
Abstract
Influenza viruses cause substantial morbidity in children each year, especially among children with specific chronic conditions. In particular, neurologic disorders have emerged as a strong risk factor for influenza-related complications. Children with these disorders may be vulnerable due to diminished respiratory muscle strength, decreased muscle tone or impaired mobility, which can compromise pulmonary function and the ability to handle secretions. Although they represent a small fraction of the general pediatric population, children with neurologic disorders make up a disproportionately high number of those children who are hospitalized and die as a result of influenza-associated complications. Annual vaccination is the most effective way to prevent influenza and its complications, and is recommended for all children 6 months through 18 years of age, including children with neurologic disorders. Family members and those who work with these children in institutional, educational and daycare settings should also be vaccinated against influenza annually. However, there have been few studies of influenza vaccination specifically in this population. In addition, vaccine effectiveness may vary from year to year and vaccination will not prevent all infections. Early empiric antiviral treatment should be started promptly in these children if they present to healthcare providers with symptoms suspicious for influenza. This article reviews influenza epidemiology in children with neurologic disorders and what is known about vaccines and other methods of protecting this vulnerable population from influenza-related complications.
Introduction
Influenza A and B viruses cause annual epidemics of respiratory illness and are a significant cause of pediatric morbidity and mortality. An estimated 20,000 children under 5 years of age are hospitalized annually due to influenza complications [Thompson et al. 2004]. In addition, since 2004, the annual number of reported influenza-associated pediatric deaths in the United States has ranged from 34 to 153 during regular influenza seasons and 348 during the 2009 H1N1 pandemic [CDC, 2013a].
While many healthy children are hospitalized with influenza and nearly half of pediatric influenza-associated deaths are in children that have no known underlying medical condition [CDC, 2013a; Wong et al. 2013], influenza disproportionately affects children with specific chronic conditions. In particular, neurologic disorders have emerged as a particularly strong risk factor both for death from influenza and influenza-related complications such as respiratory failure and bacterial pneumonia [Bhat et al. 2005; Blanton et al. 2012; Coffin et al. 2007; Cox et al. 2011; Keren et al. 2005]. This review will first examine the reasons for increased risk from influenza in children with neurologic disorders and what is known about the influenza epidemiology in this population. It will also cover what is known about influenza vaccine efficacy, vaccination coverage, and treatment in this vulnerable population, with a focus on current recommendations in the United States.
Neurologic disorders are a heterogeneous group of conditions with a wide range of phenotypes and severity. For the purposes of this review, neurologic disorder refers to neurodevelopmental disorders, neuromuscular disorders and epilepsy. Neurodevelopmental disorders include such conditions as cerebral palsy and moderate to severe development delay or intellectual disability, while examples of neuromuscular disorders include muscular dystrophy, mitochondrial disorders and spinal muscular atrophy.
Reasons for increased risk from influenza
Neurologic disorders may increase the risk of complications from influenza in a variety of ways (Table 1). Children with these conditions may have diminished expiratory and inspiratory muscle strength [Inal-Ince et al. 2009], decreased muscle tone, impaired mobility, and mechanical and structural conditions such as scoliosis which compromise pulmonary function and the ability to handle secretions [Keren et al. 2005]. Children with specific conditions such as Down syndrome may be at higher risk from a variety of factors, such as cardiac defects and hypotonia, and may be immunocompromised because of their underlying disorder; in conditions such as Duchenne muscular dystrophy, in addition to their underlying muscle weakness, children may be taking long-term glucocorticoids or other immunosuppressive drugs, increasing their vulnerability to infection [Moxley et al. 2005]. In addition, a higher proportion of these children than the general population live in institutional settings, although this likely affects only a small fraction of those with neurologic disorders. Nevertheless, congregate care settings are an environment in which influenza outbreaks can cause significant morbidity and mortality [Azofeifa et al. 2013; CDC, 2012a].
Reasons for increased risk of influenza-associated complications among children with neurologic disorders [Blanton et al. 2012; Inal-Inceet al. 2009; Keren et al. 2005].

Influenza epidemiology
Influenza infection is a frequent cause of illness resulting in hospitalization in all children, but is especially common in those with underlying neurologic disorders. In the general population, the burden of influenza is highest among infants and very young children, and substantially lower in older children, with wide seasonal variability. From the 2009–2010 to the 2012–2013 influenza season, in children with laboratory-confirmed influenza identified through a population-based surveillance system, the highest hospitalization rate was for those aged 0–4 years (seasonal range, 15.8–66.2/100,000 children); it was substantially lower in children aged 5–17 years (4.0–27.3/100,000) [CDC, 2013a].
While hospitalizations reflect the most serious influenza infections, they represent the tip of the iceberg in terms of influenza-associated healthcare use; outpatient visits associated with influenza in the general population are estimated to occur 10–250 times more often than influenza-associated hospitalization in young children [Poehling et al. 2006]. Influenza-associated visits represent a significant share of all pediatric outpatient visits; another study demonstrated that the proportion of children presenting to either emergency departments or outpatient clinics during 5 influenza seasons who had laboratory-confirmed influenza ranged from 10 to 25% annually [Poehling et al. 2013]. However, there may be different thresholds both for outpatient visits and hospital admissions for children with underlying neurologic disorders, and comparable statistics are unknown for children with neurologic disorders. Influenza may also be underdiagnosed; many who seek medical care for influenza do not have laboratory testing performed and only a fraction receive a diagnosis of influenza [Poehling et al. 2006].
Neurologic disorders are relatively rare, with cerebral palsy, spina bifida and trisomy 21 (Down syndrome) representing an estimated 0.3% [Kirby et al. 2011], 0.04% and 0.1% [Parker et al. 2010] of the pediatric population, respectively. Autism spectrum disorders (1% of the pediatric population) and intellectual disability (2–3%) are somewhat more common [CDC, 2012b]. However, children with neurologic disorders are disproportionately represented among those who develop complications from influenza. In a cohort study conducted between April 2009 and April 2010, of the 838 children admitted to 35 pediatric intensive care units with confirmed or probable influenza A(H1N1)pdm09 virus infection, 263 (31.4%) had a neurologic or neuromuscular condition. The most common conditions were seizure disorder (n = 139), developmental delay (n = 199) and cerebral palsy (n = 70); neurologic and neurodevelopmental conditions were also found to be an independent risk factor for death in this cohort [Randolph et al. 2011]. In another cohort study of 745 children hospitalized with laboratory-confirmed influenza, 12% of children had neurologic and neuromuscular diseases; this disease category was also independently associated with increased risk of respiratory failure [odds ratio 6.0, 95% confidence interval (CI): 2.7–13.5]. This increased risk was higher than that of any other group, including children with chronic pulmonary or cardiac disease; having conditions in 2 of these 3 categories (neurologic, pulmonary or cardiac) increased the probability of respiratory failure from approximately 10% in each of these categories to up to 30–40% in children with neurologic and neuromuscular disease and either cardiac or pulmonary disorders [Keren et al. 2005]. In another analysis of the same cohort, a neurologic disease increased the probability of prolonged hospital stay by 33% compared with those without these conditions [Coffin et al. 2007].
However, while studies show that a substantial proportion of children who are hospitalized for influenza have neurologic conditions, there are few estimates of rates of hospital admission or outpatient visits in this population. One study examining medical billing claims data for 9.3 million children from July 2009 to July 2010 identified a cohort of 80,608 children (0.86%) with neurologic disorders, and examined the number of hospitalizations attributable to respiratory infections, including influenza. Children with neurologic conditions had 17 respiratory infection hospital admissions per 1000 person-years, compared with 2.4 per 1000 person-years in a random sample of all children in the database. This represented a seven-fold increased risk of respiratory infection hospitalization among children with previously identified neurologic disorders when compared with the general pediatric population [Havers et al. 2013]. These rates are likely to vary substantially based on the type and severity of the underlying conditions, although this has not been well documented.
As in the general population, the burden of respiratory illnesses is highest among the youngest children, but even among older children with neurologic conditions, influenza and other respiratory infections cause significant morbidity. In the same study, while the respiratory hospitalization rate was higher for children under 2 years of age with neurologic conditions compared to those 10–18 years (62 versus 9 hospitalizations per 1000 person-years, respectively), the relative rate (RR) was higher in the older children than in younger children, when compared with the general population (RR 8.0 in those <2 years versus 14.7 in those aged 10–18 years) [Havers et al. 2013].
A study of hospitalizations among children with cerebral palsy demonstrated that respiratory infections represent a frequent reason for hospital admission in this population, even among older children. Among 1064 youth (aged 13–17.9 years) and young adults (aged 23–32.9 years) with cerebral palsy, pneumonia admissions accounted for 12.6% of admissions in youth and 15.5% of admission in young adults. It was the most common reason for admission in young adults, and the second most common reason, after epilepsy, in youth [Young et al. 2011]. Healthcare providers and caregivers should be aware of the persistently elevated risk of severe respiratory infections that children with neurologic disorders face, even as they grow older.
Children with neurologic disorders also account for a disproportionate number of pediatric influenza-associated deaths. This became apparent during the 2003-04 influenza season, when, of the 149 children who died for whom underlying health status was available, 49 (33%) had chronic neurologic or neuromuscular conditions; these included developmental delay in 42 children, epilepsy in 23 and cerebral palsy in 14 [Bhat et al. 2005]. In response to the large number of pediatric deaths that occurred during that influenza season, influenza-associated pediatric death became a nationally-notifiable condition. In every season from 2004 to 2012, neurologic disorders were the most common underlying medical conditions recorded among the 781 children with influenza-associated deaths for whom a medical history was recorded. Of the 448 with a high risk condition, the majority (57%) had an underlying neurologic disorder [Wong et al. 2013]. Similarly increased risk of death was seen during the 2009 H1N1 pandemic. Of the 336 H1N1pdm09-associated pediatric deaths with information on underlying conditions available, 146 (43%) had a neurologic condition. Among those, intellectual disability (n = 111, 76%), epilepsy (n = 74, 51%) and cerebral palsy (n = 51, 35%) were the most frequent [Blanton et al. 2012]. However, these conditions are not mutually exclusive. In particular, epilepsy and intellectual disability frequently co-occur with other neurologic disorders and may indicate increased severity of the underlying disorder; this may be why these conditions were the most frequently identified. Specific increased risk of poor outcomes from influenza in different neurologic conditions has not been well characterized.
Increased risk for neurologic complications from influenza
In addition to increased risk of influenza-associated hospitalization and death, underlying neurologic disorders are an independent risk factor for developing influenza-related neurologic complications, such as seizures, influenza-related encephalopathy, postinfectious influenza encephalopathy, or cerebral infarction [White et al. 2008]. In a cohort of 842 pediatric patients hospitalized with laboratory-confirmed influenza, the age-adjusted odds ratio of developing an influenza-related neurologic complication was 5.6 (CI 3.2–9.6) among the 115 children with an underlying neurologic and neuromuscular disorder when compared with previously healthy children [Newland et al. 2007]. A prospective study among 506 patients hospitalized with H1N1pdm09 infection also confirmed this; of the 68 children with underlying neurologic conditions, 21 (42.8%) had neurologic complications, and were 6.5 times more likely to have had neurologic complications from H1N1pdm09 infection than other children admitted with H1N1pdm09 infection [Khandaker et al. 2012]. This was not surprising as children with underlying neurologic conditions, including epilepsy, may have increased seizure activity during an acute infection because fever often lowers seizure threshold.
Vaccine recommendations
Annual influenza vaccination is the best method to prevent influenza and since 2008 has been recommended by the Advisory Committee on Immunization Practices (ACIP) of the US Centers for Disease Control and Prevention (CDC) for all children ≥6 months of age [Fiore et al. 2008] (Table 2). However, because children with neurologic disorders are at greatly increased risk for influenza complications, the ACIP recommended in 2005 annual influenza vaccination for persons ≥ 6 months with any condition (e.g. cognitive dysfunction, spinal cord injury, seizure disorder, or other neuromuscular disorder) that could compromise respiratory function or the handling of respiratory secretions or that can increase the risk for aspiration; these recommendations included all children with neurologic disorders [Harper et al. 2005]. The World Health Organization (WHO) Strategic Advisory Group (SAGE) on Immunization recommends that all children aged 6 to 59 months and all those with high-risk conditions receive seasonal influenza vaccination. SAGE includes neurodevelopmental disorders, specifically cerebral palsy, musculodystrophy and cognitive disorders in its list of high-risk conditions [SAGE Working Group, 2012]. Because vaccines and guidelines for their use may differ from year to year and vary by country, healthcare providers are advised to review annual guidelines issued by the ACIP or their own domestic public health agencies, as these recommendations may change.
US Influenza vaccination recommendations for children and adolescents with neurologic disorders aged 6 months to 18 years.*
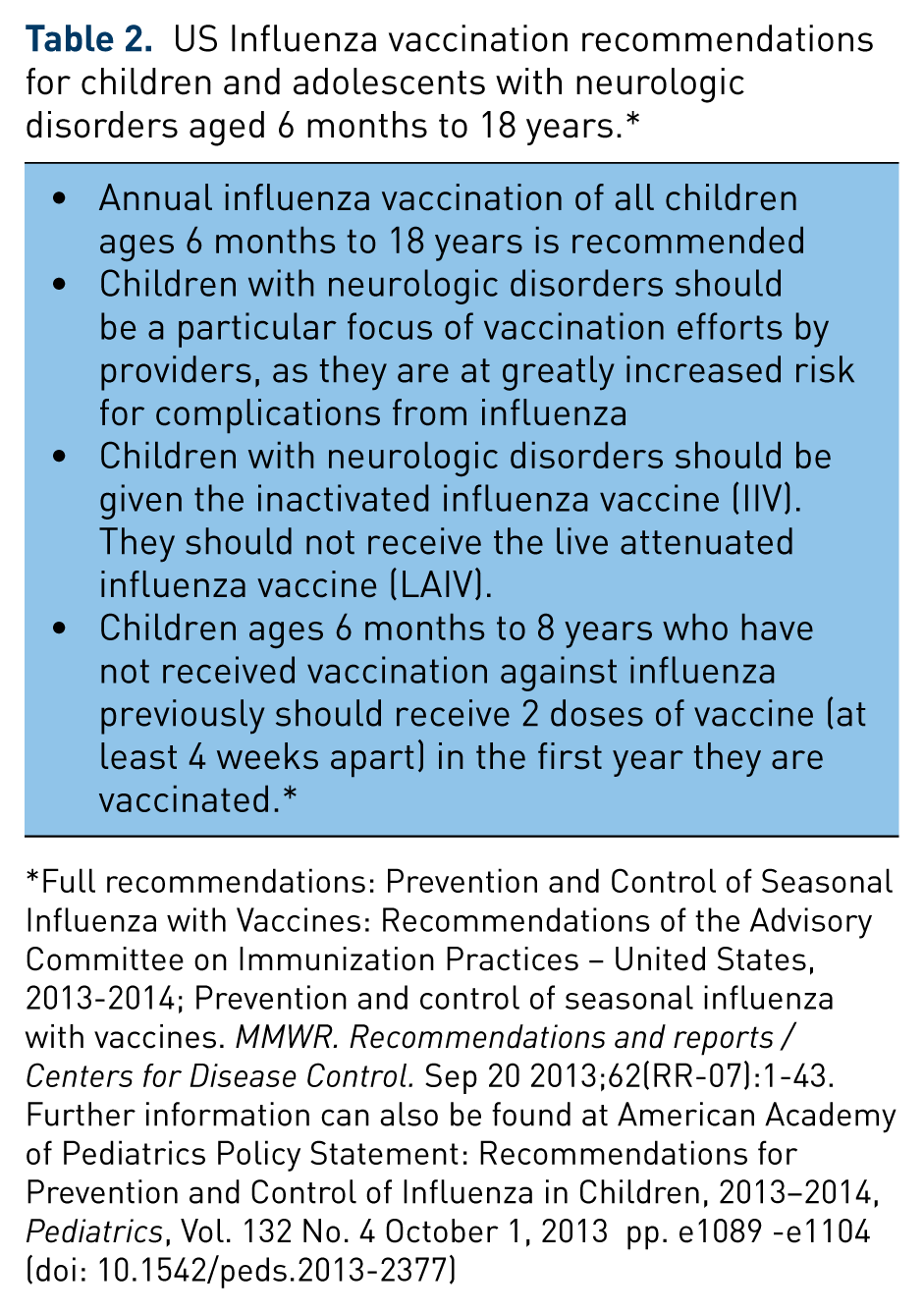
Full recommendations: Prevention and Control of Seasonal Influenza with Vaccines: Recommendations of the Advisory Committee on Immunization Practices – United States, 2013-2014; Prevention and control of seasonal influenza with vaccines. MMWR. Recommendations and reports / Centers for Disease Control. Sep 20 2013;62(RR-07):1-43. Further information can also be found at American Academy of Pediatrics Policy Statement: Recommendations for Prevention and Control of Influenza in Children, 2013–2014, Pediatrics, Vol. 132 No. 4 October 1, 2013 pp. e1089 -e1104 (doi: 10.1542/peds.2013-2377)
There are two main categories of seasonal influenza vaccines available for children, the inactivated influenza vaccine (IIV) and a live-attenuated influenza vaccine (LAIV). IIV, previously referred to as the trivalent inactivated vaccine (TIV), is given intramuscularly in children and cannot cause influenza virus infection. The LAIV vaccine, administered as an intranasal spray, uses weakened influenza virus. LAIV is not recommended for any child with a medical condition that increases his or her risk of having influenza-related complications; this includes children with neurologic disorders. Thus, ACIP recommends that children with neurologic disorders aged ≥6 months receive the IIV annually. In addition, children aged 6 months to 8 years who have not previously been vaccinated require 2 doses of influenza vaccine (administered a minimum of 4 weeks apart) to optimize immune response. More detail can be found in the ACIP and American Academy of Pediatrics (AAP) guidelines forvaccine use [Committee On Infectious Disease, 2013; Influenza Division, National Center for Immunization and Respiratory Diseases, 2013]. Beginning in the 2013–2014 season, the IIVs available include a trivalent vaccine (IIV3), which contains two influenza A strains and one influenza B strain, and a quadrivalent vaccine (IIV4), which contains a second influenza B strain of an antigenically distinct lineage. The vaccination should be given as soon as it is available, preferably before the onset of influenza in the community, so that there is time for production of protective antibody levels.
Vaccine efficacy and effectiveness
How well influenza vaccines work to protect children is measured in assessments of vaccine efficacy, which is the prevention of illness among vaccinated persons in controlled trials, and vaccine effectiveness, which is the prevention of illness in vaccinated populations. Both vaccine efficacy and effectiveness vary depending on an individual’s characteristics and characteristics of that year’s circulating virus and vaccine. Commonly used measures of the immune response to vaccination involve the post-vaccination geometric mean antibody titer against the vaccine strain using a hemagglutination-inhibition assay (HAI); the seroprotection rate is defined as the proportion of vaccinated persons with serum HAI titer ≥1:40, and the seroconversion rate is the proportion of subjects with 4-fold antibody increase in titer between the pre- and post-vaccine titers.
Most studies of vaccine efficacy and effectiveness among children have been done on healthy children and these studies have shown that influenza vaccines are effective in preventing influenza infections in the general pediatric population. Prospective observational data collected during 2005–2007 demonstrated that children aged 6 months to 5 years who were vaccinated with IIV had 56% (95% CI: 25–74%) fewer influenza-related medical visits than unvaccinated children [Staat et al. 2011]. Adjusted vaccine effectiveness estimates indicate that vaccination with the 2011–2012 influenza season vaccine reduced the risk for outpatient medical visits resulting from influenza by 45% (95% CI: 20–62) in children aged 6 months to 8 years and 58% (95% CI: 27–76) in children 9–17 years [Ohmit et al. 2013].
Whether vaccine effectiveness is similar in children with neurologic disorders is unknown, given that few studies have been carried out on influenza vaccines in this population. Children with underlying medical conditions may not mount as robust an immune response to vaccines as healthy children. In addition, a small fraction of children with neurologic disorders are on chronic steroids or other immunosuppressive drugs for their underlying conditions, which may further impair humoral responses to influenza antigens. Immune responses to influenza vaccines have been studied in immunocompromised populations such as pediatric oncology patients [Bate et al. 2010] and other patient populations on glucocorticoids [Hanania et al. 2004; Lu et al. 2011], but very few studies have been done in children with neurologic disorders.
One study evaluated the immunogenicity of intramuscular versus subcutaneous administration with IIV vaccine individuals aged 10–28 with neuromuscular disease. This study was conducted to test the hypothesis that the immune response to IIV is potentially inadequate when given intramuscularly into fibrosed muscle, a clinical phenomenon common among children with neuromuscular disorders. A total of 22 subjects, 16 of whom had Duchenne muscular dystrophy and 10 of whom were on chronic corticosteroids, were randomized to subcutaneous versus intramuscular routes of administration of IIV. There was no difference in seroprotection rate, seroconversion rate and geometric mean titer ratios between the routes of administration, although the seroprotection rates achieved did vary by influenza strain. All 22 children did achieve seroprotection against H1N1, although only 17 and 13 achieved seroprotection again H3N2 and influenza B, respectively [Golekoh et al. 2013]. In this study, there was no control group to compare the immunogenicity of the vaccine in this population with the general population.
Several other studies conducted on adults with severe motor and intellectual disability suggest that while people with these disorders do mount an immune response to influenza vaccination, it is diminished compared with healthy controls. One Japanese study examined immune response to the 2009 monovalent H1N1pdm09 vaccine in 104 institutionalized adults with severe motor and intellectual disability. Those who received the vaccine had a lower increase in antibody titer and a lower seroconversion rate from unprotected to protected status compared to healthcare worker controls [Hara et al. 2011]. Two additional studies of institutionalized Japanese adults during the 2004–2005 and 2005–2006 influenza seasons demonstrated that antibody response to IIV3 was lower in those with severe multiple disabilities than a control group of healthcare workers [Otsuka et al. 2006, 2007]. Antibody response, while attenuated in the study subjects, appeared to be more affected by the subjects’ age than the severity of their underlying conditions, and older age was significantly associated with diminished immune response [Otsuka et al. 2006]. The youngest group of subjects, aged 18–28 years, had a more robust response compared with older adults, although it was still lower than that of the controls. Further study in children with neurologic disorders is needed to evaluate immunogenicity and effectiveness of vaccines in this population.
IIVs are generally safe and well tolerated. Minor side effects that can occur include soreness, redness or swelling at the injection site, low-grade fevers or muscle aches.
Vaccination coverage
Despite the proven effectiveness of vaccination in preventing influenza, vaccination coverage remains low in the general pediatric population. In the 2010–2011 and 2011–2012 seasons, influenza vaccination coverage among all children in the US 6–17 years of age was estimated to be 51.0% and 51.5%, respectively [McIntyre et al. 2013]. However, little specific data exist on vaccine coverage among children with neurologic disorders. In one study conducted during the 2010–2011 influenza season among 1005 parents of children with neurologic conditions, 50% reported their child had received or had an appointment scheduled to receive influenza vaccine at the time of survey completion. This suggests that despite being at increased risk for complications from influenza, children with neurologic conditions are no more likely to be vaccinated than healthy children. Among the 412 physicians who completed an online survey as part of the study, intellectual disability was recognized as a high-risk condition by 46% of respondents and epilepsy by 52% [CDC, 2013b]. Many healthcare providers and parents may be unaware of the increased risk of serious complications from influenza that these children face.
The risk of hospitalization and complications from influenza drops sharply as healthy children get older. This decreasing risk may be one of the reasons why vaccination rates are highest among all children aged between 6 and 23 months and vaccination coverage decreases in older age groups [McIntyre et al. 2013]. However, children with neurologic disorders continue to face elevated risk of complications due to influenza even in older age groups. Specific rates of vaccination coverage by age in this population have not been published, but caregivers and healthcare providers must remain vigilant about influenza vaccination as children grow older. In addition, close contacts such as family members, school personnel and childcare providers should also receive annual influenza vaccines to further decrease the risk of transmitting the virus to this vulnerable population.
Influenza treatment
Annual vaccination is the most effective means of reducing complications from influenza, and is recommended for all children ≥6 months of age. However, vaccine effectiveness may vary from year to year and vaccination will not prevent all infections. Thus, additional approaches to decreasing influenza morbidity and mortality are needed. One of the most important is early empiric treatment with an antiviral agent, of which there are two classes currently available: the neuraminidase inhibitors (oseltamivir and zanamivir) and the adamantanes (amandtadine and rimantadine). Given widespread adamantine resistance among influenza A(H3N2) and H1N1pdm09 viruses and the fact that they are ineffective against influenza B viruses, only neuraminidase inhibitors are recommended for treatment or chemoprophylaxis of currently circulating influenza viruses. However, resistance to antiviral medications may change and clinicians should monitor susceptibility information throughout the season either on the AAP website (http://www.aap.org or http://aapredbook.aappublications.org/flu) or the Centers for Disease Control and Prevention (CDC) web site (www.cdc.gov/flu/index.htm).
Current CDC guidance recommends that all children who are at higher risk for complications from influenza, which includes all children with neurologic disorders, receive treatment with a neuraminidase inhibitor if they present to their outpatient provider with symptoms suspicious for influenza [Fiore et al. 2011]. In addition, the CDC recommends initiation of antiviral treatment as soon as possible for all patients with confirmed or suspected influenza who have severe, complicated or progressive illness or who require hospitalization. Treatment should be given as soon as possible, preferably within 48 hours of symptom onset, but clinicians should consider treatment in this population regardless of timing of symptom onset. If testing for influenza is performed, treatment should not be delayed while test results are pending. The FDA has licensed oseltamivir down to 2 weeks of age, although per AAP guidelines, given its known safety profile, it can be used to treat influenza in both term and preterm infants from birth (Committee on Infectious Disease, 2013). Information on influenza antiviral dosage and formulations is available on the CDC Web site (http://www.cdc.gov/flu/professionals/antivirals/index.htm) or through the AAP (http://aapredbook.aappublications.org/flu).
In two systematic reviews, treatment with neuraminidase inhibitors has been found to reduce the duration and severity of influenza symptoms in healthy children with uncomplicated influenza [Cooper et al. 2003; Matheson et al. 2007]; other studies have shown that oseltamivir reduced hospital length-of-stay in critically ill pediatric patients [Coffin et al. 2011] and acute otitis media in outpatient children [Whitley et al. 2001; Winther et al. 2010].
No studies have focused on antiviral treatment in children with neurologic conditions and few have focused solely on children with other underlying medical conditions. Piedra and colleagues examined the effect of outpatient oseltamivir prescription using insurance claims data among 5335 children 1–17 years of age with an underlying medical condition that put them at higher risk for complications from influenza, a group which included 17 children with neurologic disorders. They found that prompt outpatient treatment with oseltamivir reduced the risk of otitis media and its complications, all-cause hospitalizations and respiratory illnesses other than pneumonia [Piedra et al. 2009].
Typical symptoms that should prompt use of antiviral agents include abrupt onset of constitutional and respiratory signs and symptoms (e.g. fever, nonproductive cough, sore throat, rhinitis), although in children, otitis media, nausea and vomiting are commonly reported with influenza illness. No studies currently published describe the clinical presentation of influenza in children with neurologic disorders and this population may present differently than healthy children. They may be more likely to present neurologic symptoms, such as seizure, and may lack the traditional symptoms of fever, cough and sore throat. It is important that clinicians consider the diagnosis of influenza in children with underlying neurologic conditions presenting with atypical symptoms during influenza season, including seizures, encephalopathy and irritability.
Neuraminidase inhibitors (oseltamivir and zanamivir) are generally well tolerated in children. Most side effects are mild and short-lived, with nausea, vomiting and abdominal discomfort being the most frequent side effects. Transient neuropsychiatric events (delirium or self-injury) have been reported postmarketing among persons taking oseltamivir; the majority of these reports were among Japanese adolescents and adults [The Lancet, 2007]. However, several studies, as well as analyses of postmarketing data, found that oseltamivir is not associated with an increased risk for neuropsychiatric adverse events [Okumura et al. 2006]. The 1902 people who took oseltamivir as part of randomized blinded studies, either for treatment or prophylaxis, had no significant difference in incidence of neuropsychiatric adverse events compared to the placebo groups in those trials [Toovey et al. 2012]. One retrospective cohort analysis of influenza patients aged 1–21 years, which used a propensity-adjusted regression model, showed a statistically significant protective effect associated with oseltamivir treatment in the prevalence of neuropsychiatric diagnoses compared with those that did not receive oseltamivir, underscoring that influenza infection itself is associated with central nervous system (CNS) disorders [Casscells et al. 2009]. Another retrospective cohort study of children and adults using healthcare insurance claims data for six influenza seasons (2000 to 2006) did not show any increased risk of CNS-related and neuropsychiatric events among those prescribed oseltamivir compared with those with influenza who did not [Blumentals and Song, 2007]. The US Food and Drug Administration (FDA) advises that persons taking oseltamivir be monitored for abnormal behavior [US FDA, 2013].
In very young children (<1 year), mild gastrointestinal symptoms were common in a retrospective study evaluating safety and outcomes with oseltamivir therapy, but there were otherwise no adverse events attributable to the drug [Siedler and Skopnik, 2010]. Clinicians who are considering administering oseltamivir to infants should consult the CDC website for treatment recommendations because dosing guidelines may be revised if additional data become available http://www.cdc.gov/flu/professionals/antivirals/index.htm.
Some children with complex neurologic conditions reside in long-term care facilities, settings in which influenza outbreaks can cause substantial morbidity and mortality. In one instance, in 2011, an influenza outbreak occurred in a residential care facility providing services to children and young adults with neurologic conditions. A total of 13 residents developed confirmed or suspected influenza, resulting in 10 hospitalizations and seven deaths [CDC, 2012a]. Not only should residents of long-term care facilities be vaccinated annually, but all staff should be vaccinated as well. Several randomized controlled trials among elderly residents in long-term care facilities demonstrated that vaccination of healthcare workers was associated with a substantial decrease in mortality among facility residents. These studies underscore the importance of healthcare worker vaccination in protecting vulnerable long-term care residents, who themselves may not mount a strong immune response after vaccination [Carman et al. 2000; Lemaitre et al. 2009]. In addition, active respiratory illness surveillance during influenza seasons and good infection control procedures can help to prevent outbreaks from occurring. Any influenza outbreak that does occur in a long-term care facility should prompt early antiviral therapy for symptomatic patients, chemoprophylaxis for exposed residents, and patient cohorting and other infection control measures. For updated guidelines on influenza outbreak management in long-term care facilities, please see the web page, www.cdc.gov/flu/professionals/infectioncontrol/ltc-facility-guidance.htm.
Children who reside in long-term care facilities represent a small fraction of children with underlying neurologic disorders. However, educational and daycare settings are also common settings for widespread influenza transmission; childcare workers and school personnel, particularly those who care for children with disabilities, should also receive influenza vaccination annually.
Conclusion
Children with neurologic disorders are a vulnerable population at very high risk for serious complications from influenza. Although they represent a small fraction of the general pediatric population, they make up a disproportionately high number of those children who are hospitalized and die from influenza-associated complications. Although not perfect, annual influenza vaccination is the best tool available for protecting this vulnerable population. However, more studies are needed to understand the effectiveness of vaccines in the population and ways of optimizing protection against influenza. In addition to annual vaccination, family members, school personnel, caregivers and other close contacts should be vaccinated against influenza annually, and children in this high risk group should be given prompt treatment with antiviral medications if they present to healthcare providers with symptoms suspicious for influenza.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.
Disclaimer
The opinions expressed by authors contributing to this article do not necessarily reflect the opinions of the Centers for Disease Control and Prevention.