
Abstract
Background
Anti-tumour necrosis factor alpha agents (anti-TNF-α) have been widely used in patients with inflammatory bowel disease (IBD). However, few published meta-analyses have focused on timing of the last infusion before surgery. We evaluated the relationship between preoperative anti-TNF-α timing and postoperative surgical site infection to provide additional evidence for surgeons to choose appropriate dates for surgery.
Methods
We searched from inception until January 2019 for studies that documented postoperative complications of adults with IBD who underwent preoperative anti-TNF-α treatment. Primary outcomes of included studies were the odds ratios of preoperative anti-TNF-α time frames (4, 8 and 12 weeks). In addition, surgical site infection and its subtypes (anastomotic leakage, abscesses and wound infection) were analysed.
Results
Twenty-seven publications were included. No significant difference between anti-TNF-α and control cohorts was observed for most postoperative surgical site infections (or its subtypes) when the preoperative anti-TNF-α infusion time window was within 4, 8 or 12 weeks. Additionally, no significant difference in postoperative complications was observed between preoperative anti-TNF-α windows of within four weeks and more than four weeks.
Conclusions
In terms of surgical site infection and its subtypes, anti-TNF-α may be safe for ulcerative colitis and Crohn’s disease patients who receive their last infusion of anti-TNF-α more than four weeks before surgery. We also found no evidence that anti-TNF-α was a risk factor when administered within four weeks, with the exception of subgroup results from a single study. Stratified by time window, use of anti-TNF-α until surgery has the potential to become a more considered strategy in clinical practice.
Keywords
Introduction
Inflammatory bowel disease (IBD) is an intestinal immune disease that includes ulcerative colitis (UC), Crohn’s disease (CD) and unclassified IBD. Biologics, especially anti-tumour necrosis factor alpha agents (anti-TNF-α), have in recent years become widely used in the clinical setting to control disease progression in patients with IBD. However, anti-TNF-α treatment fails in some patients, who develop uncontrollable bleeding, intestinal obstruction or other symptoms requiring surgical intervention.1,2 During the past 30 years, > 30% of patients with CD have undergone surgery. 3 This proportion is lower in patients with UC. Preoperative serum levels of anti-TNF-α may be related to postoperative complications. 4 Moreover, the interval between preoperative anti-TNF-α use and surgery can reflect preoperative anti-TNF-α serum level to some extent. Thus, the timing of surgery may be closely related to the development of postoperative complications in patients treated with anti-TNF-α.
The results of published meta-analyses are controversial. Some reported that anti-TNF-α increased the incidence of postoperative infectious complications,5,6 while another found that anti-TNF-α increased early pouch-specific complications. 7 Other studies asserted that anti-TNF-α did not increase postoperative complications.8–10 However, researchers have usually focused on either the type of complication5,6,8,9 or the type of surgery, 7 whereas few studies have discussed surgical site infection (SSI) or the duration of the preoperative anti-TNF-α infusion window (preoperative anti-TNF-α window). 10 Various preoperative time frames ranging from two weeks to more than one year have been examined in previous studies. However, the effects of anti-TNF-α are relatively short-lived, 11 which might lead to high heterogeneity and controversial results among published meta-analyses.
To provide additional evidence for surgeons to choose the most appropriate timing for surgery, this study evaluated the relationship between the reoperative anti-TNF-α window and development of postoperative SSI through data regrouping and meta-analysis.
Methods
Search strategy and study selection
The MeSH terms ‘inflammatory bowel diseases’ (along with ‘Crohn’s disease’ and ‘colitis, ulcerative’), ‘postoperative complications’ and ‘tumour necrosis factor-alpha’ (along with ‘infliximab’, ‘golimumab’, ‘adalimumab’ and ‘certolizumab pegol’) and their entry terms were used to retrieve publications from PubMed, EMBASE, Cochrane Library and Web of Science databases from inception until 6 January 2019.
Inclusion criteria were: (a) patients underwent surgery for IBD, (b) the experimental group used at least one anti-TNF-α, (c) the preoperative anti-TNF-α window was clearly reported and (d) 30-day postoperative complications were reported. Exclusion criteria were: (a) the study focused on paediatric patients, (b) the report lacked access to original data or (c) the report was a version of a conference document for a published study that was already included. After removal of duplicate publications, we performed a preliminary selection of studies by looking through the titles and abstracts. We then reviewed the full text of each study for secondary screening. All publications were selected according to inclusion and exclusion criteria.
Data extraction
We extracted the details of each study by recording the journal, country, inclusion period and research centre; population distribution, age, sex and type of anti-TNF-α; concomitant medications, preoperative anti-TNF-α window and type of surgery; and the details of postoperative complications. Until this step (including study selection and data extraction), two researchers (Y.Q. and Z.Z.) worked separately. After comparing the results, findings were discussed to reach a consensus or referred to a third researcher for a conclusion in cases of disagreement.
Outcomes assessed
Two comparisons were performed. Comparison I was performed to compare anti-TNF-α–treated and untreated groups. We established three time frames for the preoperative anti-TNF-α window based on the original study: within 4 weeks, within 8 weeks and within 12 weeks. Comparison II was performed to compare patients administered anti-TNF-α within four weeks preoperatively with patients administered anti-TNF-α more than four weeks preoperatively. All of the above comparisons focused on SSI and its major causes. Diseases in the original studies were evaluated in a subgroup format.
Definition of SSI
An SSI was defined as an open wound or purulent discharge into an organ or space, with bacterial culture or other evidence indicating that the infection originated in the surgical area. SSI included both superficial SSI and deep SSI. Wound infection is a major cause of superficial SSI, while anastomotic leakage and abscess formation are the major causes of deep SSI (other causes include pelvic sepsis and fistulas).
Statistical analysis
We used Review Manager v5.3 (Cochrane Collaboration, London, UK) for statistical analysis using the Mantel–Haenszel analysis method. Odds ratios (OR) and 95% confidence intervals (CI) are shown. The I2 test was used to evaluate heterogeneity. I2 of ≤ 50% was defined as acceptable heterogeneity. 12 When unacceptable heterogeneity was encountered, a sensitivity analysis was performed to detect sources of heterogeneity. As some comparisons exhibited large heterogeneity (I2 > 50%), this was not conducive to the application of the fixed-effects model. Thus, all forest plots used the random-effects model. The Study Quality Assessment Tool was used for quality assessment of studies (https://www.nhlbi.nih.gov/health-topics/studyquality-assessment-tools). Our work was performed following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (www.prisma-statement.org/).
Results
In total, 1441 publications were retrieved. Of these, 234 were removed due to duplication. After screening the titles and abstracts, 1136 publications were excluded. Next, 44 publications were excluded after reviewing the full text. Finally, 27 publications were included in this review.13–39 Ten publications focused on CD, 10 focused on UC and seven focused on mixed IBD. A flow chart of the study selection process is shown in Figure 1.
Flow diagram of study selection.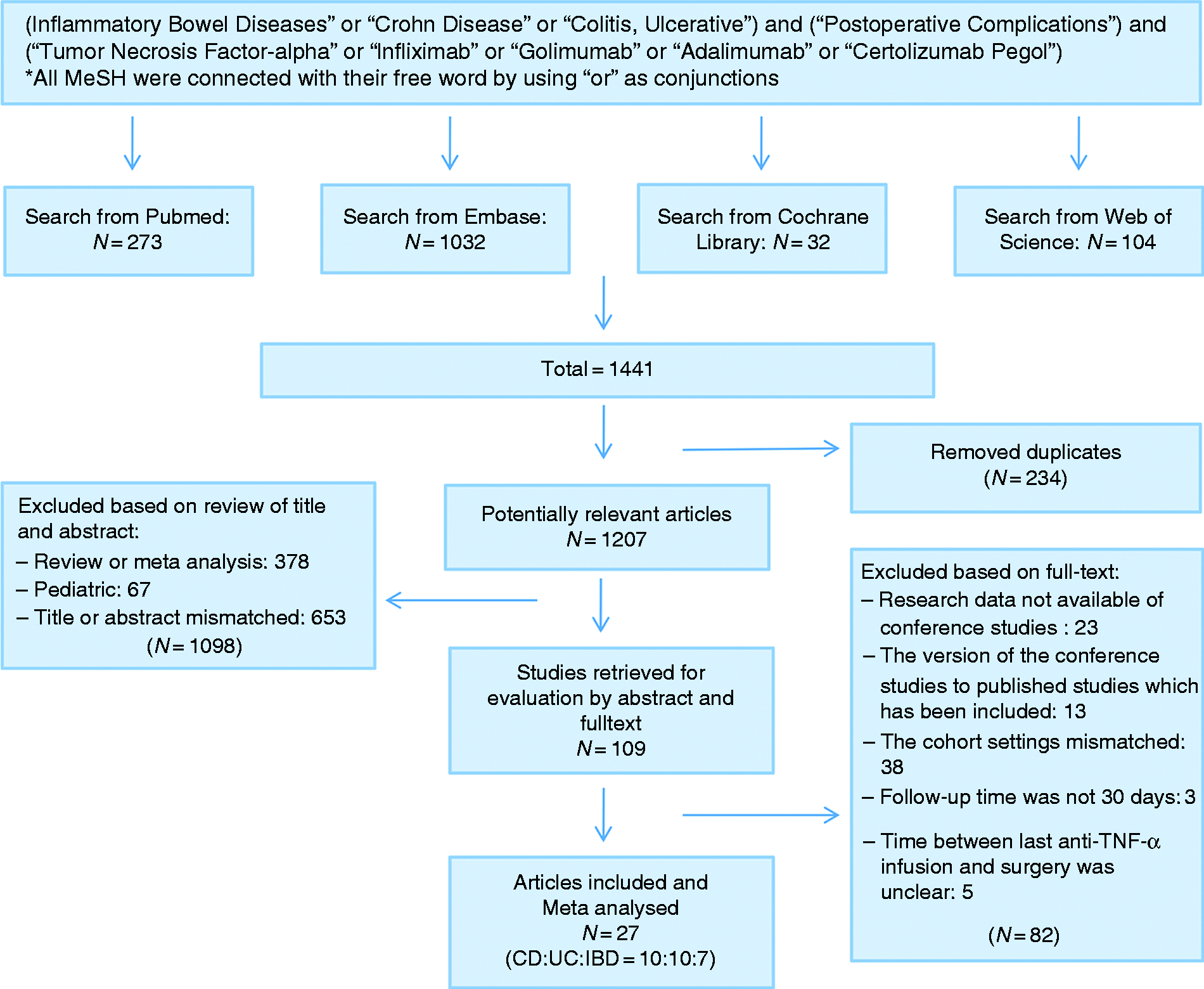
Summary of all forest plots.
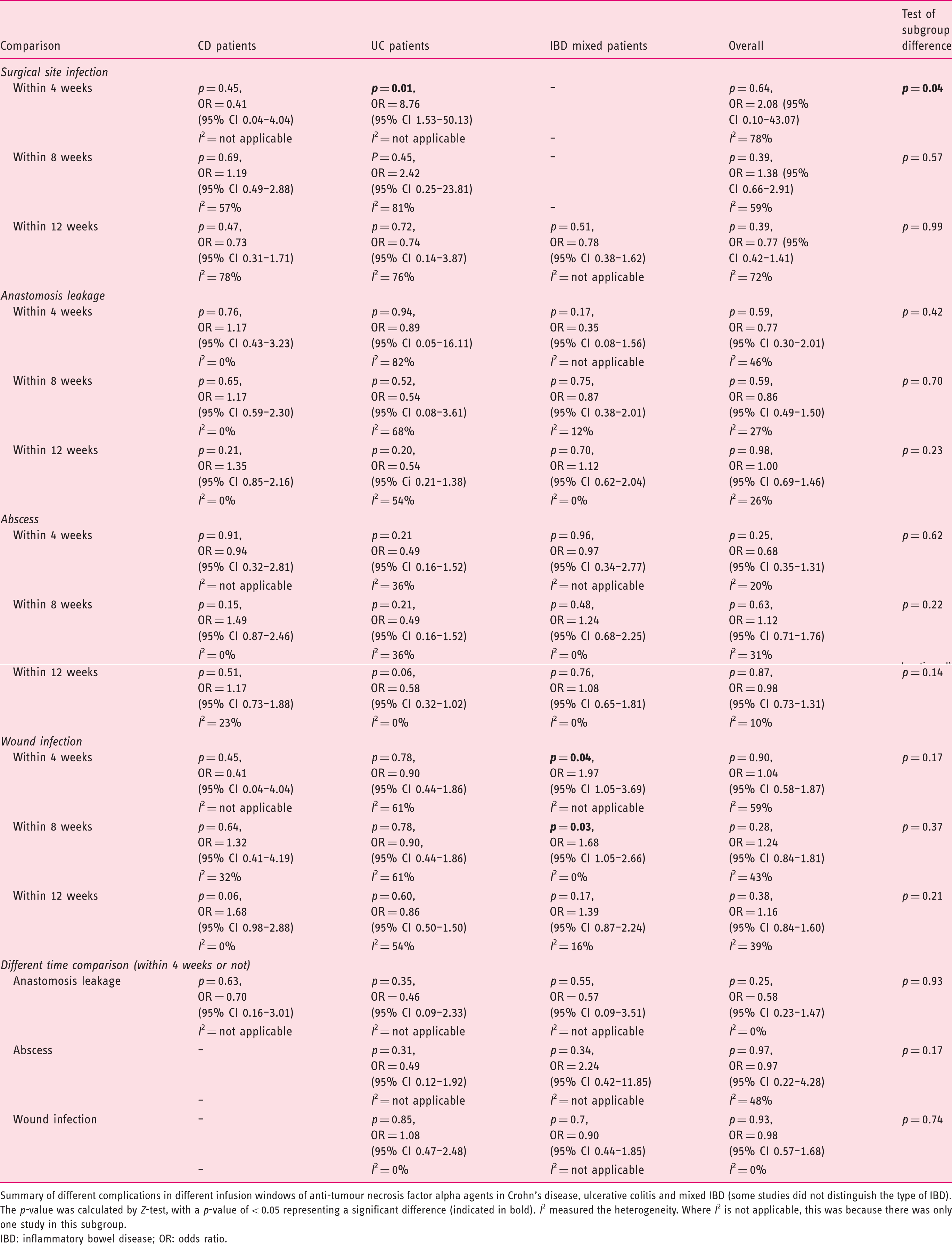
Summary of different complications in different infusion windows of anti-tumour necrosis factor alpha agents in Crohn’s disease, ulcerative colitis and mixed IBD (some studies did not distinguish the type of IBD). The p-value was calculated by Z-test, with a p-value of < 0.05 representing a significant difference (indicated in bold). I2 measured the heterogeneity. Where I2 is not applicable, this was because there was only one study in this subgroup.
IBD: inflammatory bowel disease; OR: odds ratio.
Comparison I
SSI
Within 4 weeks
Among studies with a preoperative anti-TNF-α window of within four weeks,
35
no significant difference was observed SSI between anti-TNF-α and control cohorts (p = 0.64; OR = 2.08; 95% CI 0.10–43.07, I2 = 78%). Results were similar in the CD subgroup. However, results of a single study showed that anti-TNF-α increased the risk of postoperative SSI in the UC subgroup (p = 0.01; OR = 8.76; 95% CI 1.53–50.13, I2 = not applicable; Figure 2(a)).
Surgical site infection in anti-tumour necrosis factor alpha agents (anti-TNF-α) and control. (a) Forest plot for preoperative anti-TNF-α window of within four weeks. (b) Forest plot for preoperative anti-TNF-α window of within eight weeks. (c) Forest plot for preoperative anti-TNF-α window of within 12 weeks.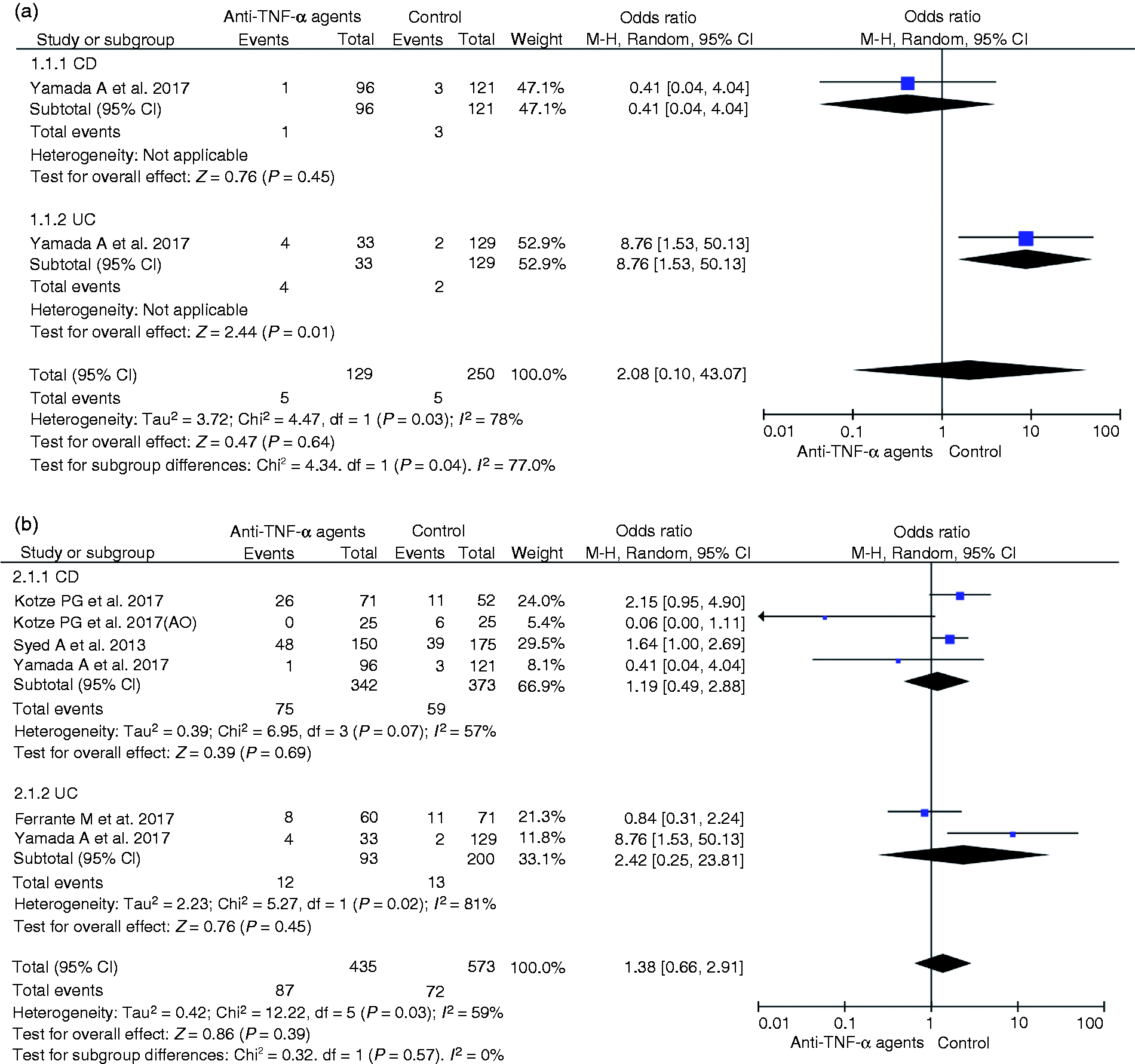
Within 8 weeks
Among studies with a preoperative anti-TNF-α window within eight weeks,24,33,35–37 there was no significant difference in SSI between anti-TNF-α and control cohorts (p = 0.39; OR = 1.38; 95% CI 0.66–2.91, I2 = 59%; Figure 2(b)).
Within 12 weeks
Among studies with a preoperative anti-TNF-α window within 12 weeks,15,24–26,33–38 the data revealed no significant difference in SSI between anti-TNF-α and control cohorts (p = 0.39; OR = 0.77; 95% CI 0.42–1.41, I2 = 72%; Figure 2(c)).
Anastomotic leakage
Within 4 weeks
Among studies with a preoperative anti-TNF-α window within four weeks,23,27,32,35 no significant difference in anastomotic leakage was observed between anti-TNF-α and control cohorts (p = 0.59; OR = 0.77; 95% CI 0.30–2.01, I2 = 46%; Figure 3(a)).
Anastomotic leakage in anti-TNF-α and control. (a) Forest plot for preoperative anti-TNF-α window of within four weeks. (b) Forest plot for preoperative anti-TNF-α window of within eight weeks. (c) Forest plot for preoperative anti-TNF-α window of within 12 weeks.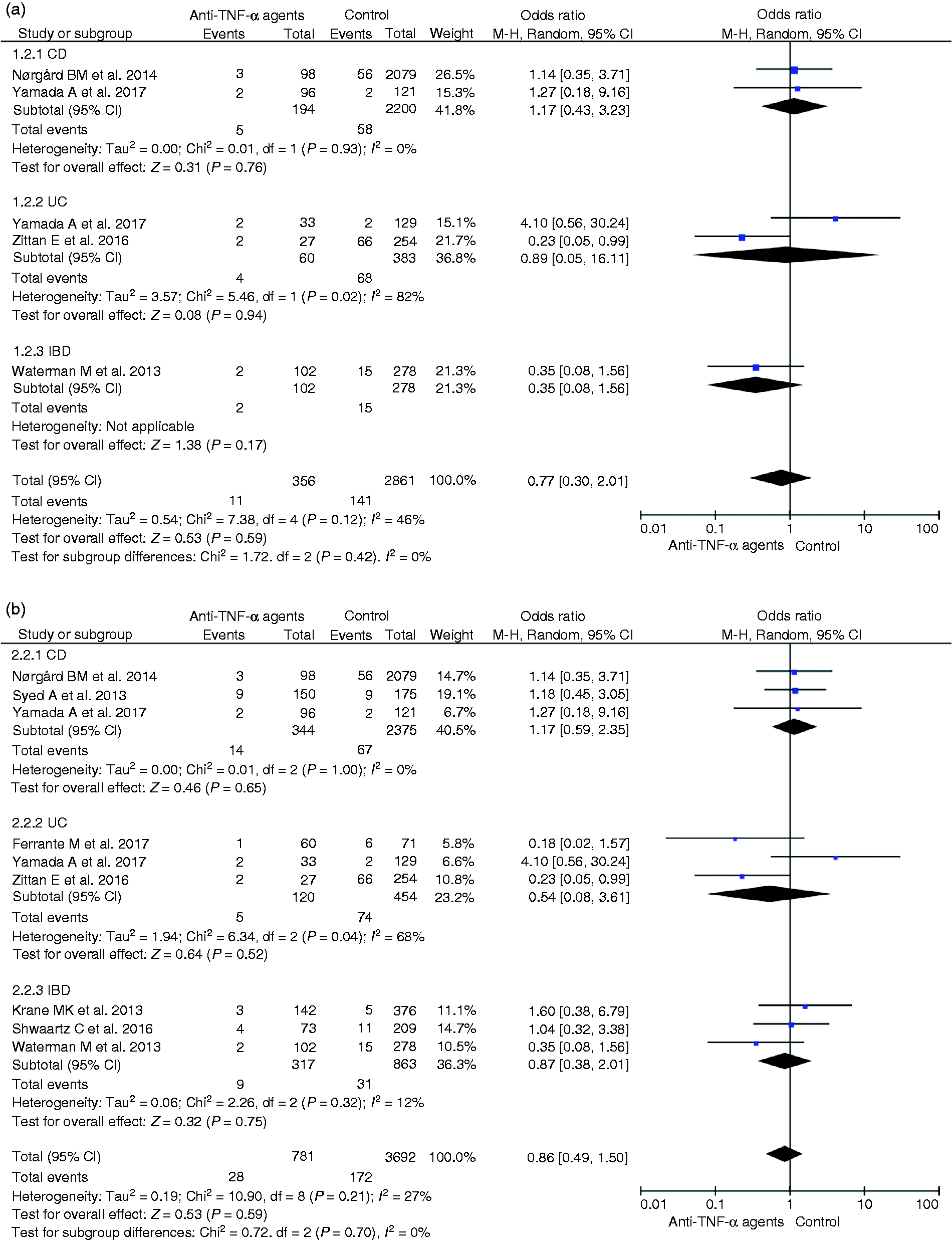
Within 8 weeks
Among studies with a preoperative anti-TNF-α window within eight weeks,22–24,27,30,32,35,36 there was no significant difference in anastomotic leakage between anti-TNF-α and control cohorts (p = 0.59; OR = 0.86; 95% CI 0.49–1.50, I2 = 27%; Figure 3(b)).
Within 12 weeks
Among studies with a preoperative anti-TNF-α window within 12 weeks,13–19,21–24,27,30,32,34–36,38 the data revealed no significant difference in anastomotic leakage between anti-TNF-α and control cohorts (p = 0.98; OR = 1.00; 95% CI 0.69–1.46, I2 = 26%; Figure 3(c)).
Abscess formation
Within 4 weeks
Among studies with a preoperative anti-TNF-α window within four weeks,27,29,32,35 no significant difference in abscess formation was observed between anti-TNF-α and control cohorts (p = 0.25; OR = 0.68; 95% CI 0.35–1.31, I2 = 20%; Figure 4(a)).
Abscess formation in anti-TNF-α and control. (a) Forest plot for preoperative anti-TNF-α window of within four weeks. (b) Forest plot for preoperative anti-TNF-α window of within eight weeks. (c) Forest plot for preoperative anti-TNF-α window of within 12 weeks.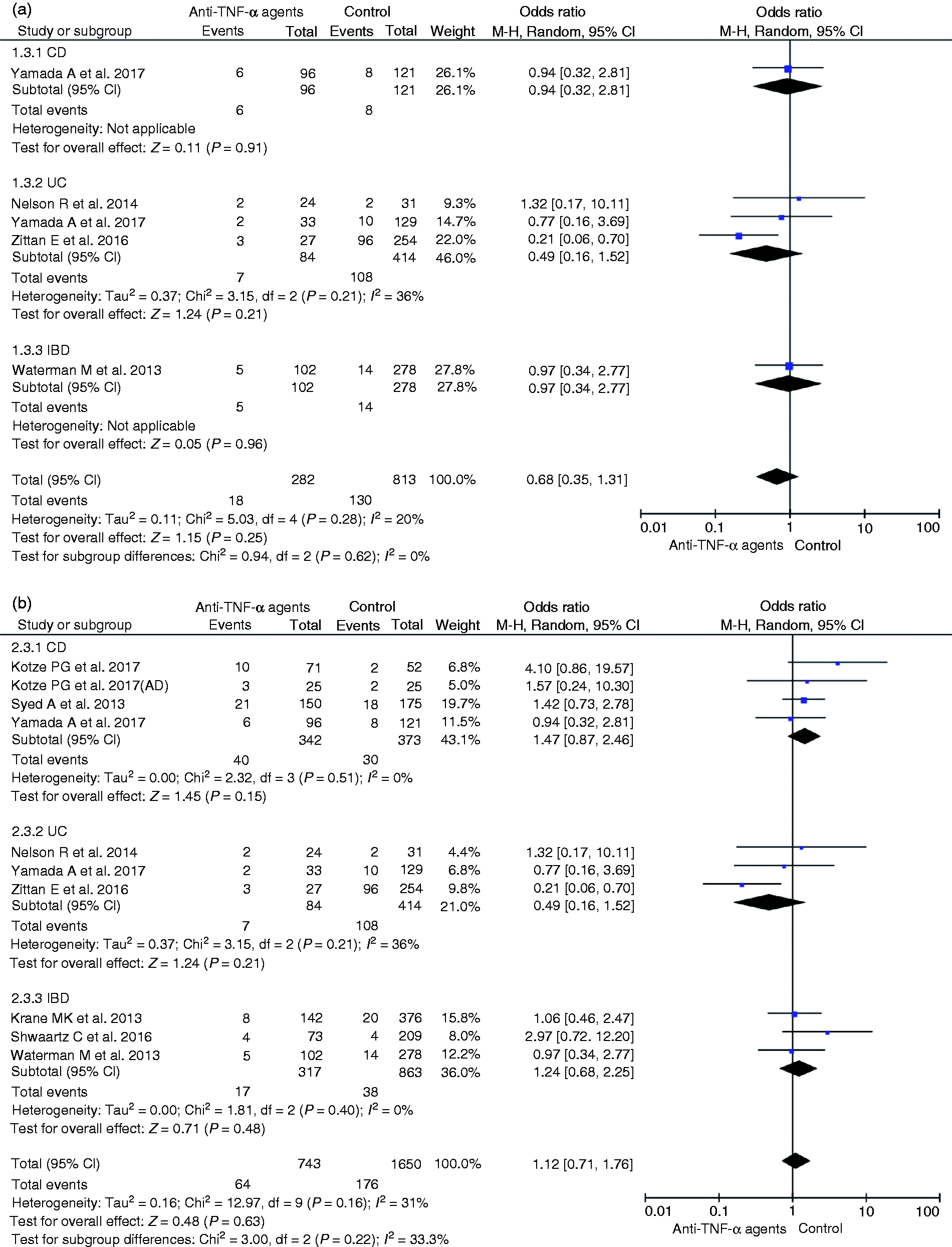
Within 8 weeks
Among studies with a preoperative anti-TNF-α window within eight weeks,22,24,27,29,30,32,33,35,37 there was no significant difference in abscess formation between anti-TNF-α and control cohorts (p = 0.63; OR = 1.12; 95% CI 0.71–1.76, I2 = 31%; Figure 4(b)).
Within 12 weeks
Among studies with a preoperative anti-TNF-α window within 12 weeks,14–16,18–27,29,30,32–35,37,38 the data revealed no significant difference in abscess formation between anti-TNF-α and control cohorts (p = 0.87; OR = 0.98; 95% CI 0.73–1.31, I2 = 10%; Figure 4(c)).
Wound infection
Within 4 weeks
Among studies with a preoperative anti-TNF-α window within four weeks,27,29,32,35,39 no significant difference in wound infection was observed between anti-TNF-α and control cohorts (p = 0.90; OR = 1.04; 95% CI 0.58–1.87, I2 = 59%). Results were similar in CD and UC subgroups. However, results of a single study showed that anti-TNF-α increased the risk of postoperative wound infection in the mixed IBD subgroup (p = 0.04; OR = 1.97; 95% CI 1.05–3.69, I2 = not applicable; Figure 5(a)).
Wound infection in anti-TNF-α and control. (a) Forest plot for preoperative anti-TNF-α window of within four weeks. (b) Forest plot for preoperative anti-TNF-α window of within eight weeks. (c) Forest plot for preoperative anti-TNF-α window of within 12 weeks.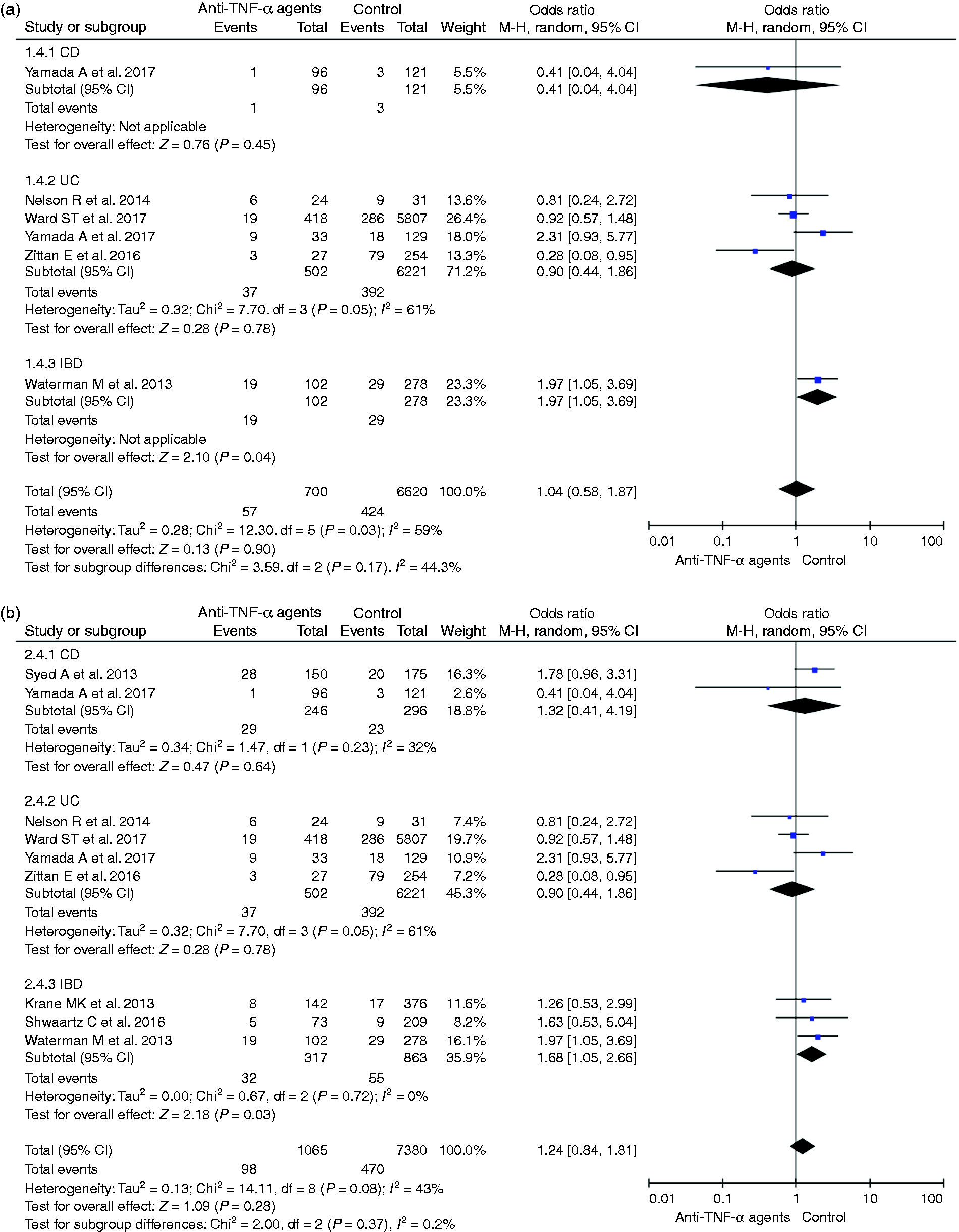
Within 8 weeks
Among studies with a preoperative anti-TNF-α window within eight weeks,22,24,27,29,30,32,35,39 there was no significant difference in wound infection between anti-TNF-α and control cohorts (p = 0.28; OR = 1.24; 95% CI 0.84–1.81, I2 = 43%). Results were similar in CD and UC subgroups. However, anti-TNF-α increased the risk of postoperative wound infection in the mixed IBD subgroup (p = 0.03; OR = 1.68; 95% CI 1.05–2.66, I2 = 0%). The results were provided in three studies (Figure 5(b)).
Within 12 weeks
Among studies with a preoperative anti-TNF-α window within 12 weeks,15,16,20–22,24,27,29,30,32,34,35,38,39 the data revealed no significant difference in wound infection between anti-TNF-α and control cohorts (p = 0.38; OR = 1.16; 95% CI 0.84–1.60, I2 = 39%; Figure 5(c)).
Comparison II
Different preoperative anti-TNF-α windows (within four weeks vs. more than four weeks)
Anastomotic leakage
Among studies involving cohorts with different preoperative anti-TNF-α windows (within four weeks vs. more than four weeks),23,27,32 no significant difference in anastomotic leakage was observed between the two cohorts (p = 0.25; OR = 0.58; 95% CI 0.23–1.47, I2 = 0%; Figure 6(a)).
Different preoperative anti-TNF-α windows within four weeks versus more than four weeks. (a) Forest plot for anastomotic leakage. (b) Forest plot for abscess formation. (c) Forest plot for wound infection.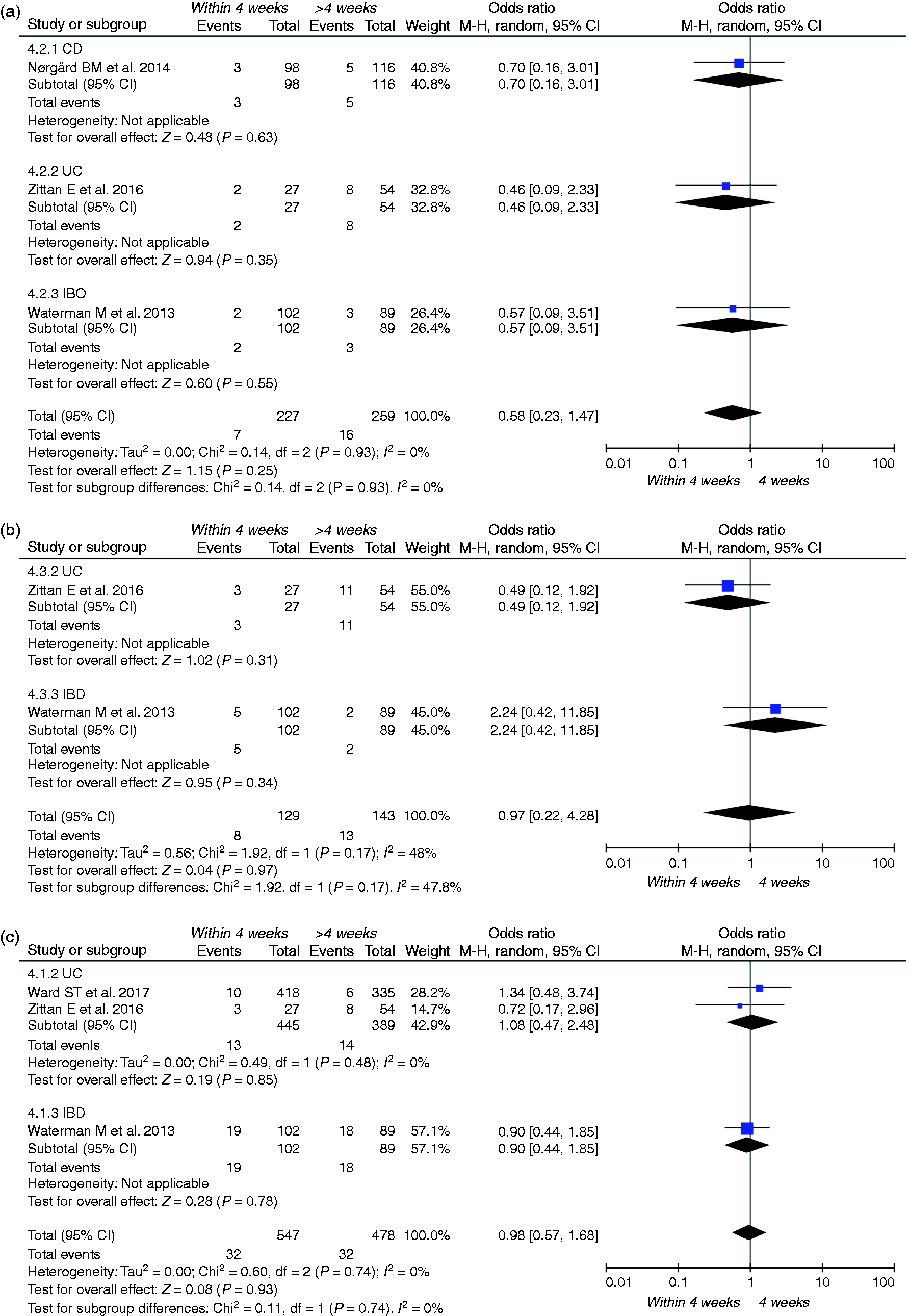
Abscess formation
Among studies with a preoperative anti-TNF-α window within four weeks or more than four weeks,27,32 there was no significant difference in abscess formation between the two cohorts (p = 0.97; OR = 0.97; 95% CI 0.22–4.28, I2 = 48%; Figure 6(b)).
Wound infection
Among studies with a preoperative anti-TNF-α window within four weeks or more than four weeks,27,32,39 the data revealed no significant difference in wound infection between the two cohorts (p = 0.93; OR = 0.98; 95% CI 0.57–1.68, I2 = 0%; Figure 6(b)).
Supplementary Comparison II
Different preoperative anti-TNF-α windows (within two weeks vs. more than two weeks)
The results revealed no significant difference in anastomosis leakage between the two cohorts (p = 0.96; OR = 0.97; 95% CI 0.30–3.12, I2 = 0%; Supplemental Figure S3).23,27,32
Different preoperative anti-TNF-α windows (within eight weeks vs. more than eight weeks)
The results revealed no significant difference in anastomosis leakage between the two cohorts (p = 0.82; OR = 0.91; 95% CI 0.39–2.12, I2 = 0%; Supplemental Figure S4).28,36
Sensitivity analyses and funnel plot
After excluding one report to reduce heterogeneity, the results for wound infection within four weeks and SSI within eight weeks remained similar to those before exclusion of the paper. In addition, heterogeneity of SSI within 12 weeks could not be reduced by excluding a single article. Details are shown in Supplementary Table S2. None of the funnel plots showed significant publication bias. Details are shown in Supplemental Figure S5.
Discussion
In this review and meta-analysis, no significant difference was found in postoperative SSI between anti-TNF-α and control cohorts, regardless of whether the preoperative anti-TNF-α window was set within 4, 8 or 12 weeks for IBD patients. Results were similar for all types of SSI, including anastomotic leakage, abscess formation and wound infection. Additionally, no significant difference in postoperative complications was observed between cohorts of patients with a preoperative anti-TNF-α window of within four weeks versus more than four weeks. These results remained the same when the cut-off was changed from four weeks to two or eight weeks. However, when CD, UC and mixed IBD subgroups were separately examined, anti-TNF-α increased the risk of postoperative SSI in the UC subgroup within four weeks. Anti-TNF-α also increased wound infection in the mixed IBD subgroup within four or eight weeks.
According to its pharmacokinetics, the reported half-life of anti-TNF-α is about 7–14 days. 11 Thus, clearance time is 35–60 days if based on five half-lives. However, it is more accurate to detect whether preoperative serum anti-TNF-α levels are higher than the trough level (0.98 mg/mL),4,32 as there are individual differences. High levels of infliximab antibody (>3 IU/mL) reduced the time to reach the trough of infliximab, which was unrelated to CD or UC.40,41 Therefore, in the present study, three common time frames were examined (4, 8 and 12 weeks) according to the original studies, during which serum levels of anti-TNF-α before operation can be reflected to some extent. Interestingly, Lau et al. reported that half of the patients treated with anti-TNF-α did not have detectable levels in preoperative serum. 4 Among these individuals, anti-TNF-α was more undetectable in the UC subgroup compared with the CD subgroup. The original author explained that UC patients may produce more anti-TNF-α antibodies as a result of a larger inflammation area than CD patients. 4 Although this explanation is controversial, it is possible that under the existing grouping criteria, even when the time frame was within four weeks, there may have been a subset of patients who did not have sufficient anti-TNF-α serum levels to make an impact during and after surgery.
As UC and CD have distinct characteristics, they should be discussed separately. For example, UC patients often use ileal pouch–anal anastomosis, while patients with CD mainly undergo segmental bowel resection to resolve the obstruction (Supplemental Table S1). However, in clinical practice, studies often grouped UC and CD as IBD without distinguishing them. Thus, we set up the mixed IBD subgroup. Although the p-value was < 0.05 when analysing SSI of the UC subgroup or wound infection of the mixed IBD subgroup administered anti-TNF-α within four weeks, this is not a reason to be overly concerned and should not be interpreted as a risk factor because there was only one included study for each subgroup. At the same time, anti-TNF-α was a risk factor for wound infection in the mixed IBD subgroup treated within eight weeks. These results were supported by three studies.22,27,30 However, no evidence of increased postoperative complications was found in the same comparison between UC and CD subgroups or in the total results. Subgrouping did not differentiate disease species to result in a bias. Thus, as a subgroup, the result of mixed IBD subgroup should not be used as a component of the main conclusion. However, we should remain wary of the potential risk for increased risk of wound infection.
In addition to the preoperative anti-TNF-α window, the main points of contention were the type of surgery, concomitant medications and disease severity. First, Selvaggi et al. 7 considered that anti-TNF-α increased early pouch-specific complications and complications after ileostomy closure. Second, most concomitant medications were corticosteroids and immunomodulatory agents. Ferrante et al. 15 suggested that corticosteroids, rather than anti-TNF-α, increased postoperative complications. Third, the severity of UC disease affects haemoglobin levels, which may affect the occurrence of postoperative complications. These factors interfere with the analysis of the effects of anti-TNF-α. Most studies statistically analysed the above three points using multivariate regression analysis. However, the above data were undivided and non-extractable in the original study, and we were unable to conduct separate subgroup analyses based on these points of contention. Although most studies used statistical analyses to prove that there was little significant difference in each point between anti-TNF-α and control groups, the influence was still significant for the results.
Our study has some limitations. First, most of the included studies were retrospective studies rather than randomised controlled trials. Second, the grouping criteria of SSI differed among the studies. Third, non-infectious complications and non-SSI were extracted but not analysed. However, this is the first systematic review and meta-analysis of the preoperative anti-TNF-α time window, and it has some strengths. We focused on all types of IBD studies, including mixed IBD, as well as a variety of anti-TNF-α agents. Moreover, we discussed the two factors of anti-TNF-α metabolism and disease types in more detail.
Our results have some clinical implications. The results suggest that the time interval between anti-TNF-α administration and surgery should not be a determinant of the timing of surgery. Moreover, if necessary, anti-TNF-α could continue to be used until the procedure is performed without fear of increased complications. This will allow surgeons to use anti-TNF-α safely for preoperative disease control in patients with IBD. It is hoped that more studies will focus on preoperative anti-TNF-α serum levels in patients to provide stronger evidence.
In conclusion, current evidence suggests that with respect to SSI and its subtypes, anti-TNF-α may be safe for UC and CD patients who received their last infusion of anti-TNF-α more than four weeks before surgery. We also found no evidence that anti-TNF-α was a risk factor when administered within four weeks after excluding subgroup results of only one study. Stratified by time window, use of anti-TNF-α until surgery has the potential to become a more considered strategy in clinical practice.
Supplemental Material
UEG878998 Supplemental Material - Supplemental material for Effects of preoperative anti-tumour necrosis factor alpha infusion timing on postoperative surgical site infection in inflammatory bowel disease: A systematic review and meta-analysis
Supplemental material, UEG878998 Supplemental Material for Effects of preoperative anti-tumour necrosis factor alpha infusion timing on postoperative surgical site infection in inflammatory bowel disease: A systematic review and meta-analysis by YuJie Qiu, ZiCheng Zheng, Gang Liu, XinYu Zhao and AnQi He in United European Gastroenterology Journal
Footnotes
Acknowledgements
Declaration of conflicting interests
The authors have no financial or other conflicts of interest to disclose.
Funding
No specific funding has been received for this work.
Ethics approval
Because of the public nature of all the data, the study did not require ethics approval.
Informed consent
No informed consent is required because the study did not involve individuals identifying information or interacting with individual humans.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.