
Abstract
Background and aims
Several studies have shown improved short-term outcome with endoscopic transmural drainage and necrosectomy for the treatment of walled-off pancreatic necrosis. However, knowledge on the long-term prognosis after such treatment is limited. The aim of present study was to evaluate long-term outcomes in patients endoscopically treated with transmural drainage and necrosectomy.
Methods
We retrospectively follow up 125 patients with walled-off pancreatic necrosis treated with endoscopic transmural drainage and necrosectomy in 2010–2017. All patients received plastic pigtail stents and nasocystic catheter. Additional external drainage was performed in 41 patients. Main outcomes were survival, pancreatic function, development of co-morbidities, ability to work and social status.
Results
During a median follow-up of 4.3 years, nine (7%) patients died. Seven deaths were unrelated to pancreatic disease, and two patients died of pancreatic cancer. Twenty-two (18%) patients developed exocrine pancreatic insufficiency. Thirty-six (32%) previous non-diabetics developed endocrine insufficiency. Endoscopic necrosectomy during admission (odds ratio (OR) = 1.28, 95% confidence interval (CI) 1.05–1.56; p = 0.015) and therapy on the main pancreatic duct (OR = 8.08, 95% CI 2.43–26.9; p < 0.001) during follow-up predicted development of exocrine insufficiency. Severity on computed tomography predicted endocrine insufficiency (OR = 1.61, 95% CI 1.24–2.09; p < 0.001). Most patients regained their working capacity and preserved their marital status.
Conclusions
This study provides robust data on the long-term outcome of patients with walled-off pancreatic necrosis treated with endoscopic transmural drainage and necrosectomy. The favourable outcomes on survival, pancreatic function and social status support current recommendations of endoscopic transmural drainage and necrosectomy being the treatment of choice for walled-off pancreatic necrosis.
Introduction
About 10% of patients with acute pancreatitis (AP) develop necrosis of the pancreatic parenchyma, the peripancreatic tissue or both. With time, the necrosis becomes surrounded by a thick fibrous capsule and is then called a walled-off necrosis (WON). 1 Patients with WON often experience a protracted disease course with infectious and vascular complications and varying degrees of organ failure. 2 In the last 15–20 years, several minimally invasive techniques for drainage and necrosectomy have been developed, replacing open surgery as first-line treatment.3,4A recent randomised study has recommended endoscopic transgastric drainage and necrosectomy (ETDN) as the primary treatment modality for WON. 5 Although several studies have shown improved short-term outcomes with the endoscopic approach for the treatment of WON, knowledge on long-term survival, pancreatic function, development of co-morbidities, ability to work and social status is limited. The aims of the present retrospective study were to assess these long-term outcomes in a well-defined cohort of WON patients treated with ETDN and to evaluate risk factors for development of exo- and endocrine pancreatic insufficiency.
Methods
All patients referred to us with WON from January 2010 to December 2017 were screened for inclusion. We included patients treated with ETDN within 90 days from the start of AP and without known chronic pancreatic disease from January 2010 to December 2017. Patients lost to follow-up (FU) within the first 12 months after hospital discharge were excluded. Data were retrospectively collected by reviewing electronic patient charts. During the inclusion period, 214 patients were referred to our department with pancreatic collection and were thus screened for potential inclusion. Of these patients, 161 were eligible for further analysis (Figure 1).
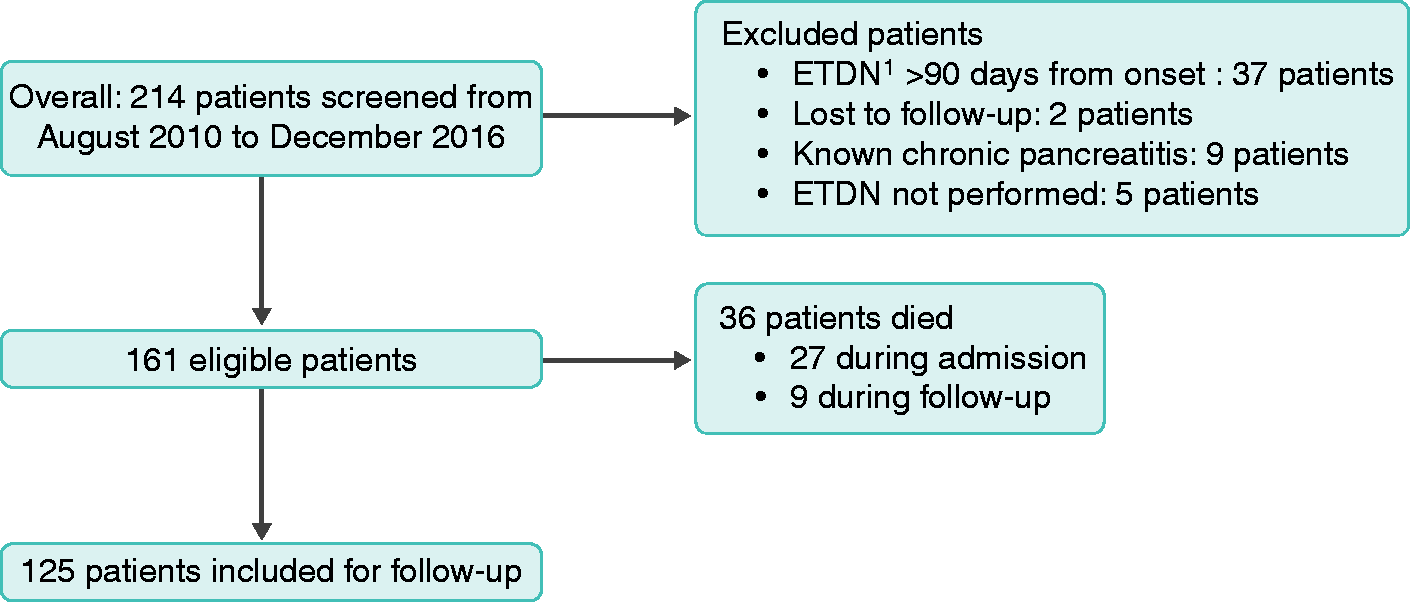
Flow diagram showing patient screening and inclusion process. 1 Endoscopic transgastric drainage and necrosectomy.
We collected data on age, sex, date of onset of AP, aetiology, exo- and endocrine pancreatic insufficiency, use of analgesics, American Society of Anesthesiologists (ASA) score, 6 Charlson Comorbidity index (CCI), 7 tobacco and alcohol use, social and working status, indication for ETDN, date of index procedure, number of dilations, number of necrosectomies, total number of procedures, external drainage, infectious status of necrosis, computed tomography (CT) severity index (CTSI), 8 modified CTSI (mCTSI), 9 WON-related admissions, non-WON-related admissions, need for endoscopic retrograde pancreatography (ERP) and death (Figure 2).
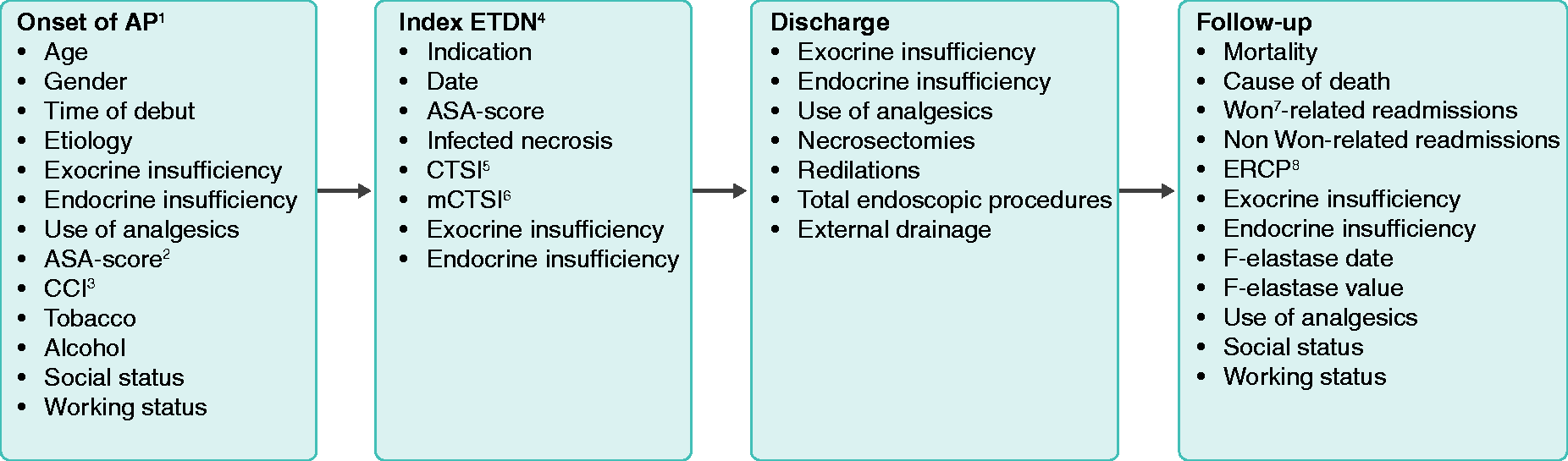
An overview of extracted data at different time points. 1 Acute pancreatitis. 2 American Society of Anesthesiologists score. 3 Charlson Comorbidity index. 4 Endoscopic transgastric drainage and necrosectomy. 5 CT severity index. 6 Modified CT severity index. 7Walled off necrosis. 8 Endoscopic retrograde cholangiopancreatography.
Endoscopic procedure
As described previously, 2 endosonography-guided transgastric or transduodenal drainage was performed using a curved linear array echoendoscope Olympus GF-UCT140-AL5 or GF-UCT180/Aloka SSD 5000 or ProSound Alpha 7 by (a) needle puncture (ECHO-19;Cook Medical, Bloomington, IN), (b) fluid aspiration for microbiological diagnostics, (c) insertion of a guidewire (0.035″ Dreamwire; Boston Scientific, Marlborough, MA) through the needle, (d) needle knife incision over the wire (Huibregtse Triple Lumen; Cook Medical), (e) balloon dilation of the tract (CRE Wireguided 12–20 mm; Boston Scientific), (f) placement of two double pigtail stents (Zimmon 7 Fr/6 cm; Cook Medical) and a nasocystic catheter (7-Fr nasal biliary drainage set; Cook Medical) for subsequent irrigation of the cavity and (g) endoscopic debridement of loose necrotic material using a therapeutic gastroscope (Olympus GIF-1TQ160/XTQ160) and tripod, stone retrieval basket or polypectomy snare (used in most cases). A small dilation balloon diameter was usually chosen at the index procedure and when there was an increased risk of bleeding from collaterals, for example in cases with splenic vein thrombosis. Endoscopic necrosectomy was usually not performed during the index procedure. Additional placement of percutaneous catheters was done in cases of widely expanding peripancreatic collections that were not accessible by the endoscopic route alone. All endoscopies were performed with CO2insufflation. Irrigation of the collections through nasocystic and/or percutaneous catheters was done three to six times a day. The irrigation volume depended on the size of the collection, usually 100–250 mL per procedure. Antibiotics (gentamicin, vancomycin or amphotericin B) were added to the irrigation fluid according to the microbiological findings. The endoscopic sessions with re-dilation of the transmural tract and necrosectomy were repeated at weekly intervals until the necrotic cavity was free of debris and vital granulation tissue was seen. At that time, the nasocystic catheter was removed. Necrosectomy was indicated when the patient did not improve or showed clinical deterioration despite dilation and lavage. The pigtail stents were removed one year after the index procedure. All procedures were performed by three experienced endoscopists (P.N.S., E.F.H. and S.N.), who all have an extensive experience in endoscopic ultrasound-guided drainage of pancreatic collections.
Definitions
WON was defined as a mature, encapsulated collection of pancreatic and/or peripancreatic necrosis that presented with a well-defined inflammatory wall. 1 The procedure of endoscopic drainage and subsequent necrosectomy has been described previously. 2 Exocrine insufficiency was defined as need for pancreatic enzyme replacement therapy (PERT). Endocrine insufficiency was defined as need for either peroral antidiabetics or insulin. Use of pain killers was stratified according to the World Health Organization 10 and classified as no use, use of non-opioids, use of mild opioids and use of strong opioids.
Statistics
The analyses were performed with STATA v15 (StataCorp, College Station, TX). Continuous data are expressed as medians with range, and categorical data as proportions. To test for differences between groups, we used the Mann–Whitney U-test or Fischer’s exact test.
Uni- and multivariate logistic-regression were used to assess predictors of exo- and endocrine insufficiency. Cox regression was used for analysis of mortality. Results are presented as crude and adjusted odds ratios (OR) or hazard ratios (HR) with 95% confidence intervals (CI). The Kaplan–Meier curve was further used to evaluate mortality.
Ethics
This study was approved by the Danish data protection agency on 27 July 2018 (j.nr.: VD-2018-256). As this was a retrospective study, approval from the ethics committee was not needed, according to Danish legislation. Likewise, patient consent was not obtained.
Results
The median age was 59 years, 55% of patients were male and gallstone aetiology predominated (Table 1). The median time from onset of symptoms to the index endoscopy was 32 days. At the index procedure, 79% had infected necrosis, and the median mCTSI was 10. The median number of endoscopic procedures before resolution of WON was four, and endoscopic necrosectomy was performed in 95 patients. Forty-one patients were treated with external drainage in addition to endoscopic treatment. Of 161 patients, 27 (16.8%) died during admission (Figure 3). Of the 134 initial survivors, nine (7%) patients died during FU. The cause of death during FU was pancreatic cancer in two patients, pulmonary cancer in one, septic shock in one, pneumonia and multiple-organ failure in two and an overdose of insulin and methadone in one patient. In two patients, the cause of death was unknown. For death during FU, alcohol abuse at the onset of AP was a significant predictor of mortality (HR = 4.89, 95% CI 1.31–18.3; p = 0.02) in univariate analysis but not in multivariate analysis.
Baseline data of 161 patients with walled-off pancreatic necrosis eligible for follow-up.
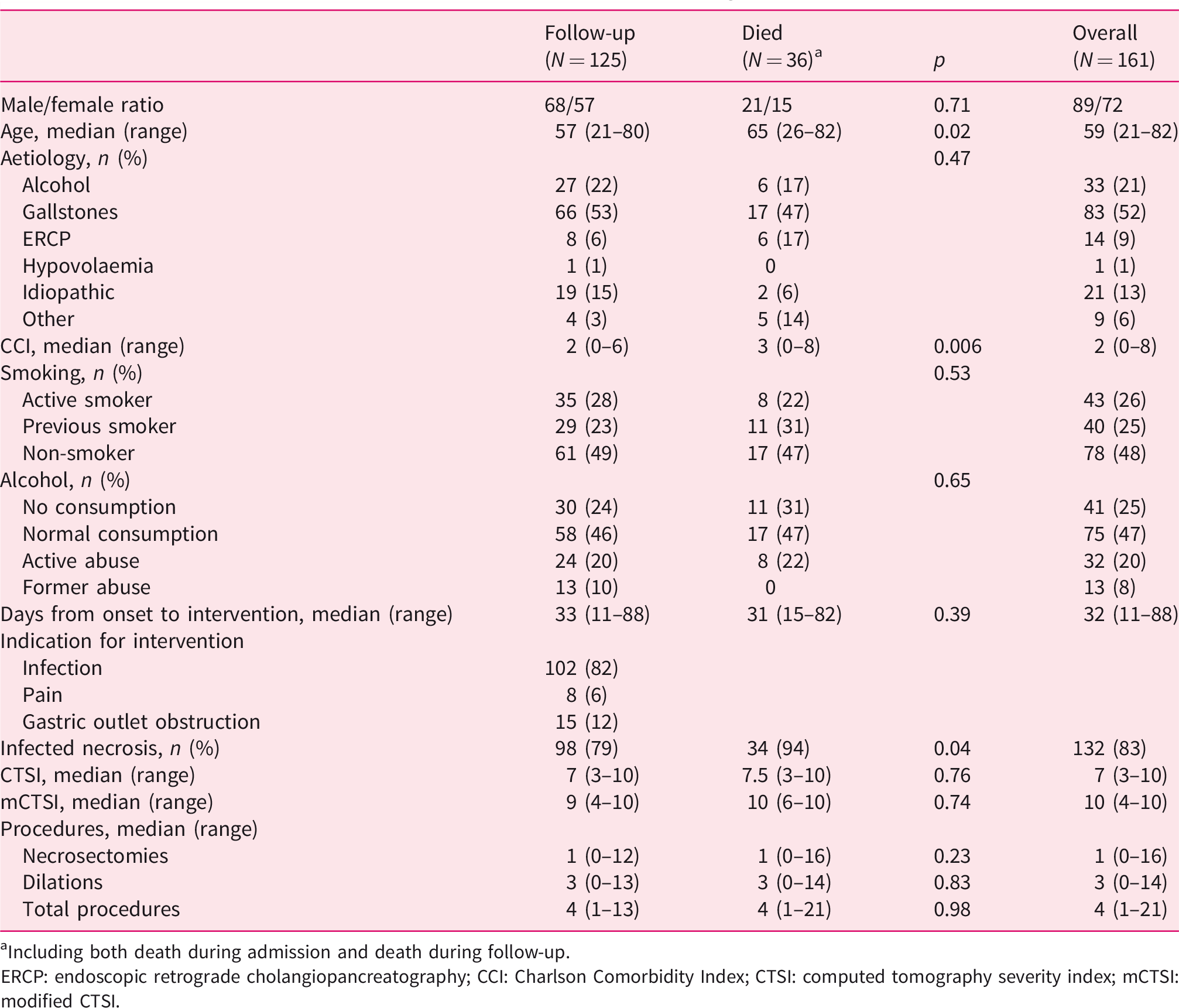
Including both death during admission and death during follow-up.
ERCP: endoscopic retrograde cholangiopancreatography; CCI: Charlson Comorbidity Index; CTSI: computed tomography severity index; mCTSI: modified CTSI.
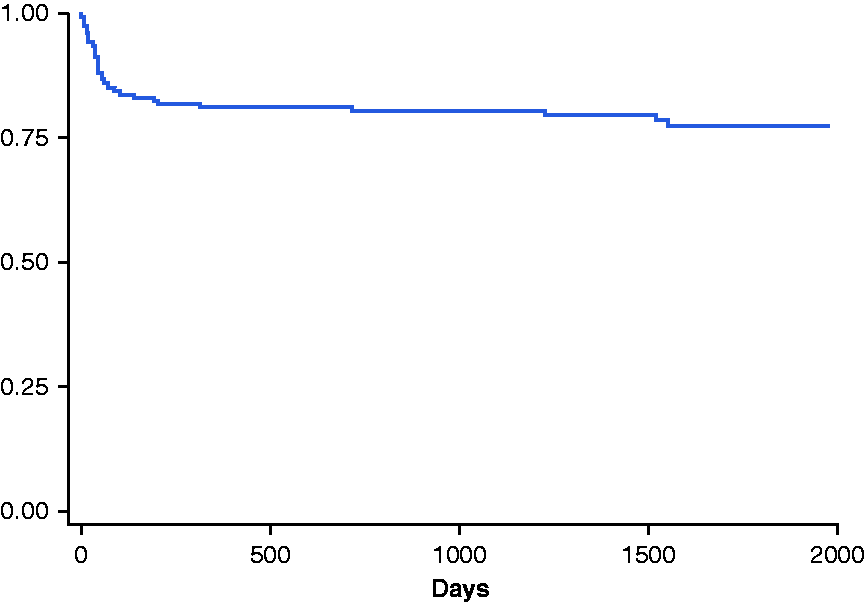
Survival estimates in all 161 patients with walled-off necrosis undergoing endoscopic, transgastric drainage and necrosectomy.
The median FU of the 125 patients who survived was 4.3 years (range 1.2–9.1 years). Data on pancreatic function, use of analgesics and social and working status during FU are shown in Table 2. Forty-five (36%) patients had one or more WON-related readmissions, and 50 (40%) patients had one or more non-WON-related readmissions. Eighteen (14%) patients needed endoscopic treatment with ERP, mainly due to newly developed strictures of the main pancreatic duct.
Outcome in 125 patients eligible for long-term follow-up.
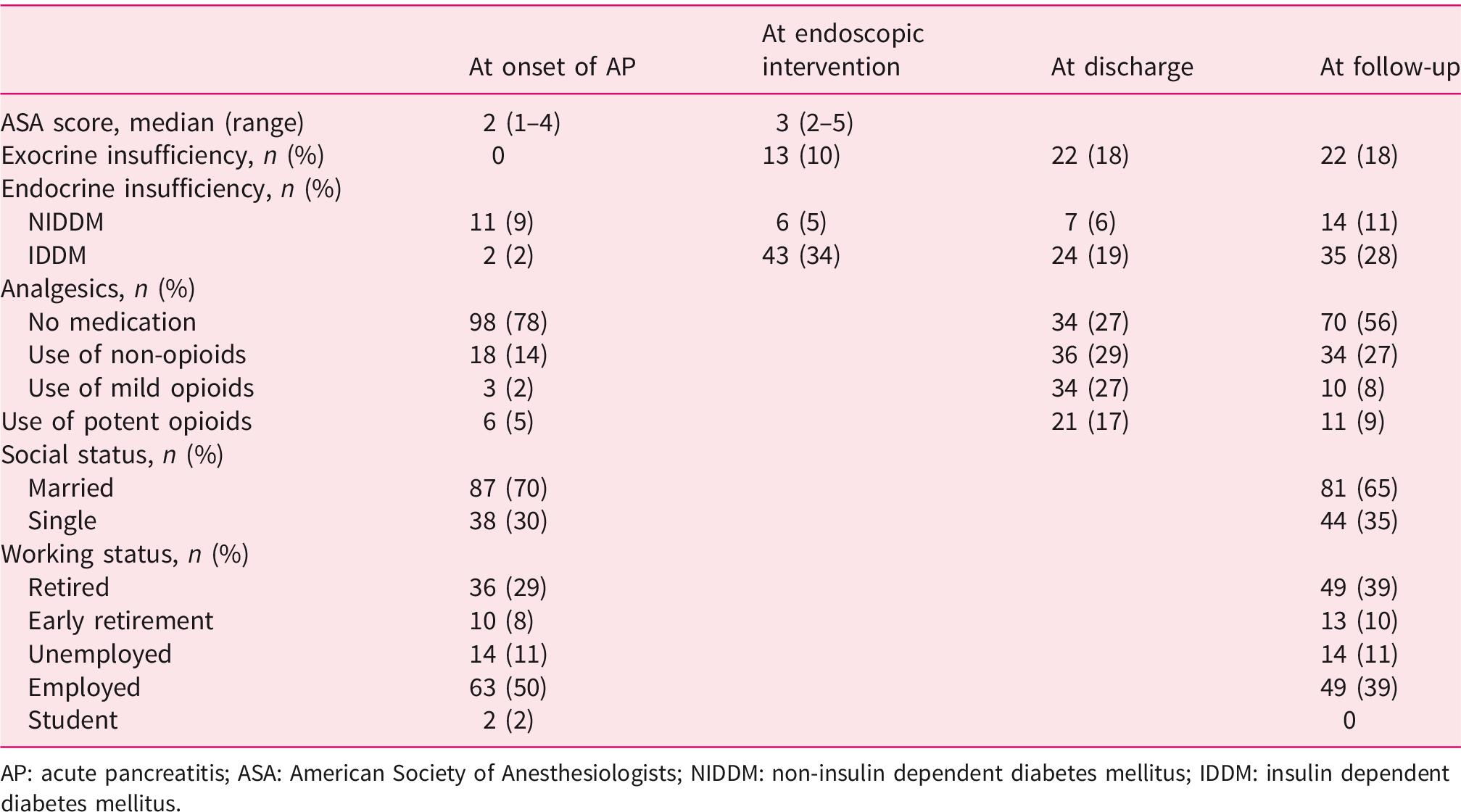
AP: acute pancreatitis; ASA: American Society of Anesthesiologists; NIDDM: non-insulin dependent diabetes mellitus; IDDM: insulin dependent diabetes mellitus.
Twenty-two (18%) patients were on PERT at discharge. This number remained unchanged during FU. Twelve patients stopped PERT during FU, as they regained their exocrine function, while 12 other patients developed exocrine insufficiency and started PERT.
The proportion of patients with diabetes increased from 10% at onset of AP to 25% at discharge and 39% at FU. Thirty-five (71%) patients with diabetes at FU needed insulin. All 24 patients who were treated with insulin at discharge were also on insulin therapy at FU. Furthermore, five of the patients who were treated with peroral antidiabetics at discharge and 11 patients who did not receive any kind of antidiabetics were on insulin therapy at FU.
At onset of AP, nine (7%) patients were already using opioids. This proportion significantly increased to 44% (p < 0.001) at discharge. At FU, 17% of the patients needed opioids – a proportion significantly lower than at discharge (p < 0.001).
Seventy per cent of the patients were either married or in a relationship at the onset of AP. During FU, this number slightly decreased to 65%, the difference being non-significant. Fifty per cent of the patients were employed at the onset of AP, and 29% were retired. At FU, the percentages were 39% and 39%, respectively. The proportion of early retired or unemployed patients was unchanged.
In univariate logistic regression (Table 3), the need for ERP (p<0.001) was a significant predictor for development of exocrine insufficiency. In multivariate analysis (adjusted for age, sex, aetiology, smoking and infected WON), the need for ERP (p < 0.001) and number of endoscopic necrosectomies (p = 0.015) predicted development of exocrine insufficiency.
An overview of predictors of exo- and endocrine insufficiency during follow-up in patients with walled-off pancreatic necrosis.
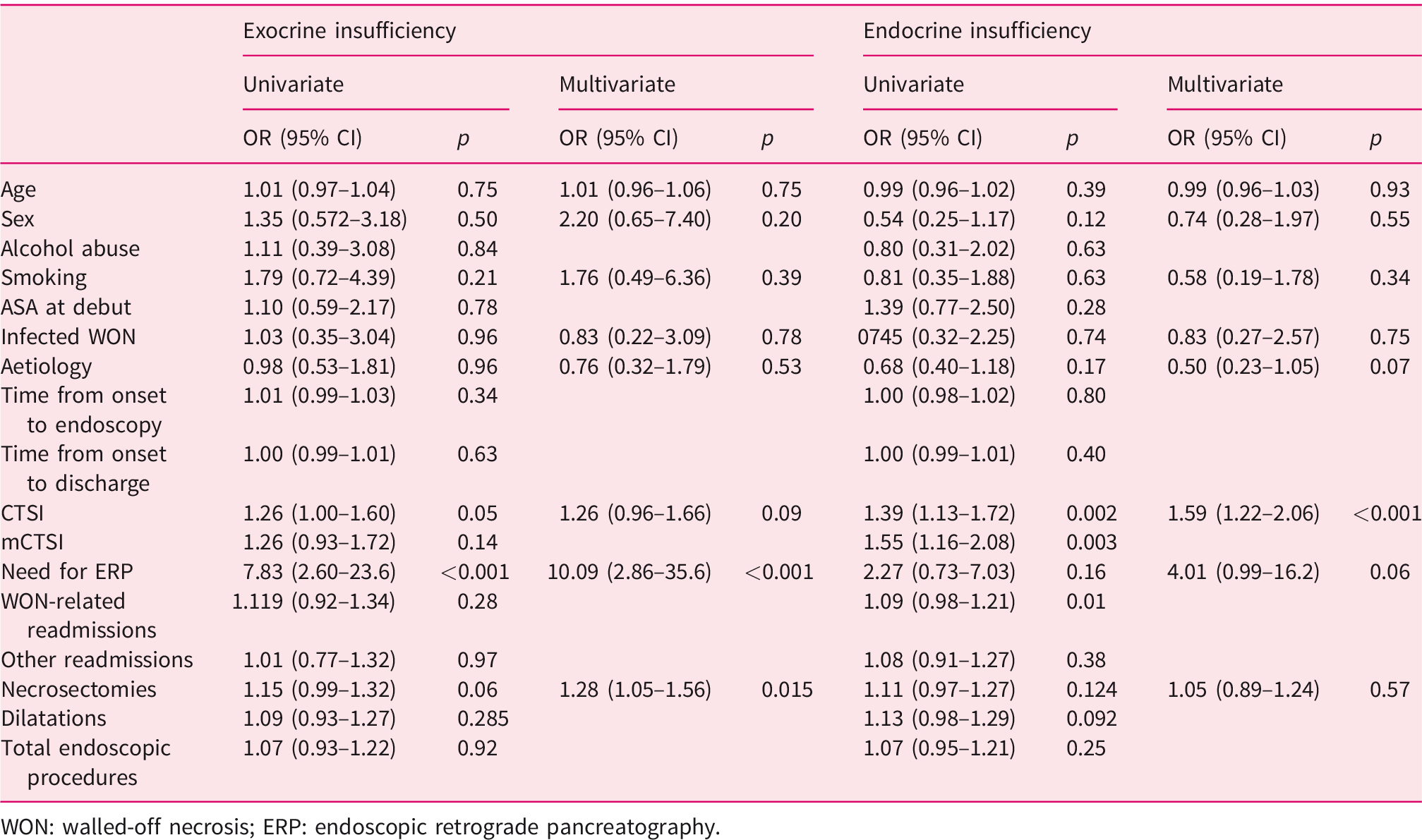
WON: walled-off necrosis; ERP: endoscopic retrograde pancreatography.
CTSI (p < 0.001) predicted development of endocrine insufficiency in univariate and multivariate analysis. mCTSI also predicted development of endocrine insufficiency in multivariate analysis (p < 0.001).
Discussion
In this study, we evaluated 161 patients with WON treated with ETDN in a tertiary referral centre, of whom 125 were eligible for evaluation of long-term outcome. With a median FU of 4.3 years and a sizable number of patients, this study provides robust data on the long-term outcome of WON patients treated endoscopically.
The mortality during FU was 7%. Two of the nine patients who died during FU died of pancreatic cancer. Both patients were initially classified as idiopathic causes of AP, while more thorough diagnostic and imaging work-up during FU in these patients seems rational.
The prevalence of exocrine insufficiency during FU was 18%, which is in accordance with a previous study (17%), 11 while others have reported a considerable higher prevalence (33%). 12 In almost half of the patients needing PERT at discharge, the treatment was discontinued during FU, suggesting a possible reversibility in pancreatic exocrine function. On the other hand, approximately half of the patients needing PERT at FU were not on prescribed medication until after discharge, predominantly within the first year, making evaluation of exocrine function during FU mandatory. Due to the retrospective design, data on faecal elastase were missing in a significant number of patients and were not included in the assessment of exocrine insufficiency.
Diabetes was the most prevalent long-term complication, occurring in almost 40% of the patients compared to 25% at discharge and 11% at the onset of AP. Both CTSI and mCTSI were significant predictors of development of endocrine insufficiency, probably reflecting an association between the extent of the pancreatic parenchymal necrosis and loss of endocrine function.
Only 17% of patients were treated with opioids at FU compared to 34% at discharge and 7% at the onset of AP. This proportion was less than reported earlier in a similar group of patients (43%). 12 The working and marital status remained almost unchanged during the disease course. Regrettably, due to the retrospective design, we were not able to evaluate the quality of life in this group of patients. A recently published retrospective study, which included health-related quality of life data on 41 patients treated endoscopically for WON, found that these patients tended to preserve life quality during FU. 12 Our data on social and working status support this.
Endoscopic necrosectomy during admission and need for ERP due to main pancreatic duct abnormalities (primarily stenosis of the duct) during FU were significant predictors of exocrine insufficiency. This finding probably reflects disease severity, loss of pancreatic parenchyma and intraductal hypertension in this subgroup of patients.
To our knowledge, this is the largest study published so far with long-term data on patients with WON treated endoscopically. Only patients with their first attack of AP were included, and all patients were treated according to a standardised treatment protocol. Evaluation at four different time points across the different disease phases provides a unique insight into the course of necrotising pancreatitis.
Our findings must be interpreted cautiously due to several limitations, most importantly the retrospective design and data collection. This was a single, tertiary referral centre study, offering ETDN as a primary modality, thus rendering it difficult to extrapolate our findings to other health-care settings with differing procedural modalities. We defined exo- and endocrine insufficiency based on need for PERT and antidiabetics/insulin. This entails a risk of underestimating the number of patients with these insufficiencies, whereas direct pancreatic function testing or measurement of glycated haemoglobin or C-peptide might have resulted in a more accurate evaluation. In a prospectively designed study, a more detailed evaluation of micronutrients, bone metabolism, body composition, muscle function and quality of life will add further knowledge to pancreatic function following episode of WON. Furthermore, this subgroup of patients may serve as an ideal population studying progression from acute to chronic pancreatitis.
In conclusion, this study demonstrated a favourable outcome of endoscopic treatment of WON as evaluated by survival, pancreatic function and social status, and thus supports current recommendations of ETDN being the treatment of choice in this patient group.
Footnotes
Ethics approval
This study was approved by the Danish data protection agency on 27 July 2018 (j.nr.: VD-2018-256). As this was a retrospective study, approval from the ethics committee was not needed, according to Danish legislation.
Declaration of conflicting interests
The authors have no conflicts of interest to declare.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed consent
Patient consent was not obtained.