
Abstract
Background
The need for a blood transfusion, defined as hemoglobin < 70 g/L, is the measure for assessing the risk levels in patients with upper gastrointestinal bleeding (UGIB). However, not all patients with a low hemoglobin level have a poor prognosis.
Objective
We assessed the clinical predictive factors associated with poor short-term prognosis in patients with a low hemoglobin level.
Methods
In this prospective cohort study, all consecutive patients with suspected acute UGIB at Tokyo Metropolitan Tama Medical Center were enrolled between 2008 and 2015. Then, we extracted those who needed a blood transfusion (hemoglobin < 70 g/L) and explored the variables associated with all-cause mortality within 28 days after presentation.
Results
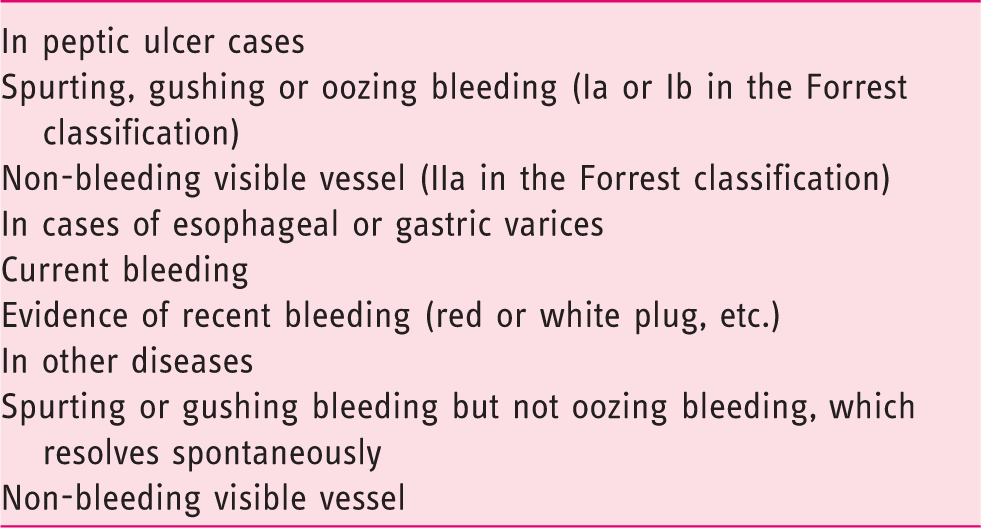
Among 1307 patients, 311 needed a blood transfusion and 13 (4.2%) died from all causes. The presence of high-risk stigmata requiring endoscopic treatment (peptic ulcers; Forrest scores Ia, Ib and IIa; varices with current bleeding or signs of recent bleeding; and spurting or gushing bleeding or visible vessel in other diseases), diagnosed by emergency endoscopy, was a unique factor affecting mortality (odds ratio: 8.47, 95% confidence interval: 1.45–160, P = 0.01). Patients without high-risk stigmata neither died from UGIB nor had rebleeding, irrespective of the hemoglobin levels.
Conclusions
Patients without high-risk stigmata showed a good prognosis even if they needed a blood transfusion. This result could facilitate triage of patients with suspected acute UGIB who only need a blood transfusion.
Keywords
KEY SUMMARY
The need for a blood transfusion is one of the conventional measures for assessing
outpatient management in patients with upper gastrointestinal bleeding (UGIB). In patients with suspected acute UGIB who need a blood transfusion, factors for
predicting good or poor short-term prognosis are still unclear. We were able to clarify the prognosis of the patients with suspected acute UGIB who
needed a blood transfusion by the presence of high-risk stigmata diagnosed by
emergency endoscopy. Patients without high-risk stigmata had a good prognosis even if they needed a blood
transfusion. The need for a blood transfusion was associated with a poor short-term prognosis in
patients with high-risk stigmata, but not in patients without high-risk stigmata. To facilitate triage for the outpatient management of suspected acute UGIB, patients
who need a blood transfusion but do not have any high-risk stigmata should be
stratified into lower risk categories.
Introduction
Upper gastrointestinal bleeding (UGIB) has an incidence of 25–35 hospitalizations per 100,000 adults annually. 1 The current guidelines recommend that risk assessment be performed to stratify patients into higher and lower risk categories. 2 Among the several scoring systems currently available for calculating the risk of UGIB, the most widely known for outpatient management is the Glasgow-Blatchford Score (GBS), which predicts the need for intervention (blood transfusion, endoscopic treatment and surgery) or death.3,4
However, need for a blood transfusion, usually defined as hemoglobin < 70 g/L, is not a suitable outcome for stratifying patients into higher and lower risk categories because a previous study demonstrated that the need for a blood transfusion indicates neither the need for endoscopic or surgical intervention nor a poor prognosis. 5 Therefore, a further risk stratification strategy is needed for patients requiring a blood transfusion. The aim of this study was to identify the clinical factors associated with poor short-term prognosis in suspected acute UGIB patients with a low hemoglobin level to facilitate triage for the outpatient management of suspected acute UGIB.
Methods
Study design and enrolled patients
We performed a secondary data analysis of a prospective cohort of 1307 patients with suspected acute UGIB at Tokyo Metropolitan Tama Medical Center between 2008 and 2015. This study was performed in accordance with the ethical principles for medical research of the Declaration of Helsinki and was approved by the Tama Medical Center Medical Ethics Committee on 1 May 2017. Written informed consent was not obtained and informed consent included an opt-out clause according to the Medical Ethics Committee. The study was observational and reported in accordance with the Strengthening Reporting of Observational Studies in Epidemiology guidelines. 6
The prospective cohort was collected starting in 2008, and the study was conducted at a single tertiary hospital in western Tokyo serving a population of about four million. The patients in the cohort were aged 16 years or older, had suspected acute UGIB, and underwent an emergency endoscopy. Acute UGIB was suspected based on the presence of hematemesis, coffee ground vomit, nasogastric lavage with blood or coffee grounds in the initial examination or melena or black stool as determined by rectal examination or history. We have a policy of performing an emergency endoscopy for all consecutive patients with suspected UGIB and of monitoring their prognosis for 28 days following their first clinical examination.
Figure 1 shows the study flow
diagram. We extracted patients who needed a blood transfusion from the total of 1307
patients in the cohort. The need for a blood transfusion was defined as hemoglobin < 70
g/L at the first examination. The cut-off for hemoglobin was set at 70 g/L because a
previous study showed that patients who received a blood transfusion when the hemoglobin
level fell below 70 g/L had a lower mortality rate than patients who received a blood
transfusion when the hemoglobin level fell below 90 g/L.
7
We divided the patients who needed a blood
transfusion into dead and living patients and compared them using predictive variables.
Study flow diagram.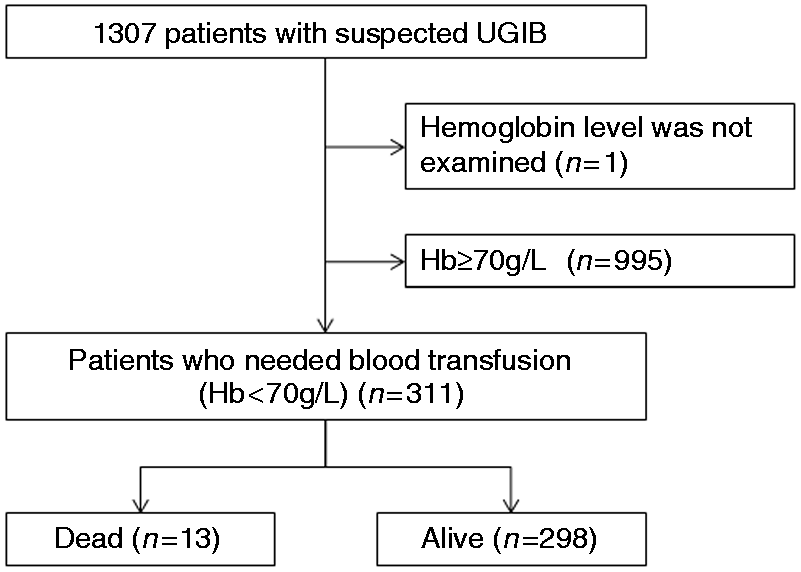
Predictive variables for prognosis and outcomes
The primary outcome was all-cause mortality. The secondary outcomes were death due to UGIB based on the patients’ electronic medical records and rebleeding. When rebleeding was suspected, an emergency endoscopy was performed for confirmation. Rebleeding was defined as the finding of active bleeding by endoscopy, interventional radiology or surgery.
Statistical analysis
We selected a number of variables from among those that had a P-value of < 0.05 in univariable analysis for multivariable logistic regression analysis after considering multicollinearity about primary outcome. We calculated the odds ratio (OR) and 95% confidence interval (CI) of each variable and selected a variable that was significantly associated with the primary outcome. Next, we compared the outcomes among the four groups (hemoglobin < 70 g/L: patients with the selected variable; hemoglobin < 70 g/L: patients without the selected variable; hemoglobin ≥ 70 g/L: patients with the selected variable; and hemoglobin ≥ 70 g/L: patients without the selected variable). For sensitivity analysis, we set another cut-off (hemoglobin < 90 g/L) for the need for a blood transfusion and compared the outcome among another set of four groups. A two-sided P-value of < 0.05 was considered statistically significant. All analyses were done using JMP(r) statistical software version 11.2 (SAS Institute, Inc., Cary, NC, USA). More details are provided in the supplementary materials.
Results
The prognosis of all consecutive patients with suspected UGIB
Of 1307 patients, 1299 (99.4%) underwent an emergency endoscopy while eight patients were unable to do so due to unstable vital signs. The median duration from the first clinical examination to initiating an emergency endoscopy was three hours (interquartile range, 2–5 hours), and 1306 (99.9%) patients were followed up until 28 days after their first clinical examination. Of all consecutive patients with suspected UGIB, 36 patients died due to all-cause mortality (2.8%), 18 patients died due to UGIB (1.4%) and 67 patients experienced rebleeding (5.1%).
The prognosis factor of the patients who need a blood transfusion (hemoglobin < 70 g/L)
Multivariate analysis for all-cause mortality among patients who needed a blood transfusion (hemoglobin <70 g/L).
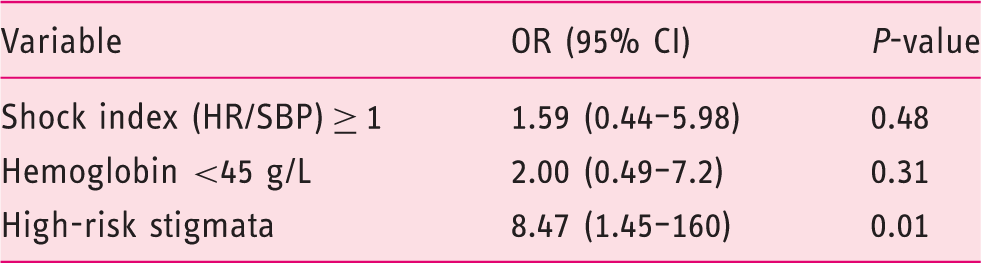
OR: odds ratio; CI: confidence interval; HR: heat rate; SBP: systolic blood pressure.
Comparison of four groups: Hb < 70 g/L or Hb ≥ 70 g/L with or without high-risk stigmata
Figure 2 shows the outcomes of
four groups, namely: the patients without high-risk stigmata who did not need a blood
transfusion (hemoglobin ≥ 70 g/L) (the “-HRS –BT” group), the patients without high-risk
stigmata who needed a blood transfusion (hemoglobin < 70 g/L) (the “-HRS + BT” group),
patients with high-risk stigmata who did not need a blood transfusion (the “+HRS -BT”
group), and patients with high-risk stigmata who needed a blood transfusion (the “+HRS
+BT” group). Of 501 patients in the -HRS –BT group, three died from terminal cancer, two
died from infection and one died from multiple organ failure. The ORs and 95% CIs for
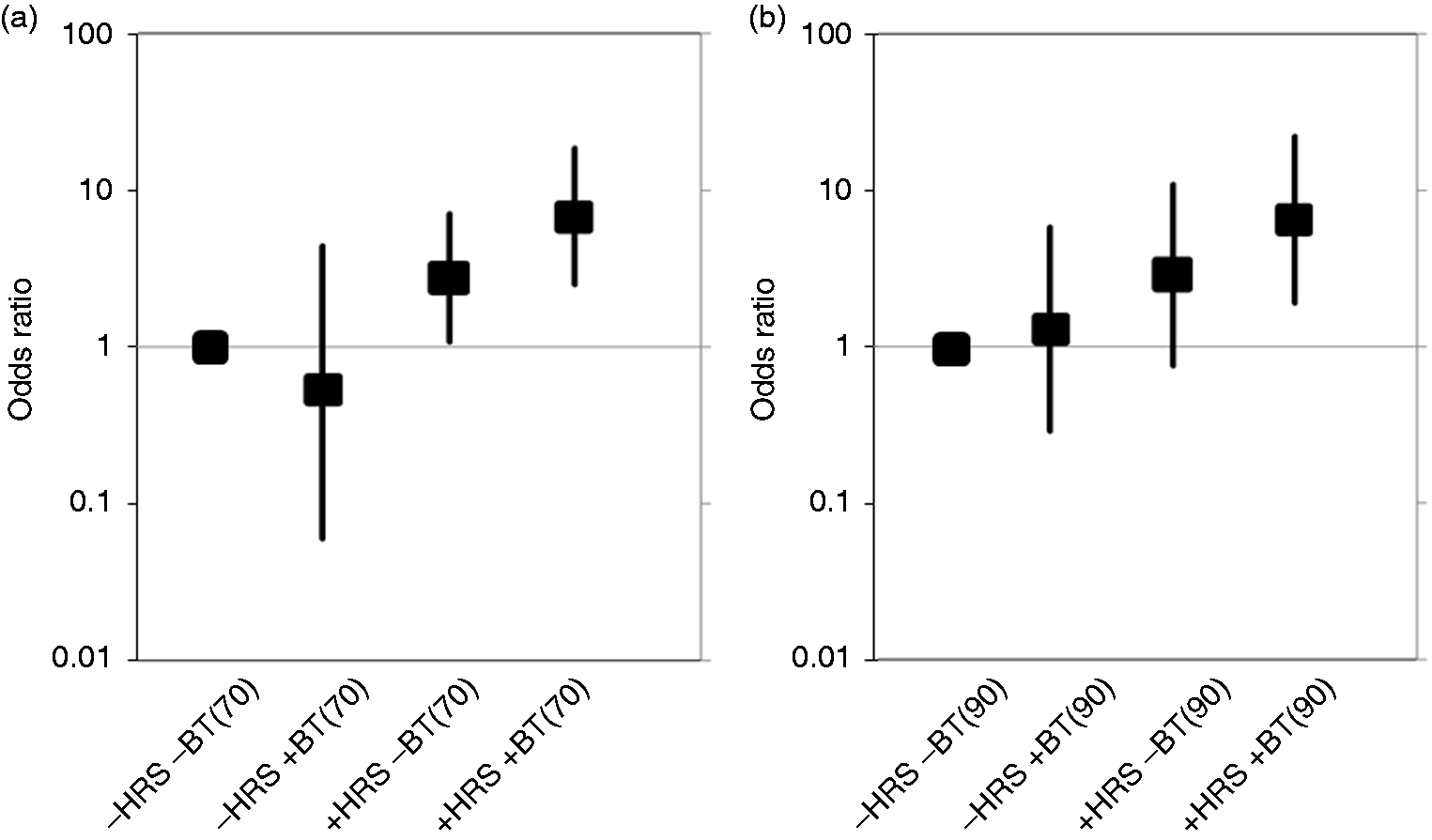
all-cause mortality among the four groups are shown in Figure 3(a). Compared with the -HRS –BT group, the OR
for mortality was 0.54 (95% CI 0.06–4.48) in the -HRS +BT group, 2.77 (95% CI 1.07–7.13)
in the +HRS –BT group and 6.82 (95% CI 2.51–18.5) in the +HRS +BT group. No patients
without high-risk stigmata, including those who needed a blood transfusion (hemoglobin
≥ 70 g/L) and those who did not (hemoglobin ≥ 70 g/L), died due to UGIB or experienced
rebleeding. Outcomes among four groups: with/without need for a blood transfusion (< 70 g/L)
and with/without high-risk stigmata. Association between all-cause mortality and the presence / absence of high-risk
stigmata with / without need for a blood transfusion: (a) need for a blood
transfusion was defined as < 70 g/L; (b) need for a blood transfusion was defined
as < 90 g/L.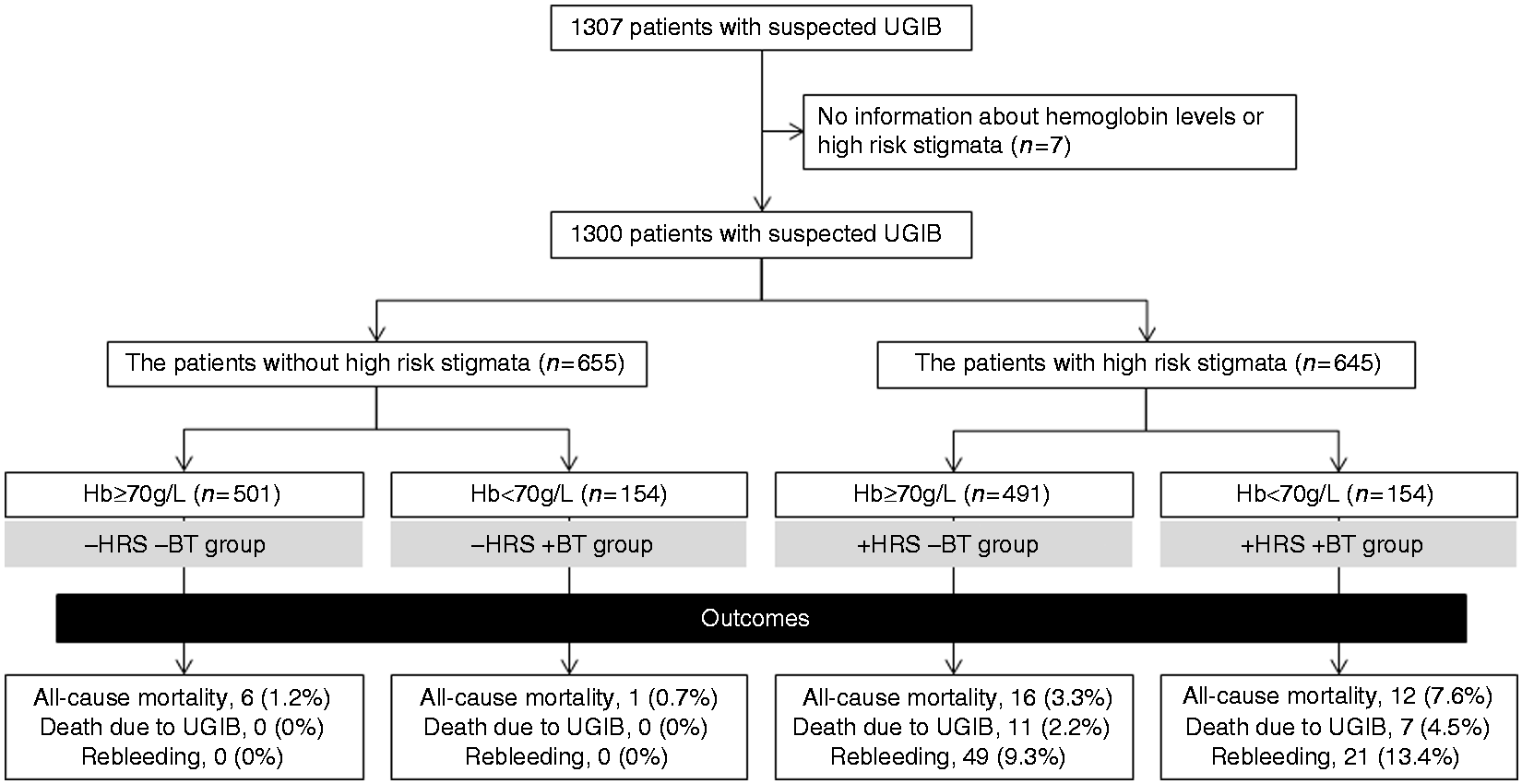
Sensitivity analysis
Comparison of four groups: Hb < 90 g/L or Hb ≥ 90 g/L with or without high-risk stigmata
To evaluate the robustness of these conclusions, we validated them using other cut-off values for hemoglobin, such <90 g/L for the need for a blood transfusion. The ORs and 95% CIs for all-cause mortality among the four groups are shown in Figure 3(b). None of the patients without high-risk stigmata, including both patients who needed a blood transfusion (hemoglobin < 90 g/L) and those who did not (hemoglobin ≥ 90 g/L), died from UGIB or had rebleeding.
Discussion
The short-term prognosis of the patients who needed a blood transfusion (hemoglobin < 70 g/L) differed depending on the high-risk stigmata. Although the patients with high-risk stigmata who needed a blood transfusion (hemoglobin < 70 g/L) had a poor outcome, those without high-risk stigmata who needed a blood transfusion (hemoglobin < 70 g/L) had a good outcome. No patients without high-risk stigmata, including both those who needed and did not need a blood transfusion, either died from UGIB or had rebleeding. Patients without high-risk stigmata may not be hospitalized. Thus, predicting high-risk stigmata was a higher priority than a blood transfusion or a composite outcome including blood transfusion for the purpose of stratifying patients into higher or lower risk categories.
High-risk stigmata were defined by well-established endoscopic findings requiring endoscopic intervention in accordance with international consensus statements.2,14,16–20 The need for a blood transfusion was determined by hemoglobin levels in almost all cases. 7 A low hemoglobin level at first examination can be caused by either of two types bleeding, namely, acute massive bleeding or chronic bleeding. High-risk stigmata may be associated with acute anemia, which could affect short-term prognosis. However, it is difficult to distinguish acute bleeding and chronic bleeding in patients with suspected acute UGIB in an emergent situation. Although most acute massive bleeding cases had high-risk stigmata and the amount of bleeding in a short time directly reflected the hemoglobin levels, chronic bleeding cases had no high-risk stigmata and the amount of bleeding over a longer period reflected gradual changes in hemoglobin levels. We performed an urgent endoscopy for all suspected acute UGIB cases, and the endoscopic findings demonstrated that the patients without high-risk stigmata who needed a blood transfusion were almost all chronic bleeding cases. Thus, the need for a blood transfusion (hemoglobin < 70 g/L) in the non-high-risk stigmata group was not associated with a poor outcome. We obtained a similar result when we set a different cut-off value for the need for a blood transfusion (hemoglobin < 90 g/L) and we performed sub-group analysis by three criteria of high-risk stigmata (shown in Table 1).
These results support stratifying patients with high-risk stigmata into higher risk categories and patients without high-risk stigmata into lower risk categories in cases of suspected acute UGIB, regardless of the need for a blood transfusion. Among the patients with high-risk stigmata, the patients who needed a blood transfusion had a higher risk than those who did not need a blood transfusion. Blood transfusion as an outcome was important only in patients with high-risk stigmata. Thus, patients without high-risk stigmata, even those with severe anemia, may be seen on an outpatient basis because their low hemoglobin value is almost always caused by chronic anemia. The guideline also recommends that patients without high-risk stigmata are considered for early discharge the same or next day. 21 However, they should still undergo selective endoscopy to determine the cause of their anemia.
To predict high-risk stigmata in patients with suspected acute UGIB including variceal and non-variceal bleeding, the Simple Score was previously reported by Horibe et al. 14 The area under the curve (AUC) was 0.74 for the Simple Score and 0.63 for the GBS, demonstrating that the Simple Score was significantly more accurate than the GBS. 14 The Simple Score consists of three variables, namely: “no daily use of PPI during one week before examination (+1 point),” “shock index (HR/SBP) ≥ 1 (+1 point),” and “Urea/creatinine (Cr) ≥ 140 (blood urea nitrogen/Cr ≥ 30) (+1 point),” with a range of 0–3 points. 14 A low hemoglobin level (need for blood transfusion) was not included in the Simple Score. The same study demonstrated that there was no significant association between high-risk stigmata and a low hemoglobin level (need for blood transfusion). 14
Treating blood transfusion as an outcome for risk assessment has two problems. First, predicting the need for a blood transfusion using any scoring system is unnecessary because the need for a blood transfusion can be determined based on the hemoglobin level (transfusion when the hemoglobin level is < 70 g/L) or vital signs.7,22,23 Second, the effectiveness of any scoring system that incorporates the hemoglobin level is massively overvalued for its ability to predict outcomes including blood transfusion for the reason stated earlier, i.e. that the need for a blood transfusion can be determined by the hemoglobin level. 7 Actually, the AUCs of the GBS were 0.68–0.85 for only blood transfusion and 0.34–0.68 for composite outcomes excluding blood transfusion, indicating that the removal of blood transfusion from the outcomes decreased the AUC of the GBS.6,8,24,25 The effectiveness of the GBS depends on the association between the hemoglobin value included in the GBS and blood transfusion. Moreover, blood transfusion was the most frequent outcome; the percentage of blood transfusions, endoscopic interventions, interventional radiology, surgery, rebleeding and mortality for UGIB was 59.1–84.4%, 30–54%, 2–7.6%, 1–1.8%, 5–29.8% and 3.4–19.6%, respectively.5,24,26,27 Thus, blood transfusion as an outcome had a high impact on the AUC of the GBS. Using the GBS for suspected cases of acute UGIB runs the risk of miscategorizing patients with chronic anemia into the high-risk group. Patients who need only a blood transfusion may not require hospitalization.
Our study has two limitations. First, the prognosis of patients without high-risk stigmata is still unclear if they were treated as outpatients, since all our participants were treated as inpatients. A good prognosis may be due to the effect of treatment in post-admission follow-up. However, despite our policy of following up all suspected UGIB cases post-admission, we were unable to detect any severe adverse events associated with UGIB until 28 days after the first examination. We also compared patients with and without high-risk stigmata who were treated similarly post-admission, and were able to demonstrate that the prognosis of patients without high-risk stigmata who received optimal treatment was better than that of patients with high-risk stigmata who received the same treatment.
Second, this study was conducted at a single tertiary care center. However, as the only acute-care general hospital, Tama Medical Center covers not only tertiary care but primary care and secondary critical care as well. Thus, although this secondary data analysis of a prospective cohort study was conducted at a single institution, our study population was a highly representative cross-section of the general UGIB population. Moreover, there was little bias in evaluating high-risk stigmata because 1299 (99.4%) patients underwent an emergency endoscopy and the median time was three hours, even if the suspected acute UGIB patients were thought to be mild cases.
In conclusion, the short-term prognosis of patients without high-risk stigmata, including those who needed only a blood transfusion (hemoglobin < 70 g/L), was good. High-risk stigmata requiring endoscopic treatment was an important outcome for predicting prognosis. On the other hand, blood transfusion was not a prognostic factor in those without high-risk stigmata. A combination of the presence of high-risk stigmata and the need for a blood transfusion achieved the greatest risk stratification. Considering that the need for a blood transfusion can easily be assessed by hemoglobin levels, a scoring system should be constructed to predict only high-risk stigmata and the need for a blood transfusion should not be considered as a risk stratification outcome.
Supplemental Material
Supplemental material for Absence of high-risk stigmata predicts good prognosis even in severely anemic patients with suspected acute upper gastrointestinal bleeding
Supplemental Material for Absence of high-risk stigmata predicts good prognosis even in severely anemic patients with suspected acute upper gastrointestinal bleeding by Masayasu Horibe, Yuki Ogura, Juntaro Matsuzaki, Tetsuji Kaneko, Takuya Yokota, Osamu Okawa, Yukihiro Nakatani, Eisuke Iwasaki, Toshihiro Nishizawa, Naoki Hosoe, Tatsuhiro Masaoka, Naohisa Yahagi, Shin Namiki and Takanori Kanai in United European Gastroenterology Journal
Footnotes
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethics approval
This study was approved by the Tama Medical Center Medical Ethics Committee on 1 May 2017.
Informed consent
Written informed consent was not obtained and informed consent included an opt-out clause according to the Medical Ethics Committee.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.