
Abstract
Background
Colonoscopy is the gold standard investigation for the detection of colorectal cancer, but the right colon is more difficult to examine than the left colon. A second examination of the proximal colon has the potential to reduce rates of missed pathology.
Objective
To determine whether proximal retroflexion improves the adenoma detection rate or other outcomes in the right colon compared with the forward view.
Methods
We performed a multicentre randomized controlled trial of patients from the colorectal cancer screening programme with a positive faecal immunochemical test. Patients were randomized to a second right colon examination using proximal retroflexion or forward view.
Results
A total of 692 patients were included. A second examination of the right colon, with an average additional procedure time of 1.62 min, increased the adenoma detection rate by 11%, regardless of the method used (9% proximal retroflexion vs. 12% second forward view, p = 0.21). The adenoma miss rate was 19% (17% proximal retroflexion vs. 20% forward view, p = 0.28) The success rate of retroflexion was 83%, without secondary complications. In the 15.6% of patients in whom lesions were detected during the second pass, endoscopic follow-up was modified by reducing the time of the next colonoscopy.
Conclusions
A second examination of the right colon, either from retroflexion or second forward view, can increase adenoma detection rate and shorten surveillance intervals in patients undergoing screening colonoscopy. This should be emphasized during colonoscopy training and integrated into diagnostic colonoscopy practice.
Key summary
To summarize the established knowledge on this subject:
Colonoscopy is the gold standard for detecting and removing preneoplastic lesions. Colonoscopy is less effective in preventing right-sided compared with left-sided CRC. New techniques and manoeuvres have been developed to improve the quality of colonoscopy and to reduce missed lesions and post-colonoscopy colorectal cancers. Proximal retroflexion of the colonoscopy may improve visualization of the proximal side of the folds and increases ADR. No data exist in a positive FIT screening cohort.
What are the significant and/or new findings of this study?
Proximal retroflexion manoeuvre in the right colon is safe. We find that second examination of the right colon in retroflexed or forward view increases ADR by 11% in CRC screening patients with positive FIT. Re-examination of the right-side colon should be considered in patients referred for CRC screening colonoscopy with positive FIT. In the 15.6% of patients in whom lesions were detected in the second examination, endoscopic surveillance was modified, reducing the time to the next colonoscopy according to the ESGE guidelines.
Introduction
Colorectal cancer (CRC) is the second cause of cancer in Europe and the second cause of death 1 from cancer, although its incidence and mortality rate are decreasing in persons undergoing screening. 2 Colonoscopy, the gold standard for detecting preneoplastic lesions, provides the possibility of resection and preventing lesions from progressing to CRC. 3
Colonoscopy is less effective in preventing right-sided compared with left-sided CRC.4–7 Proximal lesions are more difficult to detect due to their endoscopic characteristics: pale, flat appearance, located between the haustra and on the proximal side of the folds. 6 Therefore, various devices (full-spectrum endoscope, Endocuff Vision®, among others)8–11 and exploratory manoeuvres have been incorporated to increase adenoma detection rates (ADRs), including dynamic position changes, 12 proximal retroflexion and second forward view.13–15
This study focuses on the meticulous examination of the right colon, to decrease the rate of undetected adenomas, which, according to the literature, is around 27–33%. 16 , 17 A 1% increase in ADR reduces interval cancer by 3%. 3 Reports show disparate results for proximal retroflexion, but uniformly show an increased ADR after a second right colon examination.17–19 The population analysed in all studies is heterogeneous, so we wanted to focus only on patients from a CRC screening programme with a positive faecal immunochemical test (FIT). The main objective of this study was to determine whether proximal retroflexion improved the ADR in the right colon compared with a forward view in a CRC screening programme with a positive FIT.
Materials and methods
This is a multicentre randomized controlled and prospective trial. The study was carried out in the Gastroenterology Department of three Spanish hospitals (Rio Hortega Hospital, Hospital del Mar and Hospital Santos Reyes) from October 2017 until October 2018 in asymptomatic subjects aged 50–69 years referred by the CRC screening programme for colonoscopy after a positive FIT (>20 µg/g). The study was approved by the Rio Hortega Hospital´s Ethical Board (6 June 2017, CEIC: 62/16) and the respective ethics committees. The study protocol conforms with the ethical guidelines of the 1975 Declaration of Helsinki.
Patients who agreed to participate in the study, and after written informed consent was obtained, were included in a common database (sequentially numbered containers) and randomized to second right colon examination using proximal retroflexion or forward view.
Patients randomized to proximal retroflexion in whom the manoeuvre was not possible received a second exam using forward view.
Study subjects: consecutive asymptomatic patients aged 50–69 years with a positive FIT (>20 μg/g) referred by the CRC screening programme who gave signed informed consent were included. Preparation for colonoscopy followed the protocols of participating centres, and a right colon Boston Bowel Preparation Scale (BBPS) score of ≥2 was required.
Exclusion criteria were: patients who rejected giving informed consent, incomplete colonoscopy, inadequate preparation (right side colon BBPS <2) or pathological findings: colorectal malignant neoplasm, diverticulitis, inflammatory bowel disease or colonic stenosis on examination.
In this study involving caecal retroflexion, the right colon was defined as the caecum, ascending colon and hepatic flexure. However, in general colonoscopy the right colon also includes the transverse colon proximal to the splenic flexure. The endoscopist evaluated the level of confidence in the retroflexive manoeuvre on a 0–10 visual analogue scale (VAS).
We determined the per-colonoscopy adenoma miss rate (AMR) of the right colon by determining the number of additional adenomas in the right colon detected by retroflexive view or frontal view divided by the number of total colonoscopies performed in each group.
Colonoscopy was carried out by five expert endoscopists performing at least 200 colonoscopies per year, each physician with more than five years of experience. They were not experienced in using proximal retroflexion. Between June 2017 and September 2017 they were provided with written information and training videos on proximal retroflexion manoeuvre.
Colonoscopy was carried out using a standard forward view colonoscope (diameter 12.8 mm, working channel 3.7 mm) with a high-resolution Olympus Exera II and Exera III video processor with a 170° angle of view (H180 and H190 series, Olympus). Candidates for colonoscopy followed the Colon Cleansing Protocols of each hospital. The BBPS was evaluated (right-side colon scores < 2 were excluded from the study). Colonoscopy was performed under deep sedation with propofol usual dose 1.5–2.5 mg/kg delivered by bolus and CO2 insufflation.
Once the caecal pole was reached and after thorough examination of the caecum, the endoscope was withdrawn to the hepatic flexure by forward view, resecting the polyps found, and making a thorough inspection of the proximal face of the haustral folds. Once the hepatic flexure was reached, the endoscope was progressed again to the caecal pole and a second withdrawal was carried out by forward view or retroflexion until the hepatic flexure was reached again with the resection of the polyps identified in the second pass. Retroflexion was performed with the endoscope tip in or near the caecum, through the maximum angulation up and left of the tip, and the insertion tube rotated counter-clockwise to enter retroflexion. The patient position during the second examination was chosen by each endoscopist and is not recorded in the study. Proximal retroflexion was considered successful when the right colon at or near the caecal pole could be examined to the hepatic flexure with the maximum angle of the tip of the endoscope upwards and to the left and with the insertion tube rotated clockwise simultaneously. Information on whether polyps were viewed on the first or second pass and by forward view or retroflexion view, and the success of endoscopic resection, was collected. To determine withdrawal time, the stopwatch was stopped during polypectomy. The localization of the polyps was analysed according to the different zones of right side colon: caecum, ascending colon divided into right proximal colon, middle right colon and right distal colon or hepatic flexure.
Outcome and definitions
The main objective of this study was to determine whether proximal retroflexion improved the ADR in the right colon compared with a forward view in the FIT-based CRC screening programme.
Secondary objectives were to determine whether a second exploration of the proximal areas, whatever the method used, increased the ADR; to evaluate the right-side AMR, to evaluate per-adenoma miss rate of the right side colon in each randomized group, to evaluate the per-colonoscopy AMR of the right colon; to determine the success rate of proximal retroflexion and the possible causes of failure; to evaluate complications due to proximal retroflexion and to analyse pre-procedure factors that could influence the prevalence of precursor lesions in the colon.
We determined the right-side colon ADR as the number of colonoscopies with ≥1 adenoma on the right colon divided by the number of total colonoscopies performed in each group.
We determined the per-adenoma miss rate of the right colon in each randomized group as the number of additional adenomas in the right colon detected by retroflexed view or forward view divided by the total adenomas in right colon (forward view plus retroflexed view). 20
We determined the per-colonoscopy AMR of the right colon by determining the number of additional adenomas in the right colon detected by retroflexed view or frontal view divided by the number of total colonoscopies performed in each group. 21
We considered advanced adenoma to be: high grade adenoma or villous component or adenoma ≥10 mm in size.
The size, shape and location of polyps identified and/or resected were collected. The morphology was described according to the Paris classification and the size was estimated by the size of the open biopsy forceps prior to resection. Polyps <5 mm were resected with a cold forceps, pedunculated polyps ≥5 mm with a snare polypectomy and non-pedunculated polyps by mucosectomy.
Variables collected
We collected the characteristics of adenomas identified in each procedure: shape, size and histology; the rate of polypectomies carried out and the polyps recovered for histological study; the time of withdrawal to the hepatic angles and the total withdrawal time (stopwatch halted during polypectomy); adverse events at the time of the procedure and the 30 days post-procedure; and, possible influencing factors of the ADR such as smoking, alcohol abuse (>20 g ethanol/day in women and >40 g/day in males) and the FIT score. We collected complications with the retroflexion manoeuvre. Self-confidence of proximal retroflexion was evaluated using a VAS and the learning curve for proximal retroflexion was assessed by measuring success and failure rates over time.
Statistical analysis
The sample size was calculated assuming there would be 4–10% more polyps in the second pass, according to published results. 18 , 21 , 22 The sample size needed to demonstrate a difference of 6% in the ADR between the two techniques was 314 subjects in each group (alpha error 5%, power 80%), and assuming a 10% loss.
Percentages were compared using the chi-square test or Fisher’s exact test as required. Non-conditional logistic regression was used to adjust for other variables of interest. In the bivariate analyses, contingency tables and the chi-square test were used to detect possible relationships between qualitative variables. The Student t test or non-parametric alternatives were used to compare quantitative variables. Yates’ correction was applied to the chi-square tests. A Poisson regression model was constructed to study differences in the number of adenomas detected by each procedure. In all tests, the level of statistical significance was set at 5% and 95% confidence intervals were calculated to indicate the accuracy of the estimate. The analysis was made using the R Core Team (R package version 2018.04.17) program with the RStudio interface.
Results
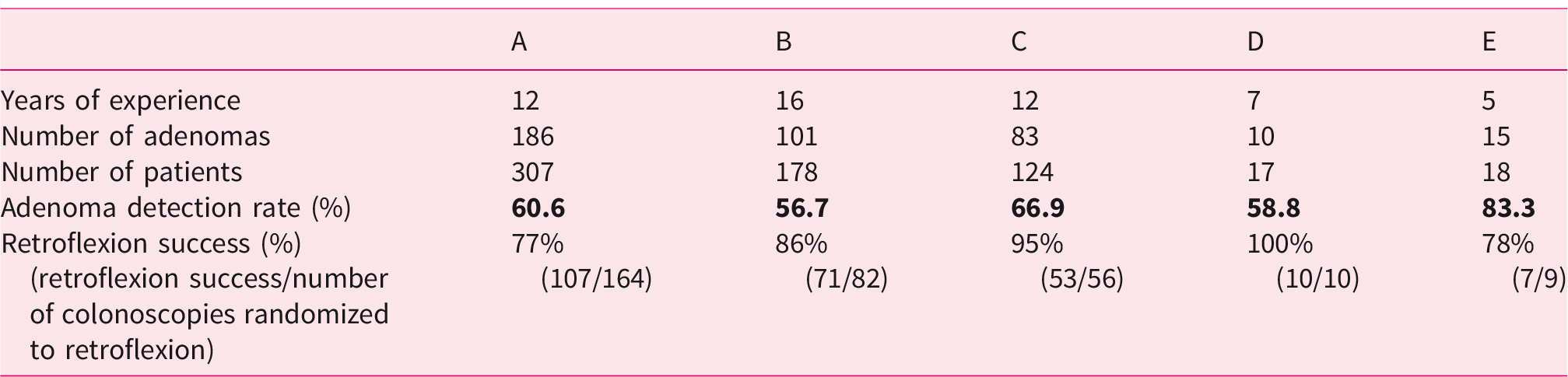
We initially included 692 patients, of whom 44 were excluded due to incomplete colonoscopy (n = 18), inadequate preparation (n = 22) or pathological findings during colonoscopy (n = 13). Finally, 316 patients were assessed in the proximal retroflexion group and 332 in the forward view group. Fifty-three patients were unable to be assessed using retroflexion and so were included in the forward view group (Figure 1). The two groups were similar in terms of sex, mean age, BMI, smoking, alcohol, previous surgery and BBPS scores (Table 1). Table 2 shows the patients included, the ADR per endoscopist and retroflexion success rate per endoscopist.
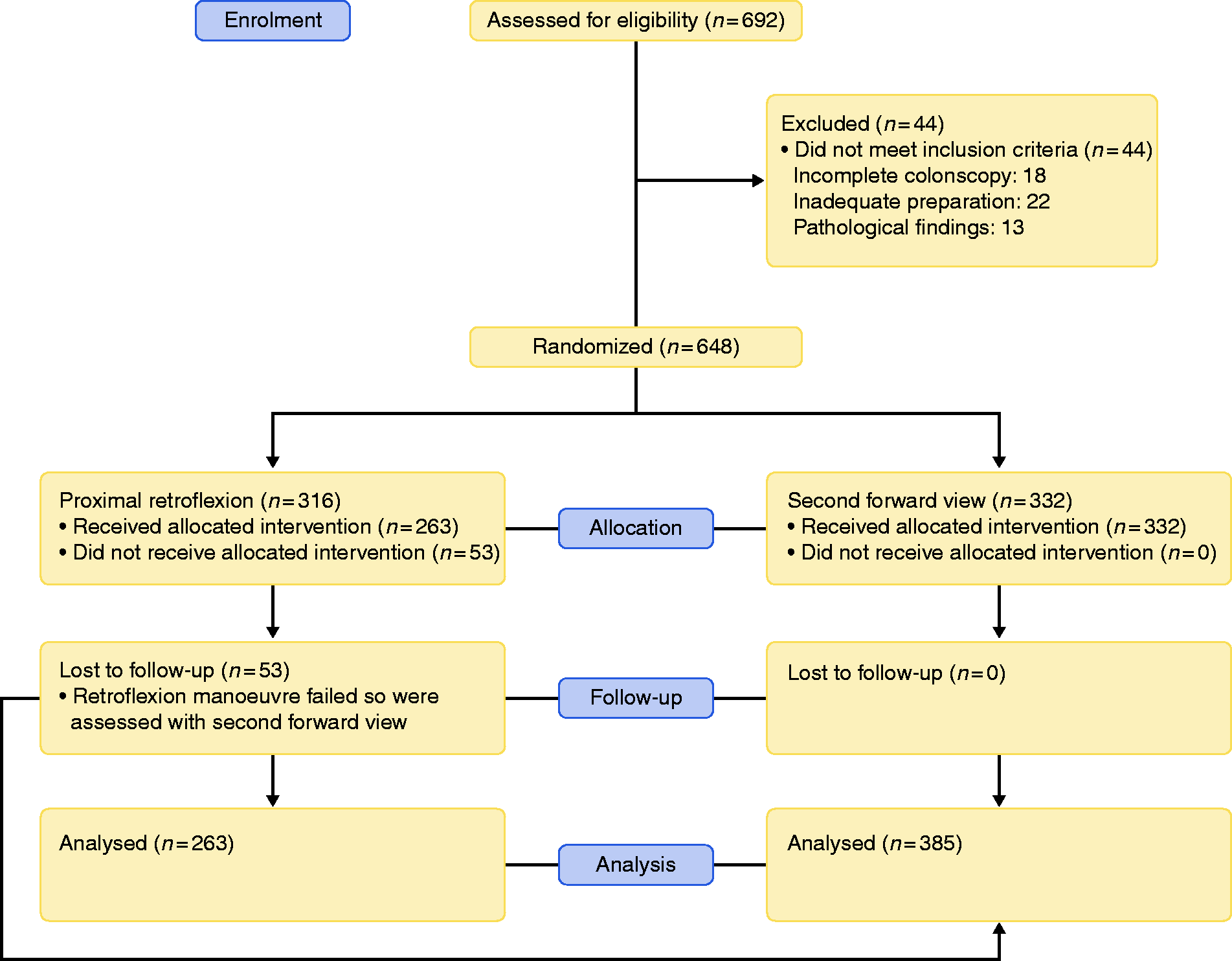
Flow diagram.
Baseline sociodemographic and health status variables.
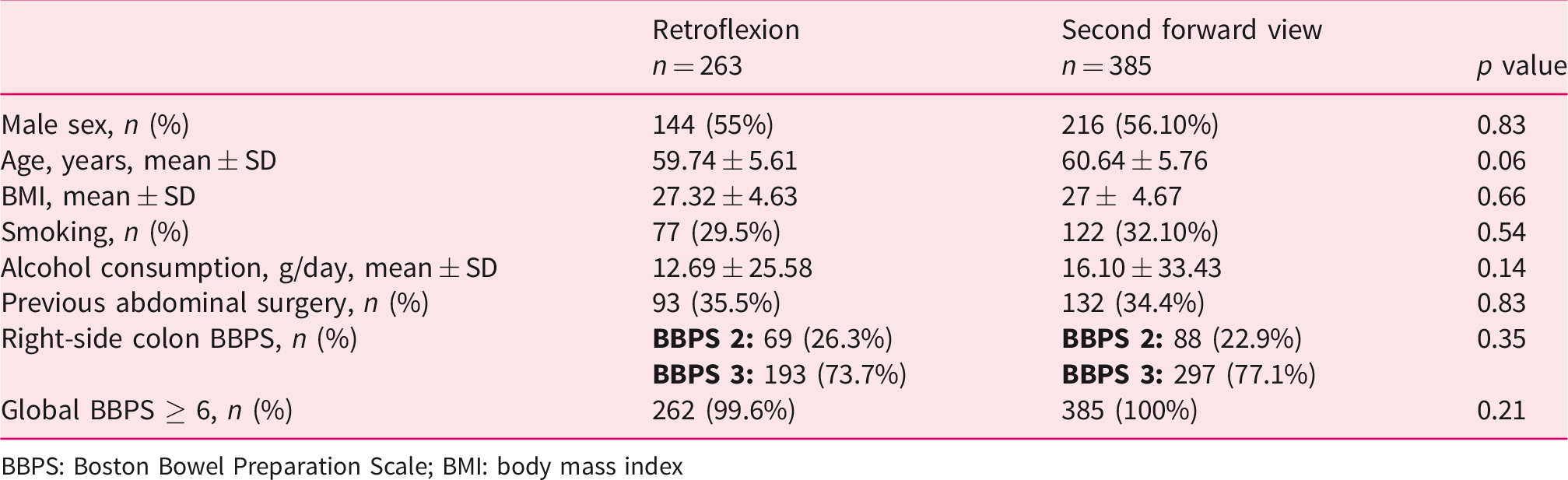
BBPS: Boston Bowel Preparation Scale; BMI: body mass index
Total adenoma detection rate in all sections of the colon and retroflexion success per endoscopist.
General characteristics and overall results
The global results were ADR 61% (396/648). The mean adenoma rate (MAR) per procedure was 1.9 (1248/648) and the MAR in colonoscopies with ≥1 adenoma was 5.35 (1248/233), a polyp detection rate of 69%, polyp retrieval rate (PRR) 94% and caecal intubation rate 97%. The mean total examination time from the caecum to the anus was 9.17 min (proximal retroflexion: 8.79±3.32 min vs. forward view: 9.44±5.27 min) (p = 0.07).
Proximal retroflexion
Proximal retroflexion was successful in 263/316 (83%) patients without complications. The causes of failure were most likely due to: endoscopic looping (39.6%); anatomical features (24.3%): (narrow colon and very short right colon (18.8%), multiple right colon diverticula (3.7%), colon fixation by previous surgery (1.8%)), unknown causes (33.9%) and large mucosectomy at right colon (1.8%). Figure 2(a) shows the learning curve for proximal retroflexion according to successes and failures over time. Self-confidence of retroflexion increased slightly over time, but the results were not significant (p = 0.051) (Figure 2(b)).
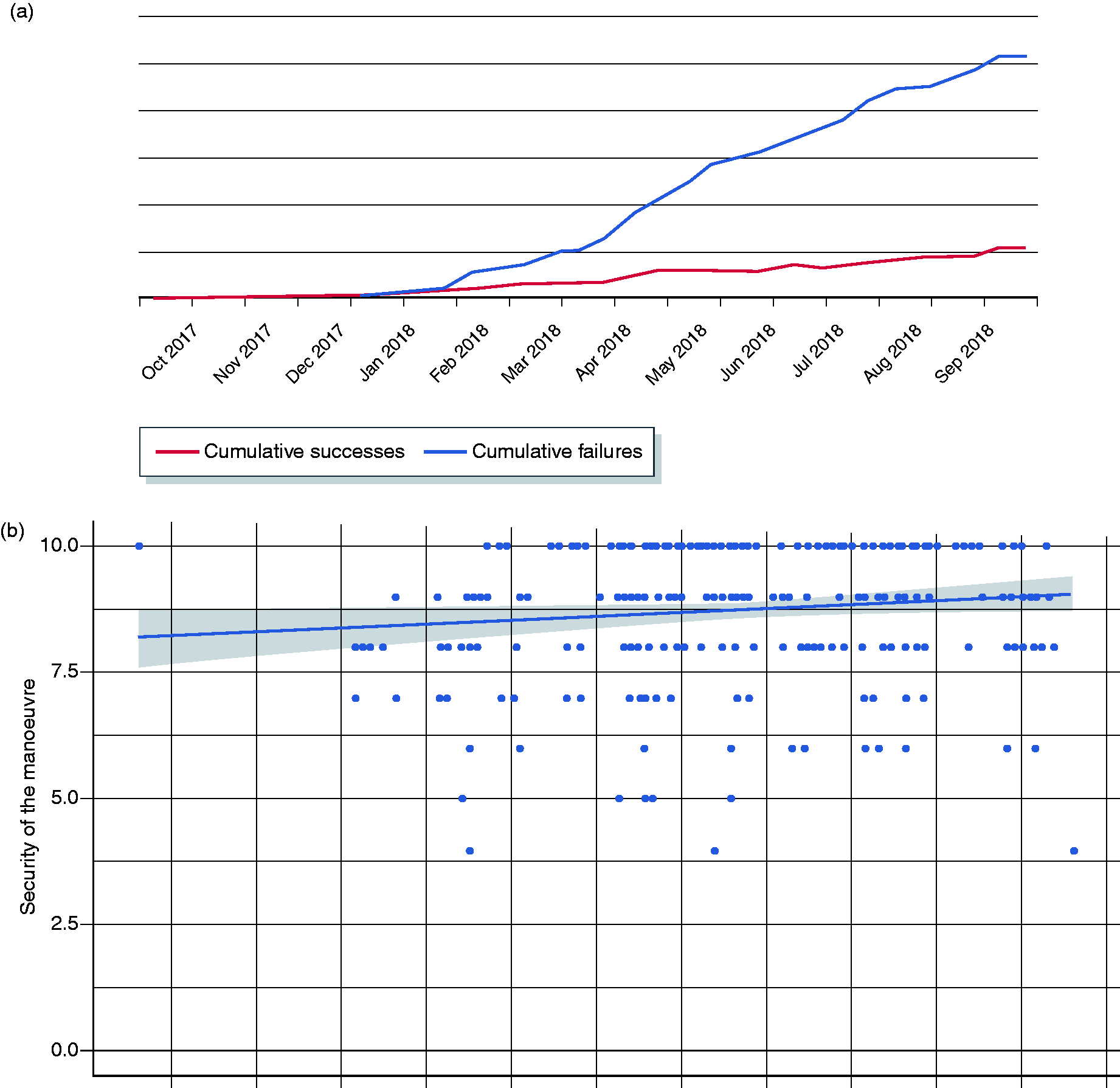
(a) Learning curve for the whole study is presented in this figure. The number of successes increases drastically from March 2018 until the end of the study compared with the number of failures. (b) Relationship between the security of the retroflexion manoeuvre along the time, according to visual analogue scale.
We analysed technical factors into predictors of failed retroflexion: endoscopic looping, anatomical features and unknown causes. The bivariate analyses do not demonstrate association between gender, previous surgery, age and BMI with the cause of failed retroflexion (Table 3).
Predictors of failed proximal retroflexion.
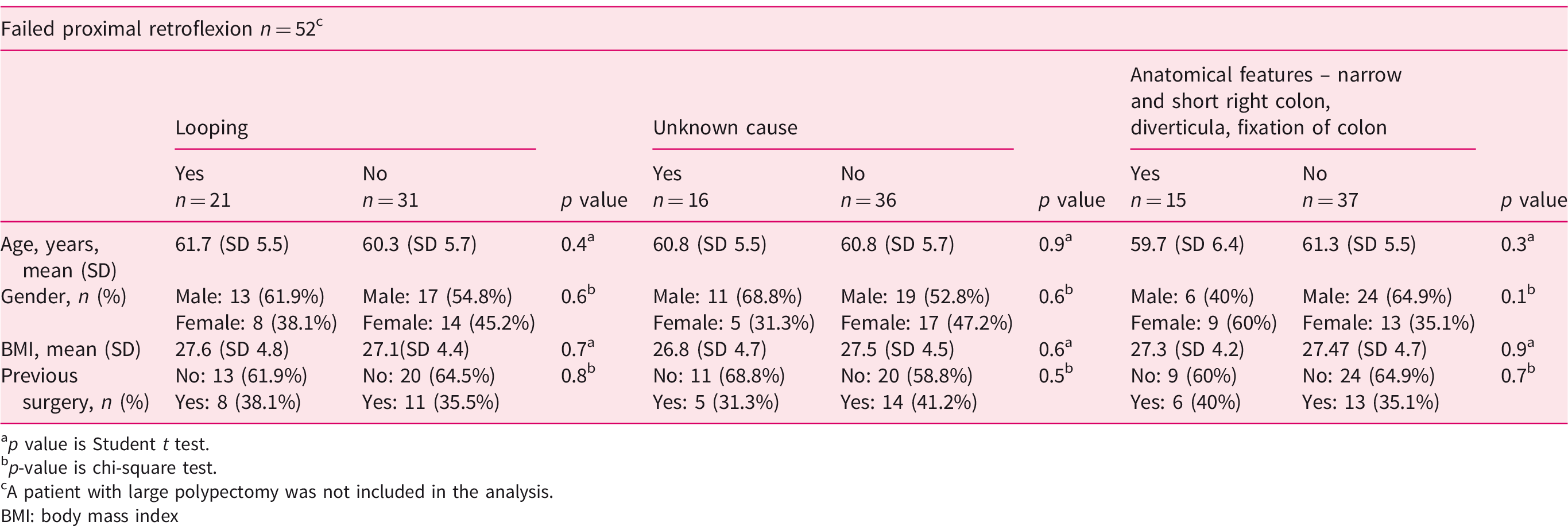
ap value is Student t test.
bp-value is chi-square test.
cA patient with large polypectomy was not included in the analysis.
BMI: body mass index
Findings at second examination
Table 4 shows the characteristics of colonoscopies and findings on the right side of the colon: 588 lesions (476 adenomas) were detected, 124 (90 adenomas) in the second pass (proximal retroflexion: n = 43 and forward view: n = 81). The right-side ADR was 30% on the first pass. In the second view (intention to treat analysis) the number of colonoscopies with ≥1 adenoma was 73, achieving an increase in ADR of 11%, without significant between-group differences (proximal retroflexion: 9% vs. forward view: 12%). The rate of missed polyps was 21% and AMR was 19%. In the per-protocol analysis, the total ADR was 61% and the total ADR in the right colon in the second pass was proximal retroflexion: 9.5% and forward view: 12%. There are no differences in the second examination withdrawal time related to the type of manoeuvre (proximal retroflexion: 1.66 vs. forward view:1.58) (p = 0.23).
Characteristics of colonoscopy and findings on the right side of the colon.
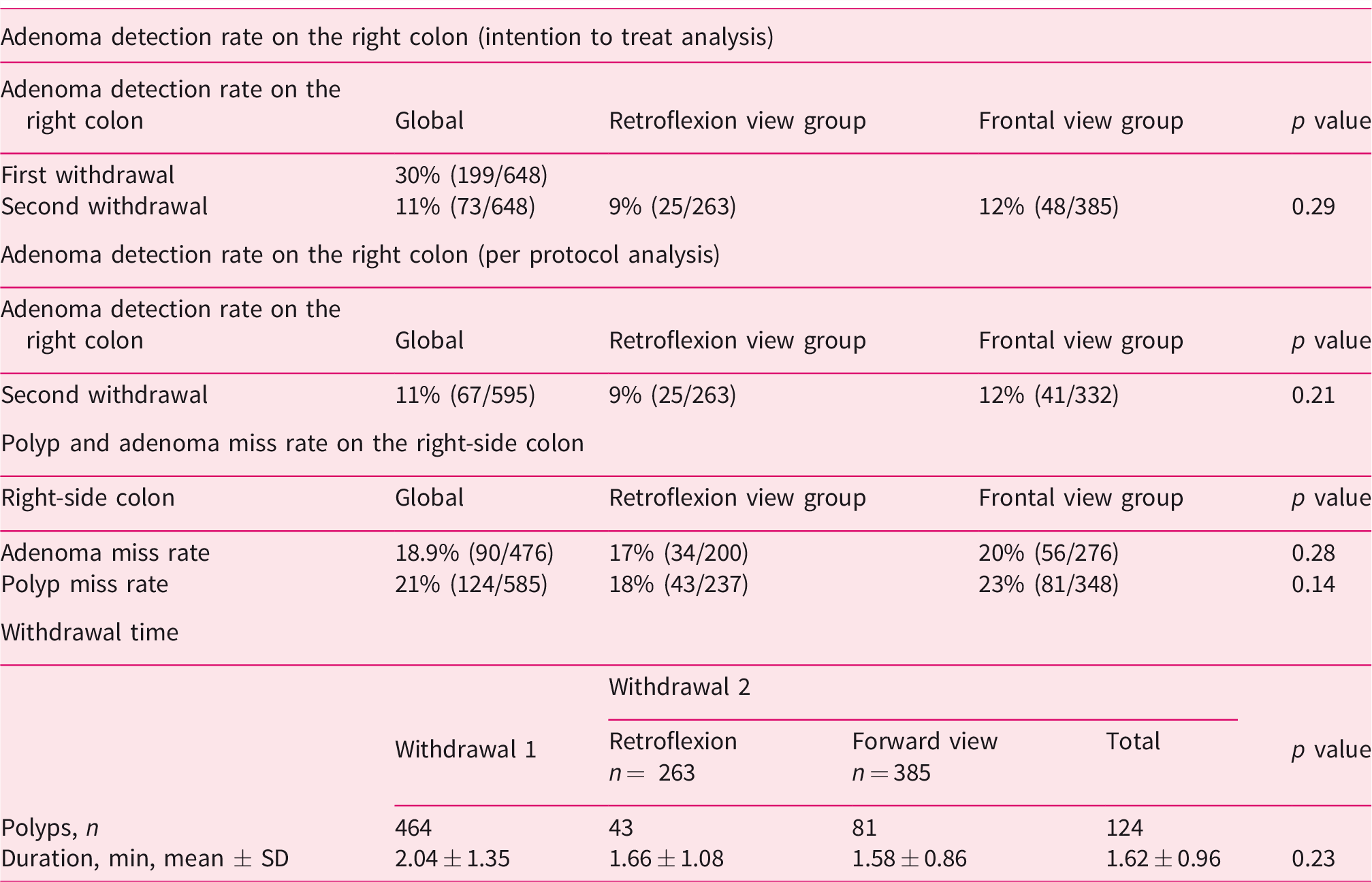
The proximal CRC and proximal advanced adenoma rates were 1.2% and 17.5% respectively, whereas the overall CRC and advanced adenoma rates were 3.5% and 27% respectively. The overall AMR was 12.9% in the proximal retroflexion group and 14.5% in the forward view group
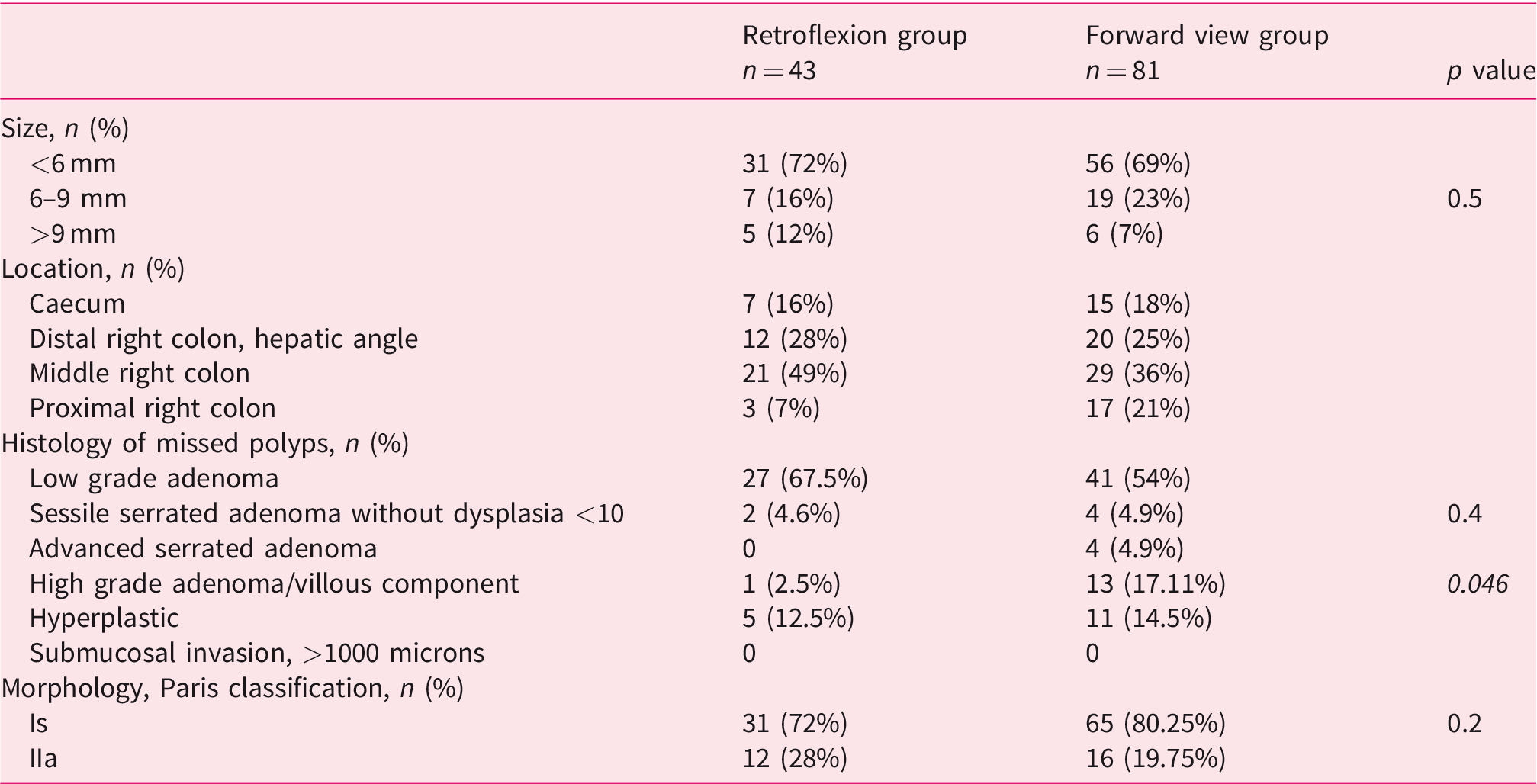
Table 5 describes the characteristics of the polyps not visualized in the first pass: they were predominantly <6 mm, low grade adenomas located in the middle right colon and the morphology according to the Paris classification was Is. We found no invasive neoplasia in the second exam. There were no differences between adenomas visualized by proximal retroflexion or forward view, except that forward view revealed 17% high-grade adenomas versus 2.5% in proximal retroflexion (p <0.05).
Characteristics of missed polyps.
A total of 49 right-sided sessile serrated lesions (SSLs) (10.3%) was found. Right-sided SSL rate was 11.1% (n = 10) at second examination: without dysplasia <10 mm (n = 6) and advanced SSL (n = 4) including: SSL with dysplasia, without dysplasia >10 mm and traditional serrated adenoma (p = 0.4).
In the 15.6% of patients in whom lesions were detected in the second examination (proximal retroflexion: 17% and forward view: 14.5%), endoscopic surveillance was modified by reducing the time of the next colonoscopy according to the European Society of Gastrointestinal Endoscopy (ESGE) guidelines. 23
We analysed the following pre-procedure variables that may influence the prevalence of precursor lesions in the right-side of the colon (Supplementary Material Table 1 online): sex, age, alcohol consumption, tobacco use and FIT value in which more detailed examinations will have to be performed using proximal retroflexion or second forward view. There was a weak association between age and alcohol. Descriptively, there were more polyps in men and smokers. FIT values were not associated with the number of polyps.
As the number of polyps was a variable with outlying values, Poisson robust regression was computed. To interpret the coefficients, quantitative variables (age, BMI, alcohol and FIT) were standardized using Z-scores. Three pre-procedure variables were significant: sex, alcohol and age. The sign of β (model coefficient) of the variable sex was negative, implying that the number of polyps detected was lower in women than in men (p<0.001). The number of polyps detected tended to increase in tandem with age and alcohol (p<0.001 and p = 0.028).
Discussion
The results of a multicentre study including patients from a FIT-based CRC screening show that it is necessary to perform a second examination at the right colon, but by which method does not matter, retroflexion or forward view. The success rate of proximal retroflexion was 83%. We had no complications with the retroflexed manoeuvre. Nevertheless, forward view is easier to perform so we recommend this method for a second right colon inspection.
In the 595 patients included under per protocol analysis, after a second pass, the ADR increased by 11% (proximal retroflexion 9% vs. forward view 12%, p = 0.21). The AMR was 19% (proximal retroflexion 17% vs. forward view 20%, p = 0.28). Previous studies with colonoscopies in tandem show that the AMR 24 and, therefore, interval cancer, were higher in the right colon. 7 Likewise, the AMR depended on the lesion size: the AMR was 6% in polyps ≥10 mm, 13% in polyps sized 6–9 mm and 27% in polyps ≤5 mm. 16
Regarding histology, polyps not detected in the first exploration were mainly low grade adenomas (54%), smaller than 6 mm in size and sessile. However, the second view revealed a significant percentage of advanced adenomas (17%). Their detection could be important to decrease interval cancer. Second forward view exploration revealed 17% high-grade adenomas versus 2.5% in retroflexion view. This could mean that retroflexion visualized smaller and non-advanced lesions hidden behind haustra folds than forward view. These results change surveillance recommendation, with a shortened follow-up time.
Kushnir et al. 18 found an AMR of 20% in patients undergoing screening and surveillance colonoscopies without differences between proximal retroflexion and second forward view, results similar to our and other studies. 17 The recent meta-analysis by Desai 19 found similar results to ours (second forward view of the right side colon increased ADR by 10% compared with 6% for retroflexion). However, our study differs from previous publications that analyse only positive FIT CRC screening populations.
In our study, an average additional procedure time of 1.6 min for second mucosal visualization is demonstrated without differences between the two groups. Approximately 25% of the patients included in each group presents BBPS 2 on the right-side colon; this could partly justify prolonging the procedure for mucosal cleaning. Our results are similar to those of the group of Kushnir 18 (1.4 min vs. 1.9 min, p<0.001). In Harrison et al., 17 a mean time of withdrawal in second exam was longer (4.7 min and 4.3 min). In this study proximal retroflexion included from the caecum to the splenic flexure.
In our cohort, we found higher rates of CRC and advanced adenoma compared with other groups with the same value for FIT cutoff, 20 µg/g faeces, for CRC screening; with a CRC detection rate of 0.6% and an advanced adenoma detection rate of 11.8%. 25 Kligman et al. 26 found in global positive FIT colonoscopy: 32.4% advanced adenomas and 0.96% CRC rate. It is important to notice that we found at right-side colon 1.2% with CRC (CRC is diagnosed in 3.46% of the 692 patients included) and 17.5% advanced neoplasm (global rate 27%). Results of the ADR differ in screening positive FIT colonoscopy (72.9%, 26 53.6% 27 and 61% in our study). We increase the ADR by 11% in a second right colon exploration; this could decrease post-colonoscopy colorectal cancer. It is very important to continue to focus on strategies and advanced technique in polyp detection to improve ADR in the average risk population.
Factors associated with an increase in the number of lesions in the right colon included older age, male sex and alcohol consumption. We found an increase in the number of polyps detected in the right colon in the second pass in patients with the highest number of polyps in the first pass.
Polyps not detected in the first exploration were located in the middle of the ascending colon in both study groups. During the second examination, more lesions were detected by forward view than by retroflexion in the proximal right colon and caecum (21% vs. 7%). This is logical as the caecum is not visualized correctly by retroflexion because this is the area in which the endoscope bends. 28
Studies show increased lesion detection by proximal retroflexion, which ranges between 2%, 13 5.1% 22 and 9.8%, 21 and an increased ADR after a second pass. 17 , 18 Lee et al. found an increased ADR with proximal retroflexion performed after two passes in forward viewing. 15 Desai et al. 19 concluded that a second pass of the right colon increased the ADR, whatever the method used.
Most studies agree that retroflexion causes no complications other than those inherent to colonoscopy, although some reports have shown an increase of 0.03% in adverse events. 20 , 29 The most common cause of failure of retroflexion is a caecum arrival with a loop during the insertion of the endoscope, while others include anatomic difficulties. 13 , 21 In our cohort, the causes of failure were most likely due to: endoscopic looping (39.6%), anatomic features (24.3%) and unknown causes (33.9%). We do not find any association with these causes of failure and previous surgery, age, BMI and gender.
Experts defend proximal retroflexion as safe and essential for the resection of some polyps 28 , 30 and suggest every endoscopist should know how to use it in normal practice.
Proximal retroflexion caused no complications and the success rate was 83%, in line with reported rates of 82.4–91.9%. 13 , 15 , 21 The learning curve of participating endoscopists showed a progressive increase in the success rate of retroflexion over time. All endoscopists had an ADR of >40%, the minimum established for screening colonoscopy from a FIT-based CRC screening, 31 although some included < 20 subjects, meaning their ADR should be interpreted with caution, as well as retroflexion success rate.
The study had some limitations. First, the study was not blinded, as the endoscopists were aware of the technique they were using, which could have led to greater efforts to detect polyps with a specific technique, as well as they could have prolonged the inspection time to achieve quality exploration times. Also, it could be a risk of bias, as endoscopists were aware at the first pass that there would be a second pass. Several endoscopists participated, making the results more heterogeneous, since there were differences related to the evaluator (per-endoscopist level), not only to the exploratory manoeuvre used. However, this may suggest greater reproducibility of the results in usual practice. The absence of a third arm (neither retroflexion nor second view) is an inherent limitation in the study design; future studies are necessary in this regard.
The strength of the study is that it was a randomized controlled trial and it was carried out in the CRC screening programme with positive FIT.
Studies with a larger sample size are needed to confirm these results.
In conclusion, re-examination of the right-side colon should be considered in patients referred for CRC screening colonoscopy, at least in older men with alcohol consumption and those with a high number of polyps in the first examination. In all patients with new polyps discovered after a second view, the surveillance recommendation would be changed in 15.6% of cases, the follow-up time being shortened.
Supplemental Material
sj-pdf-1-ueg-10.1177_2050640620924210 - Supplemental material for Proximal retroflexion versus second forward view of the right colon during screening colonoscopy: A multicentre randomized controlled trial
Supplemental material, sj-pdf-1-ueg-10.1177_2050640620924210 for Proximal retroflexion versus second forward view of the right colon during screening colonoscopy: A multicentre randomized controlled trial by Ma Henar Núñez Rodríguez, Pilar Díez Redondo, Fausto Riu Pons, Marta Cimavilla, Luis Hernández, Andrea Loza and Manuel Pérez-Miranda in United European Gastroenterology Journal
Footnotes
Acknowledgement
ClinicalTrials.gov (NCT03041532).
Declaration of conflicting interests
The authors have no conflicts of interest to declare.
Ethics approval
The study was approved by the Rio Hortega Hospitals Ethical Board (6 June 2017, CEIC: 62/16) and the respective ethics committees.
Informed consent
Written informed consent was obtained from patients who agreed to participate in the study. CEIC 62/16
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Gerencia Regional de Salud de Castilla y León (grant number GRS 1240/A/16).
Supplemental material
Supplemental Material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.