
Abstract
Introduction
Device-assisted enteroscopy is a new endoscopic technique for the evaluation of small bowel in adults and children. Data in pediatric population are limited. This review aims to identify diagnostic and therapeutic benefits of enteroscopy in children.
Methods
We have analysed paediatric literature on device-assisted enteroscopy focusing on indications, technical aspects and complications, with attention given to adult publications that may be applicable to the paediatric population.
Results
Obscure gastrointestinal bleeding, Crohn’s disease and small bowel polyps are the main indications of enteroscopy in children. Device-assisted enteroscopy has high diagnostic yield for the main paediatric indications, but MR-enterography and capsule endoscopy should be used beforehand in diagnostic work-up to better identify candidates for enteroscopy and to improve its diagnostic and therapeutic yield. Major complications are rare and mostly related to therapeutic procedures.
Conclusion
Despite limited data in the paediatric population, device-assisted enteroscopy represents a useful and safe endoscopic technique in children. Its use, combined with MR-enterography and capsule endoscopy, allows identification and treatment of many of the small bowel paediatric diseases with a low risk of complications.
Introduction
Evaluation of small intestinal mucosa is an important aspect in the treatment of children with gastrointestinal disorders.1,2 So far, small bowel (SB) contrast studies have represented the most effective diagnostic procedure because of the length, location and tortuosity of the small intestine. 2 Push and surgically assisted enteroscopy were used to further diagnose or treat SB lesions. However, the lack of efficacy and the invasive nature of these procedures indicated a need for new methods. 2
In 2001, the introduction of capsule endoscopy (CE) allowed high-quality full colour views of the mucosa for the first time. Major limitations of CE are the inability to take biopsies and perform therapeutic procedures and the absence of controlled movement of the capsule. 3 Another limitation is that general anaesthesia is needed in young children to place the capsule in the duodenum. 3 The contraindications due to potential capsule retention are motility disorders, suspicion of gastrointestinal obstruction or fistulas.2,3
Device-assisted enteroscopy (DAE) is a new endoscopic method, combining excellent visualization of SB, biopsy sampling and therapeutic procedures. 4 The diagnostic and therapeutic benefits of DAE in adults are well documented. Data on DAE in children are limited to case reports and the few prospective studies. 5
This article will review paediatric literature on DAE focusing on the indications, technical aspects, complications and risks, with attention given to adult publications that may be applicable to the paediatric population.
Technical considerations
Equipment
In 2001, the double-balloon enteroscopy (DBE) system was presented for the first time in Japan, 6 and the first paediatric reports of balloon-assisted enteroscopy (BAE) stem from 2003.7,8 Currently, the available DAE systems are DBE, single-balloon enteroscopy (SBE) and spiral enteroscopy. However, no data reporting the use of spiral enteroscopy in children have been published to date, and the 16-mm outer diameter of the overtube currently makes this technique impractical for most paediatric patients. 9
Double-balloon enteroscopy
Two type of endoscopes, EN-450P5 and EN-450T5 (Fujinon Inc, Saitama, Japan), are available, both of which have a working length of 200 cm. The EN450-P5 model has a working channel of 2.2 mm and an outer diameter of 8.5 mm. The EN450-T5 model has a working channel of 2.8 mm and an outer diameter of 9.4 mm. The soft flexible polyurethane overtube measures 12.2 and 13.2 mm, respectively, with an overall length of 145 cm. The latex balloons of the DBE system are located at the tip of the enteroscope and of the overtube. The balloons can be inflated and deflated using a pressure control pump.7,8
Single-balloon enteroscopy
SBE (Olympus Optical, Tokyo, Japan) has a working length of 200 cm, 9.2-mm outer diameter and a 2.8-mm working channel. The flexible overtube measures 140 cm in length and has a diameter of 13.2 mm with a silicon balloon at the distal end. 10
Technique and procedure
In the paediatric population, the DBE and SBE have the same procedural technique as that used for adults.10,11 However, there are special considerations specific to age and patient size. BAE is suitable and safe for paediatric patients aged >3 years or body weight >14 kg.7,12,13 Because of a smaller abdominal cavity, thinner intestinal walls and a narrower intestinal lumen, BAE in younger children is more technically difficult and requires a greater level of skill. 7
The air pressure controlled pump system determines the balloon size with a maximum inflatable pressure of 45 mmHg. This pressure does not increase the risk of discomfort or perforation. After being inflated the balloon facilitates anchoring and shortening of the intestine when retracted. This leads to straightening of the bowel allowing further advancement of the enteroscope and prevents looping. 14 Repeated advancement and retraction, push-and-pull technique, facilitates pleating of the SB over the enteroscope, allowing for deep enteroscopy. 15 BAE is often performed by two physicians, one manoeuvring the dials of the enteroscope, the other assisting in the passage and reduction of the overtube.
The approach (oral, anal or both) is determined on clinical judgement. Several techniques, including CE and MR-enterography (MRE), may be used to assist in localizing the lesion. The complete view of SB, from duodenum to caecum, is often difficult, so both oral and anal approaches are used if inspection of the whole intestine is needed. An India ink tattoo is left at the deepest point of insertion achieved during the first enteroscopy. In many cases complete SB assessment is not necessary (e.g. primary lesion is encountered, obviating the need for complete examination) or unachievable, and the reported success rate is 16–86%.16,17 Usually, the oral approach is the first choice due to the lower technical difficulty. Indeed, published series for BAE in adults and children have noted technical challenges to consistent passage through and beyond the ileocaecal valve.
The procedure time varies from 40 up to 200 minutes in case of a therapeutic procedure.7,8,13,18 A recently randomized multicentre trial compared the technical performance of DBE and SBE procedures and pointed out that there is no significant difference between the two systems regarding insertion depth and diagnostic yield. 19
For the oral approach, an overnight fasting of 12 hours for solid food and 4 hours for clear liquids before starting the procedure is adequate; for retrograde enteroscopy, a bowel cleansing is performed, as it is indicated for conventional colonoscopy. General anaesthesia is recommended for difficult and long investigations or for patient in whom moderate sedation is not appropriate.7,20 Fluoroscopy can help with identifying enteroscope positioning and confirming absence of a loop that might explain limited scope advancement. Yet, once an endoscopist’s experience develops, fluoroscopy is less often needed, except in selected cases when adhesions are expected or in massive SB Crohn’s disease involvement. Radiology is also useful to assess stricture complexity and to guide balloon dilation. 21 Currently, there are not specific and well-established learning programmes for enteroscopy, especially for paediatric endoscopists. 15 Enteroscopy training may be incorporated into the standard endoscopic training. Recently, a minimum of 10 trans-oral procedures and at least 5 retrograde examinations for a single operator to maximize competence has been suggested.22,23
Indications
List of the available studies containing data on the number of cases, indications, main findings and complications.
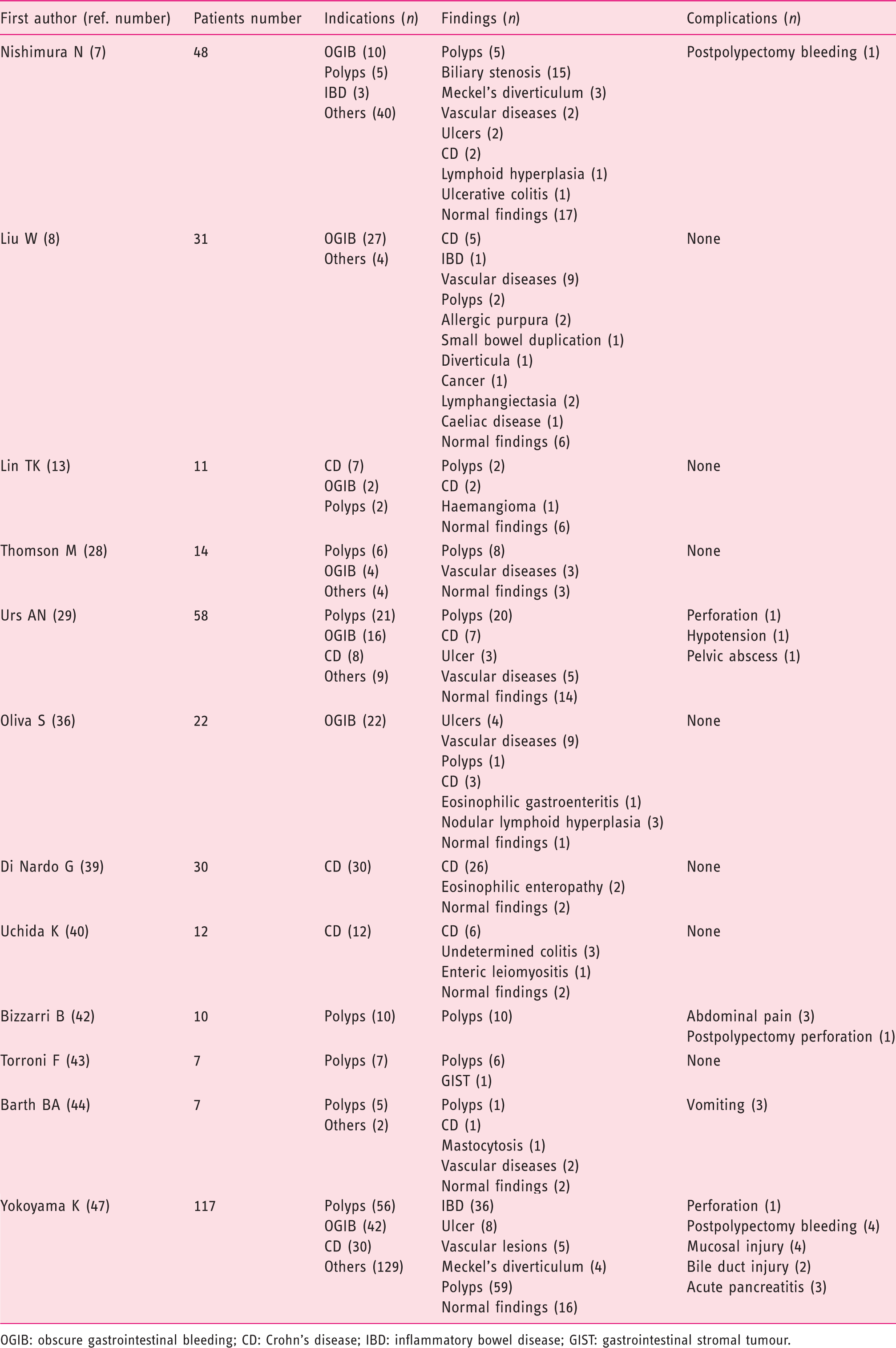
OGIB: obscure gastrointestinal bleeding; CD: Crohn’s disease; IBD: inflammatory bowel disease; GIST: gastrointestinal stromal tumour.
Obscure gastrointestinal bleeding (OGIB)
OGIB is the most common indication for BAE in children. Recent paediatric reports have shown diagnostic yields of between 50% and 81% and therapeutic yields of between 40% and 64%.7,8,28,29 Small bowel polyps, ulcer, angiodysplasias, Crohn’s disease and Meckel’s diverticulum are the prevalent causes of bleeding (Figure 1). Therapeutic interventions such as polypectomy, argon plasma coagulation and clip placement have been described. In a prospective study comparing CE and DBE in patients with OGIB, the diagnostic rate was 80% for CE and 60% for DBE; however, 51% of the patients had therapeutic intervention using argon plasma, pointing out a clear advantage for BAE.
30
Enteroscopic findings of the main small bowel diseases. Bleeding ulcer (a), pedunculated polyp (b) treated with polypectomy (c), angiodysplasia treated with clip placement (d and e).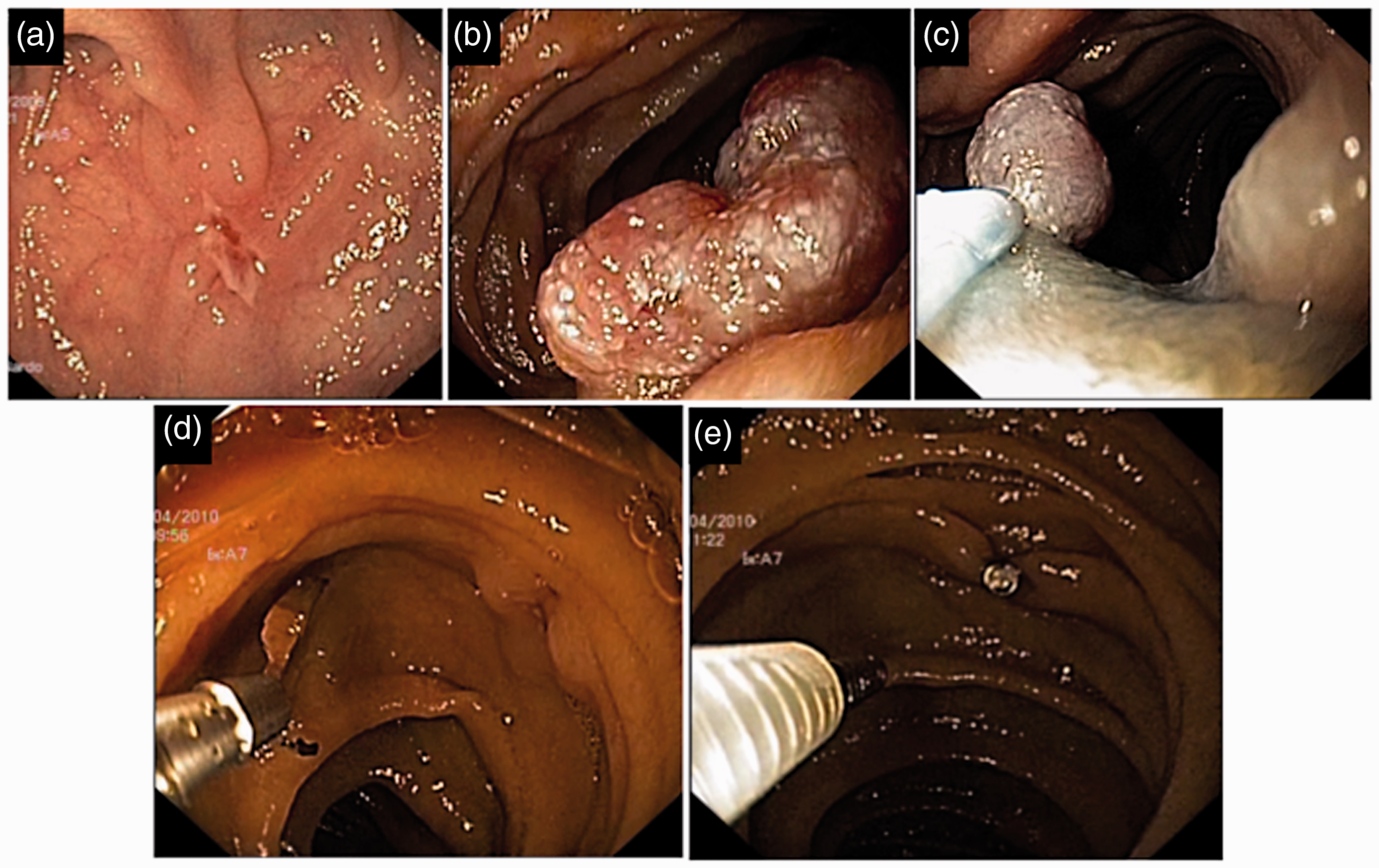
Three meta-analyses of adult patients confirmed a diagnostic yield of BAE of approximately 60% in OGIB31-33 comparable to that reported for CE. In practice guidelines endorsed by international gastroenterology associations, MRE or CE are recommended before BAE to increase diagnostic yield, to direct route of insertion and to optimize therapeutic options.24,27,34,35
In our recent prospective paediatric study CE has been systematically performed (including second look with Colon-CE) before enteroscopy, and this combined approach significantly increased the overall diagnostic yield (86%). 36 However, CE is an expensive procedure and retention of capsule can be a possible complication; 3 thus, we have recently demonstrated that MRE is an accurate imaging modality in the evaluation of paediatric OGIB, with a diagnostic power comparable to CE. 37 In this article we have highlighted the key role of MRE to identify intestinal disorders requiring a surgical first line approach avoiding expensive and potentially dangerous techniques such as CE and BAE.
In conclusion, BAE has a high diagnostic yield in diagnosing the cause of OGIB in children with the advantage of histologic diagnosis and therapeutic intervention. Nevertheless, future prospective studies are needed to establish the correct role of enteroscopy in the diagnostic algorithm of children with OGIB. Based on current literature and our practical experience we propose an algorithm for the diagnosis of paediatric OGIB (Figure 2).
Proposed algorithm for children with obscure gastrointestinal bleeding. In children with negative upper endoscopy and colonoscopy, MR-enterography and/or Meckel scan are recommended. If imaging is positive, detected lesions should be treated with enteroscopy or surgery, while in presence of unspecific or negative imaging findings, CE should be done. If CE is positive, specific management should be carried out. If CE is negative, the patient should have a clinical follow-up and in case of recurrence, CE-second look or BAE should be considered. GI: gastrointestinal; CE: capsule endoscopy; BAE: balloon-assisted enteroscopy.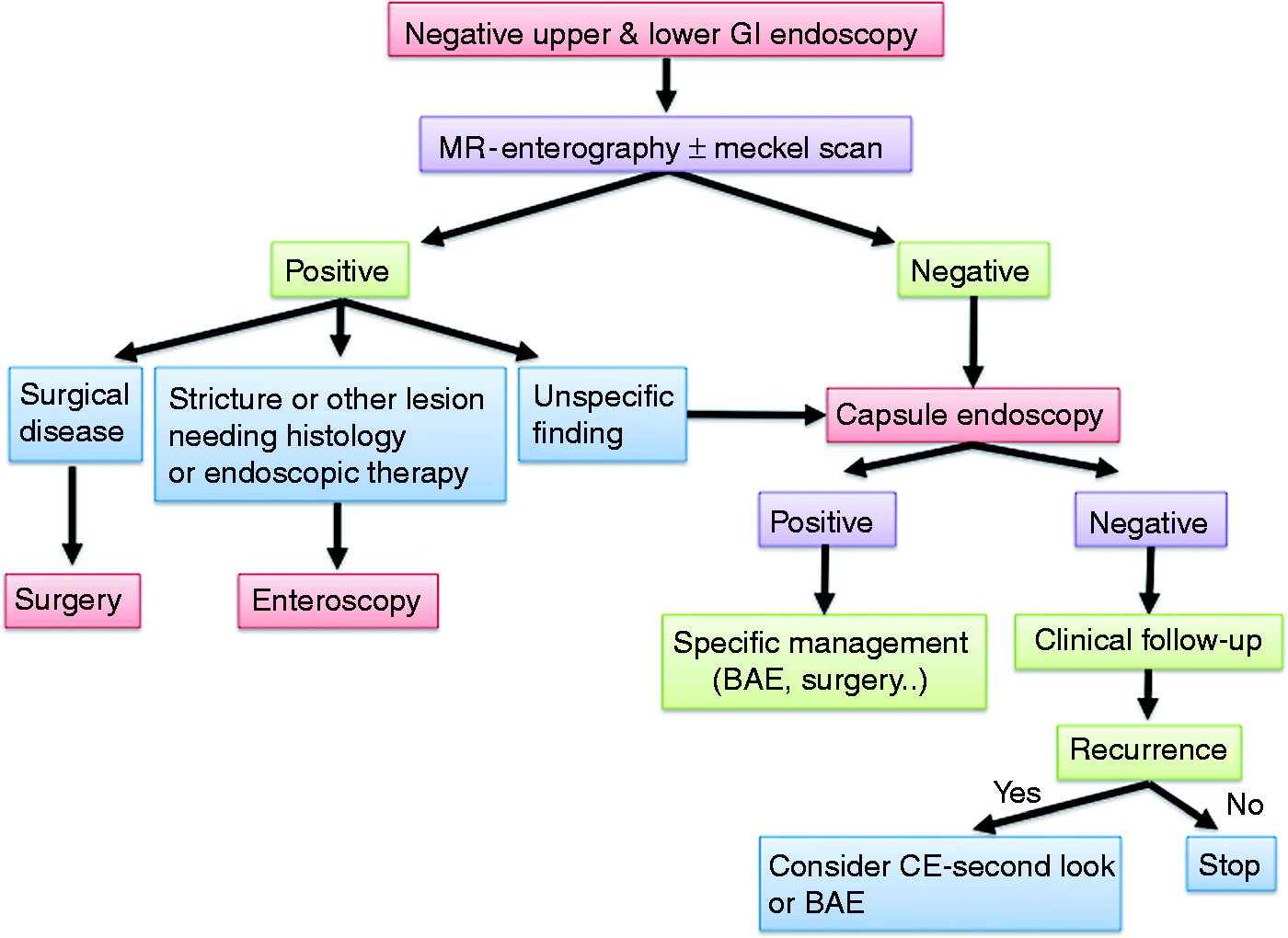
Crohn’s disease
In adults, the role of BAE in the management of patients with Crohn’s disease (CD) has been described in the endoscopy guidelines of the ECCO.24,38
Four studies, two of SBE and two of DBE,18,29,39,40 evaluated the impact of BAE in children with suspected and established CD. In our study, 16 paediatric patients with suspected CD and nonspecific findings at upper and lower gastrointestinal endoscopy were evaluated by SBE. 39 This provided histological diagnosis of CD in 12 patients and eosinophilic enteropathy in 2 patients, whereas no lesions were found in 2 patients. In 14 patients with longstanding CD, previous surgery and clinical symptoms unexplained by conventional endoscopy SBE findings led to the introduction of or to a change in biological therapy. SBE allowed successful dilation of small bowel strictures identified on MRE in five patients with CD. No complications occurred in all cases.
De Ridder et al. evaluated the diagnostic yield of SBE for paediatric CD by comparing it with ultrasonography and MRE. 18 Of 14 patients with suspected CD, 8 had a diagnosis confirmed after SBE. In five out of six patients with established CD, SBE findings led to a change in therapy. In the case series by Ridder, patients were evaluated directly by two-route SBE, not preceded by conventional upper and lower endoscopy or CE.
In the paper from Urs et al. 8 patients underwent 14 DBE procedures for suspected or established CD. 29 All of the patients had undergone CE, indicating changes in mucosa before DBE. In the suspected group, an accurate diagnosis of CD was obtained on DBE findings. In the established group, DBE led to a change or adjustment of treatment in all patients.
The study from Uchida et al. evaluated the efficacy and safety of DBE in 12 children with suspected or established CD.
40
In the suspected CD group (in which the diagnosis of CD was not possible on clinical and laboratory data, upper GI endoscopy, colonoscopy and SB-contrast study) DBE confirmed the diagnosis of CD in two patients out of eight, and led to a diagnosis in seven patients. In the established CD group DBE led to a change in the treatment in three patients out of four. We have published a diagnostic algorithm in paediatric patients with suspected and established CD.
41
Briefly, BAE is recommended when conventional studies including oesophagogastroduodenoscopy, ileocolonoscopy and imaging of SB and CE have not been determined and histological diagnosis and/or therapeutic procedure would alter disease management (Figure 3). In the setting of established CD, BAE is indicated when endoscopic visualization and biopsies of the small intestine beyond the reach of oesophagogastroduodenoscopy or ileocolonoscopy is necessary to exclude an alternative diagnosis (lymphoma, tuberculosis or carcinoma) or undertake a therapeutic procedure including dilation of a SB stricture, removal of retained capsule and treatment of bleeding lesions.
Proposed algorithm for children with suspected Crohn’s disease. BAE is recommended when conventional studies, including oesophagogastroduodenoscopy, ileocolonoscopy and imaging of SB and CE, have not been determined and histological diagnosis and/or therapeutic procedure would alter disease management (adapted from Di Nardo et al.
41
). GI: gastrointestinal; SB: small bowel; CE: capsule endoscopy; BAE: balloon-assisted enteroscopy.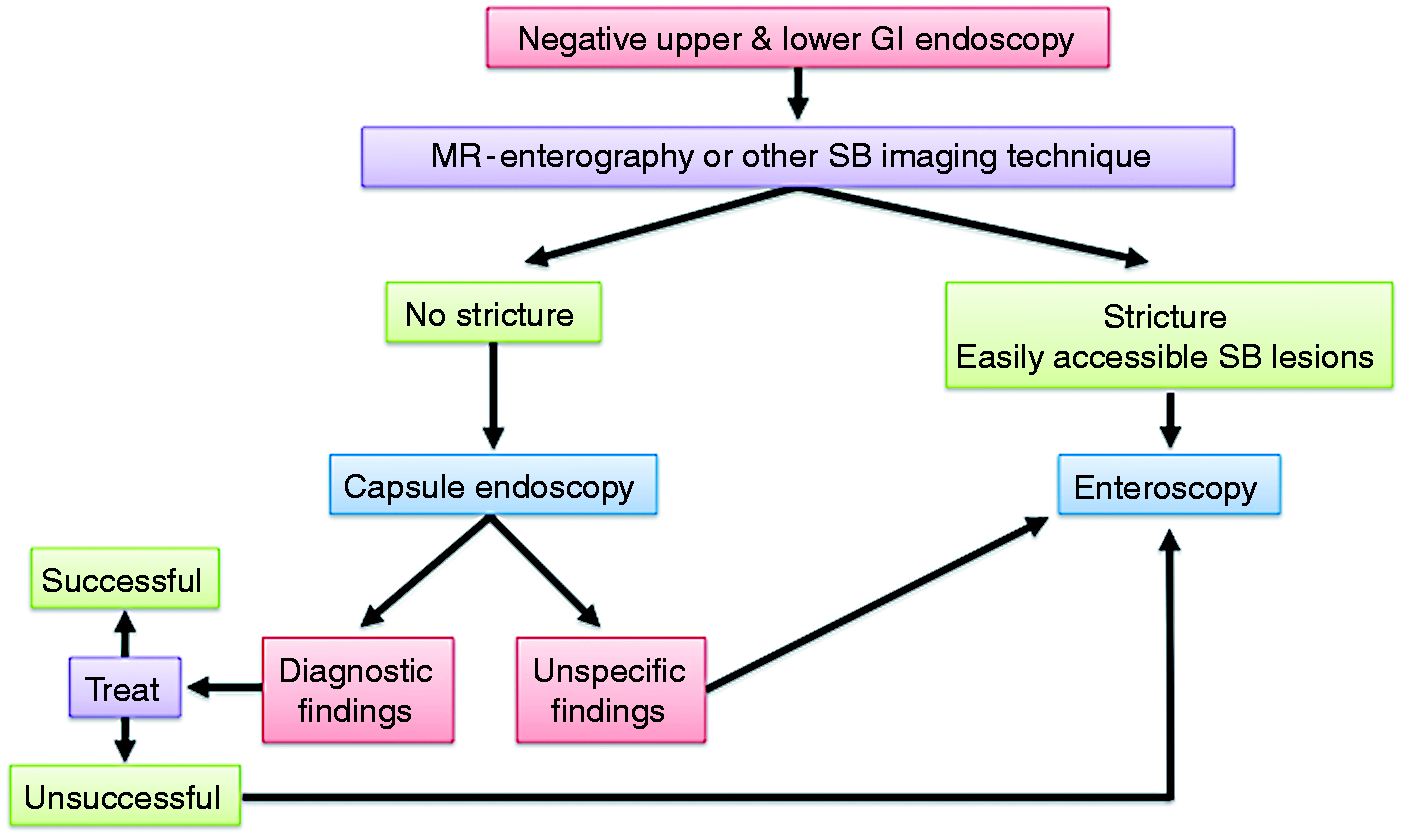
Polyps
Polyps in children with hereditary polyposis syndromes may cause bleeding, obstruction or intussusception and may finally progress into malignancy. These patients have a higher risk of undergoing emergency laparotomies with an increased rate of morbidity and mortality. Thus, well-time polypectomy may avoid the need for multiple surgical resections of affected intestine that may lead to short bowel syndrome.42-45
To date, eight case series, three SBE42-44 and five DBE,7,13,28,29 on paediatric patients have reported the performance of enteroscopy in the management of gastrointestinal polyps. In these case series, 53 patients underwent enteroscopy for surveillance and treatment; 101 procedures and 321 polypectomies were performed. A retrospective multicentre study evaluated the correlation between DBE and CE to investigate SB polyps and demonstrated that CE could be useful to define the number, location and size of the polyps and predict the difficulty of the polypectomy during enteroscopy. 45
Torroni et al. developed an algorithm for the management of patients with Peutz–Jeghers syndrome providing a screening from 8 years or earlier if symptomatic with endoscopy, colonoscopy and CE. They suggested elective polypectomy with SBE when significant small bowel polyps are detected (>15 mm) and laparotomy when polypectomy is not possible. Follow-up with CE, upper endoscopy and SBE, if necessary, is recommended every 2 years. 43 Although further studies are needed to assess the role and the timing of enteroscopy in the management of children with hereditary polyposis syndromes, enteroscopy is an effective and safe alternative to surgery for the treatment of isolated and non-complicated SB polyps.
Complications and safety
In adults, the rate of complications in diagnostic DBE is approximately 1% of cases. 46 The complications may be related to the procedure itself or may be secondary to anaesthesia, and the risk is higher in therapeutic enteroscopy (3–4%). The most commonly reported complications are pancreatitis, bleeding and perforations; the complications due to anaesthesia are less than 1% and they include pneumonia, respiratory depression and aspiration. The rate of mortality is 0.05%, even if the only data available are from the German double-balloon registry. 46
In paediatric published case series, major complications have been reported for therapeutic procedures, whereas there are no significant complications related to diagnostic procedures.
Liu and co-workers reported a case of aspiration of oral secretions; 8 no additional information has been reported in the study. Nishimura and co-workers described a case of post-polypectomy bleeding in one patient with familiar adenomatous polyposis; 7 bleeding was successfully stopped with endoscopic haemostasis. Two cases of perforations were reported, one in a patient who had a SB transplant 29 and the other in a patient with a giant 60-mm invaginated polyp requiring an emergency laparoscopy. 42 A case of hypotension with no bleeding or perforation that required fluid resuscitation possibly secondary to fluid shift/sepsis was described. 29 Two cases of pelvic abscesses were reported: one patient who underwent laparoscopic-assisted DBE developed a pelvic abscess without intestinal perforation and required surgical drainage; 29 the other patient presented with a pelvic abscess after seven polypectomies performed by laparoscopic-assisted DBE. 28
A recent large retrospective study analyzed 257 DBE procedures in paediatric patients and reported an overall complication rate of 5.4%; in patients under 10 years, it was 10.4%. 47
Conclusions
In recent years, CE and BAE have improved the diagnosis and treatment of SB disorders both in adult and paediatric populations. Furthermore, enteroscopy has an addictive diagnostic role thanks to the ability to perform biopsies and therapeutic procedures avoiding surgery in selected cases. In adults, BAE plays a validated role in many diseases, such as OGIB, polyposis syndromes, gastrointestinal tumours, CD, refractory caeliac disease, chronic diarrhoea, and chronic abdominal pain. Data on the use of BAE in paediatric patients are limited; in this population the more common indications are OGIB, CD and SB polyps. As in adults, the paediatric literature reported high diagnostic yield and a low rate of complications, both for diagnostic and interventional procedures. Moreover, we have highlighted that MRE followed by CE has a key role in the optimization of diagnostic work-up of children with suspected SB disease.
Footnotes
Declaration of conflicting interests
None to declare.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.