RJB
Contributorship
NAJ and RJB researched the literature and conceived the article. NAJ wrote the first draft of the manuscript. NAJ, RJB and FCH reviewed and edited the manuscript, and all authors approved the final version.