
Abstract
Background
Perihilar cholangiocarcinomas are often considered incurable. Late diagnosis is common. Advanced disease therefore frequently causes questioning of curative surgical outcome.
Aim
This study aimed to develop a prediction model of curative surgery in patients suffering from perihilar cholangiocarcinomas based on preoperative endosonography and computer tomography.
Methods
A cohort of 81 patients (median age 67 (54–75) years, 62% male) with perihilar cholangiocarcinoma was retrospectively analyzed. Multivariate logistic regression analysis of staging variables taken from the European Staging System was performed and applied to ROC analysis.
Results
The correlation of predicted rates of eligibility for surgery with actual rates reached AUC values between 0.652 and 0.758 for endosonography and computer tomography (p < 0.05 each). Best prediction for curative surgical option was achieved by combining endosonography and computer tomography (AUC: 0.787; 95% CI 0.680–0.893, p < 0.0001). A predictive model (pSurg) was developed using multivariate analysis.
Conclusions
Our predictive web-based model pSurg with inclusion of T, N, M, B, PV, HA and V stage of the recently published European Staging System for perihilar cholangiocarcinoma results in highly significant predictability for curative surgery when combining preoperative endosonography and computer tomography, thus allowing for better patient selection in terms of possibility of curative surgery.
Key summary
Summarize the established knowledge on this subject: Perihilar cholangiocarcinomas (pCCA) are often considered incurable. Surgical resection is associated with high mortality and morbidity rates. Various staging systems exist, none predicting operability. European Staging System (ESS) might overcome the limitation of former staging systems. What are the significant and/or new findings of this study? Adequate preoperative staging of pCCA by means of computed tomography and endoscopic ultrasonography is feasible. ESS is valuable for staging patients with pCCA. This is the first predictive model for estimating the likelihood of curative surgery in patients with pCCA. A newly developed web-based (www.pmal-score.org) score refers patients with pCCA to either potentially curative surgery or to primary non-surgical oncological treatment
Introduction
Cholangiocarcinomas (CCA) represent a heterogeneous group of malignant transformations of epithelial cells of the bile duct presenting markers of cholangiocyte differentiation. Currently, the most common classification divides CCAs into three subgroups on the basis of their anatomical location including intrahepatic, perihilar, and distal cholangiocarcinomas. These subsets differ not only in their anatomic origin, but also in epidemiology, pathogenesis and treatment.1–3 This leads to different demands in staging systems and therapeutic approaches. A simple, reproducible and comprehensive staging system is needed not only to identify the appropriate therapeutic option and avoid dispensable operations, but also to evaluate outcomes over time and between institutions with respect to quality assessment.
Perihilar cholangiocarcinoma (pCCA) is localized to the area between the second-degree biliary branches and the junction of the cystic duct and the common bile duct. 2 Because it was first described by Klatskin in 1965, pCCA is commonly named the Klatskin tumor. 4 It accounts for 50%–67% of all cholangiocarcinomas.5–7 A variety of risk factors for pCCA, which accounts for 10% of cases, have been identified, including advanced age, male gender, primary sclerosing cholangitis, parasitic infections, cholelithiasis, cirrhosis, inflammatory bowel disease and chronic pancreatitis.2,8,9
CCA is the second most common primary liver tumor worldwide.5,10,11 Since incidence and mortality rates have risen, it represents a challenging and controversial disease.
Most of these tumors are commonly diagnosed in the advanced stage of the disease, which worsens their very poor survival prognosis. The current five-year survival rate after surgery, even in selected cases, rarely exceeds 35%.6,7,9,12,13 The only potentially curative treatment for this type of cancer is the complete surgical resection of the tumor that can be applied to only a minority of patients with well-localized lesions. In selected cases liver transplantation can be performed.6,14
For the appropriate prediction of operability, the comparison of results over time and among different centers is needed. The major barrier to comparing results among centers and identifying the best therapeutic approach according to the type and extent of the disease is the lack of such a reliable, comprehensive staging system. The Bismuth-Corlette classification is widely used, but it does not include critical data about distant metastases, though this classification has recently been extended to also take into account arterial and venous encasement. 7 Other systems are restricted to each center’s experience and do not provide enough information for guiding therapy, including liver transplantation. One currently available staging system is the Memorial Sloan-Kettering Cancer Center staging system similar to Bismuth-Corlette, which is primarily used for the evaluation of patients who are eligible for a surgical resection. The tumor-node-metastasis (TNM) staging system as a commonly used staging system is specifically intended for predicting prognosis; however, it is based on resection results, and therefore it is not applicable to the majority of pCCA patients with unresectable disease or preoperatively, which must be staged on clinical, rather than pathologic, criteria. 13
Although being a very informative and comprehensive system, the European Staging System (ESS) has its limitations in inter-institutional comparison and data collection by requiring extensive data from different phases of preoperative care, which may not always be available at one particular setting. 15
The diagnostic evaluation consists of, in addition to physical examination, blood counts and liver function tests of abdominal computed tomography (CT) scan or magnetic resonance imaging (MRI), endoscopic retrograde or percutaneous transhepatic cholangiography (ERCP) and possibly endoscopic ultrasonography (EUS). 16 While CT and MRI have the advantage of delineating hepatobiliary anatomy, localizing lymphadenopathy and additionally allowing staging of distant metastases, EUS provides more accurate information of the distal extrahepatic biliary tree, hilar lesions and vasculature. Hence, the above-mentioned techniques should not be considered competitive but complementary and in the authors’ opinions may all be necessary as part of a surgical assessment.
Thus, the aim of this study was to more specifically evaluate the value of the imaging methods EUS and CT to identify detailed anatomical and pathological factors that predict the possibility of curative-intended resection in patients with pCCA.
Materials and methods
Study design
We performed a retrospective study analyzing patients with histologically proven pCCA undergoing CT scan, EUS and surgical exploration. Informed, written consent from all patients was obtained before investigations were performed. This study was performed in accordance with the Declaration of Helsinki 1975 and the International Conference on Harmonization Good Clinical Practice guidelines and was waived by the local ethical review board of Münster, Germany because of its retrospective study design (#2016-046-f-S; April 4, 2016). A total of 81 of 109 consecutive patients at our tertiary referral center who underwent diagnostics for perihilar tumors between 2002 and 2013 and who fulfilled the inclusion criteria were enrolled.
Baseline characteristics of patients with pCCA tumor.
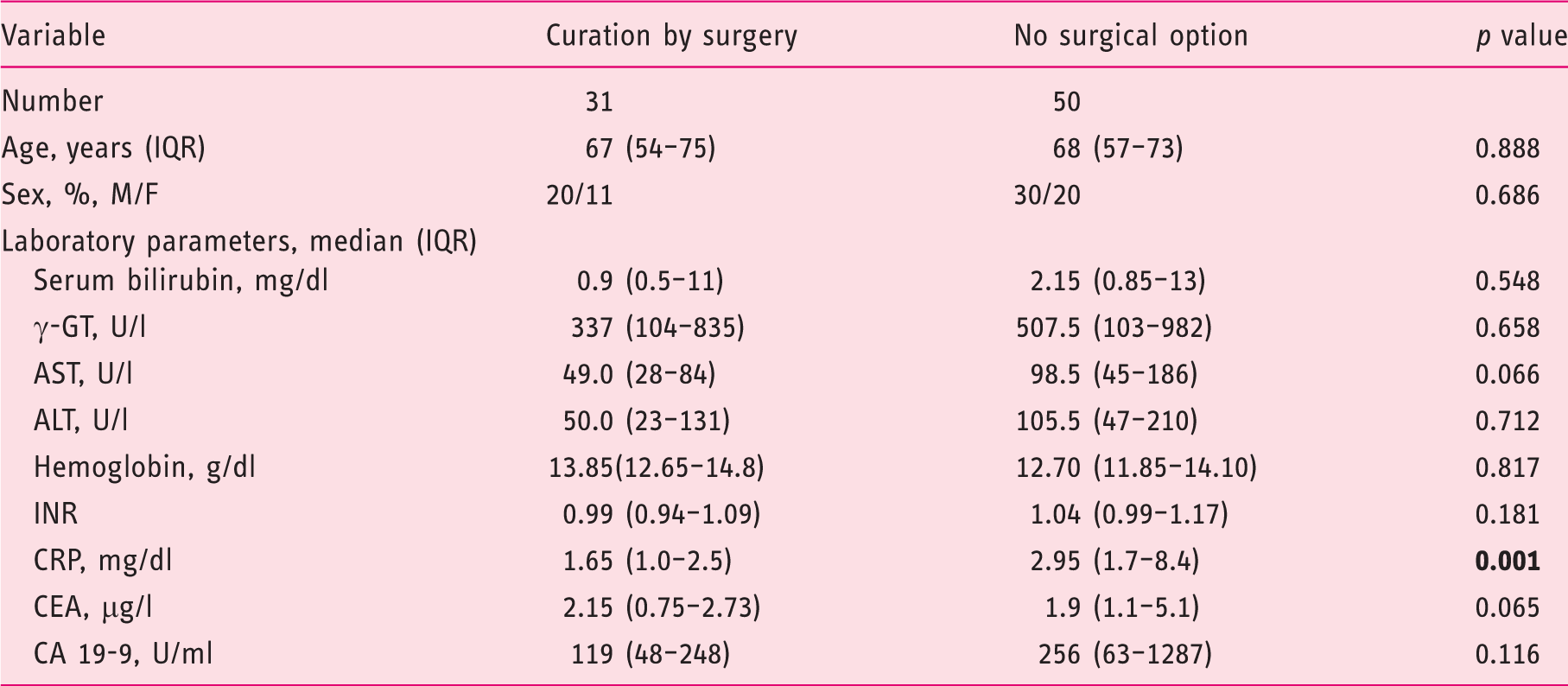
pCCA: perihilar cholangiocarcinoma; M: male; F: female; IQR: interquartile range; γ-GT: gamma-glutamyl transferase; AST: aspartate aminotransferase; ALT: alanine aminotransferase; INR: international normalized ratio; CRP: C-reactive protein; CEA: carcinoembryonic antigen; CA 19-9: cancer antigen 19-9. Bold variables indicate significance.
Procedures
The following procedure descriptions were adapted from a previous publication by the authors. 17 All endoscopic maneuvers were executed by highly experienced investigators according to the generally accepted guidelines with an ERCP/EUS case volume greater than 200/year. 18 All endoscopic procedures were performed under conscious sedation (propofol combined with pethidine) according to the German guidelines. 19
The EUS procedures were performed using a radial or linear echoendoscope with up to a 10 MHz frequency (EG-3670 URK and EG-3870 UTK, Pentax Medical/Hitachi Medical Systems, Tokyo, Japan) with the patient lying in the left lateral position.
CT examinations were performed using multi-slice CT scanners (16- and 64-slice scanner, Siemens AG, Forchheim, Germany) using a standardized tube voltage at 120 kV with a detector configuration of 16 mm × 0.75 mm and 32 mm × 0.6 mm, respectively, and a pitch of 0.75. In the majority of cases, the images were reconstructed with a slice thickness of 1.0 mm (reconstruction increment of 0.8) with a soft tissue reconstruction kernel (B30). A volume of 120–150 ml intravenous contrast agent (Ultravist 370®, Bayer Schering Pharma AG, Leverkusen, Germany) was applied at a constant flow rate of 3–4 ml/s depending on the acquired phases of contrast enhancement. Dual-phasic images were acquired with a scan delay of 45 seconds (late arterial, as obtained by test or care bolus technique) and 75 seconds (portal-venous). The imaging protocol did not differ from the standardized protocol used in clinical routines. For image assessment, the reconstructed images were assessed on a standard workstation (Syngo, Siemens AG, Forchheim, Germany) with cine mode and multiplanar reformation capabilities. In 46 cases, image analysis was possible only on hard copies. Image data were analyzed independently by one radiologist, blinded to the final diagnosis, who evaluated the pCCA characteristics and the involvement of regional lymph nodes or distant metastases. Furthermore, tumor size and localization were assessed.
All participants underwent surgery with a curative intention or for staging laparoscopy at the Department of General and Visceral Surgery of Münster University hospital for definite staging assessment.
Staging of pCCA
In retrospect, all patients were preoperatively staged according to the new staging for pCCA according to DeOliveira. 7 For each diagnostic tool (EUS and CT) the following information was obtained: T stage, N stage, M stage, involvement of the bile ducts (B stage), involvement of the portal vein (PV stage), involvement of the hepatic artery (HA stage) and estimation of the liver remnant volume by CT scan (V stage). Because the macroscopic form (F stage), recorded as periductal or sclerosing type, mass-forming type or intraductal polypoid type, is difficult to assess preoperatively, which is in accordance with the findings by Ismael et al., 15 we did not include it in our analysis.
Statistical analysis
Data were analyzed using SPSS 17.0 (SPSS Inc, Chicago, IL, USA). Results are expressed as medians with interquartile range (IQR), or number/percentages. Non-continuous parameters were analyzed by chi-square test and continuous parameters were analyzed by Mann-Whitney U-test as appropriate. A p value below 0.05 was considered statistically significant. The predictive model for multivariate logistic regression was calculated based on the T, N, M, B, PV, HA and V stage of the new staging system by DeOliveira. 7 The predictive factor X was generated as the weighted sums of the predictive factors, weighed with their regression coefficients from the binary logistic regression analysis. Final probability of curative surgical option (pSurg) was calculated as follows: pSurg = 1/(1 + e–x). A receiver operator characteristic (ROC) curve analysis in the patient cohort with pCCA with correlation of predicted (EUS, CT and the combination of the two diagnostic tools) versus actual rates of eligibility for surgery was performed. The area under the curve (AUC), 95% confidence intervals (95% CI) and p values for each of the diagnostic tools were plotted. Predicted rates of curative surgery were presented using box plots.
Results
A total of 81 out of 109 screened patients were included for statistical analysis. Patients who underwent curative surgery (n = 31) were compared to 50 individuals who intraoperatively had no option for curative surgical resection because of extended disease. The median age was 69 (58–76) years and did not differ statistically between the two groups. Gender distribution was similar (Table 1). Laboratory parameters were analyzed. C-reactive protein (CRP) (1.65 [1.0–2.5] versus 2.95 [1.7–8.4] p = 0.001) was the only laboratory value that was significantly higher in the cohort with no curative surgical option. Detailed baseline characteristics are presented in Table 1.
B stage, T stage, N stage, M stage, PV stage, HA stage and V stage according to the new classification ESS 7 were assessed by EUS or CT and compared with histopathology and intraoperative findings.
Multivariate analysis
Multivariate analysis for prediction of curative surgical option (logistic binary regression).
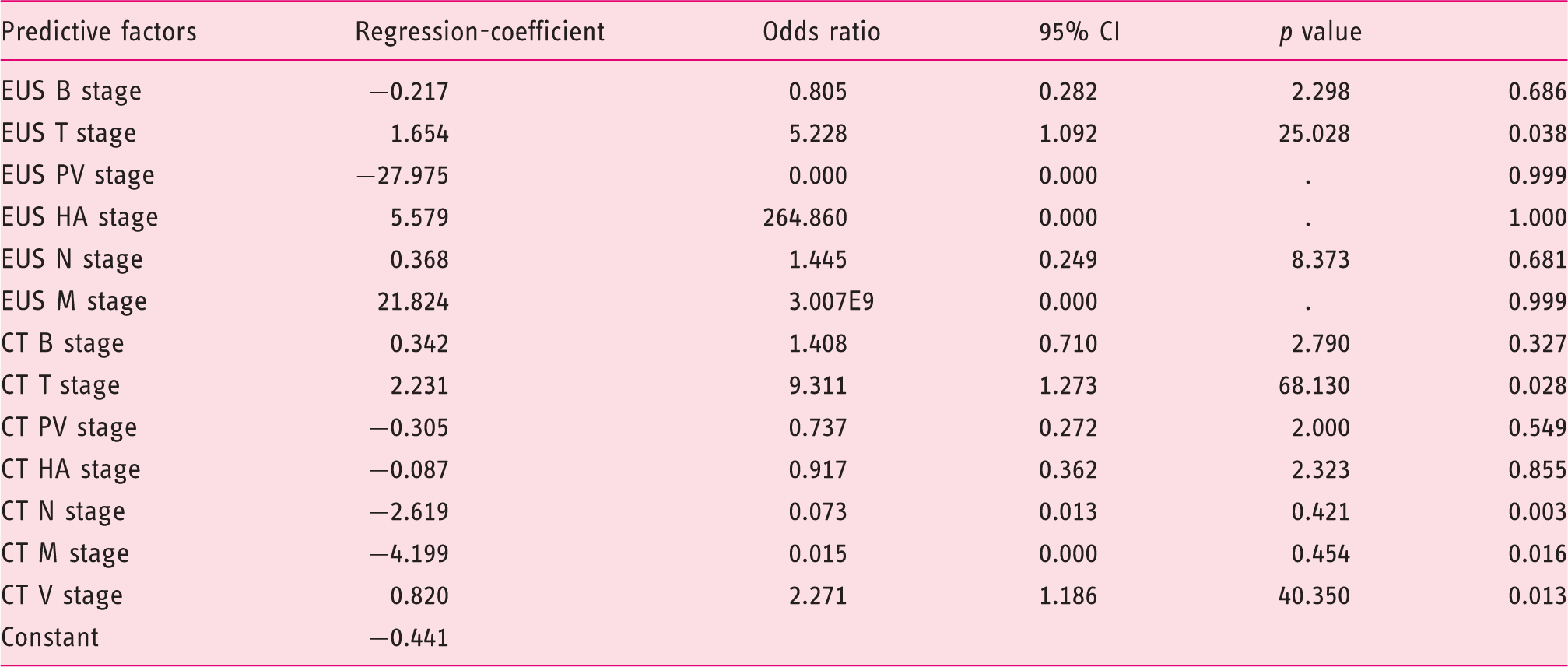
EUS: endoscopic ultrasonography; CT: computed tomography; B stage: bile ducts; PV stage: involvement of the portal vein; HA stage: involvement of the hepatic artery; T: tumor; N: node; M: metastasis; V stage: estimation of the liver remnant volume; CI: confidence interval.
Predicting factor pSurg and ROC analysis
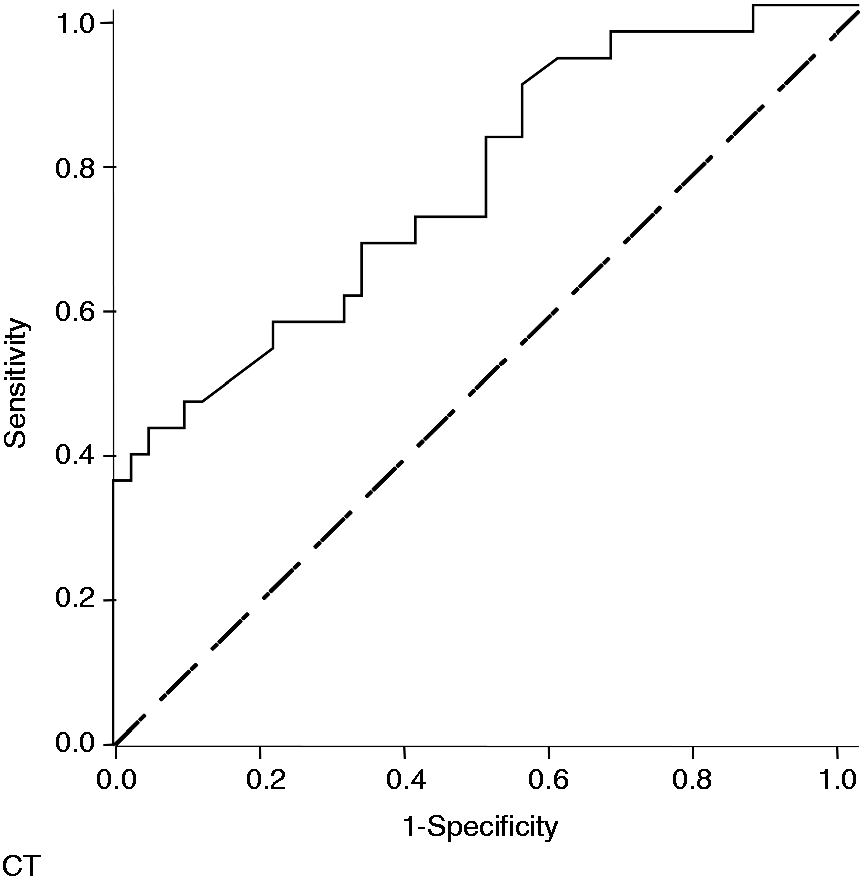
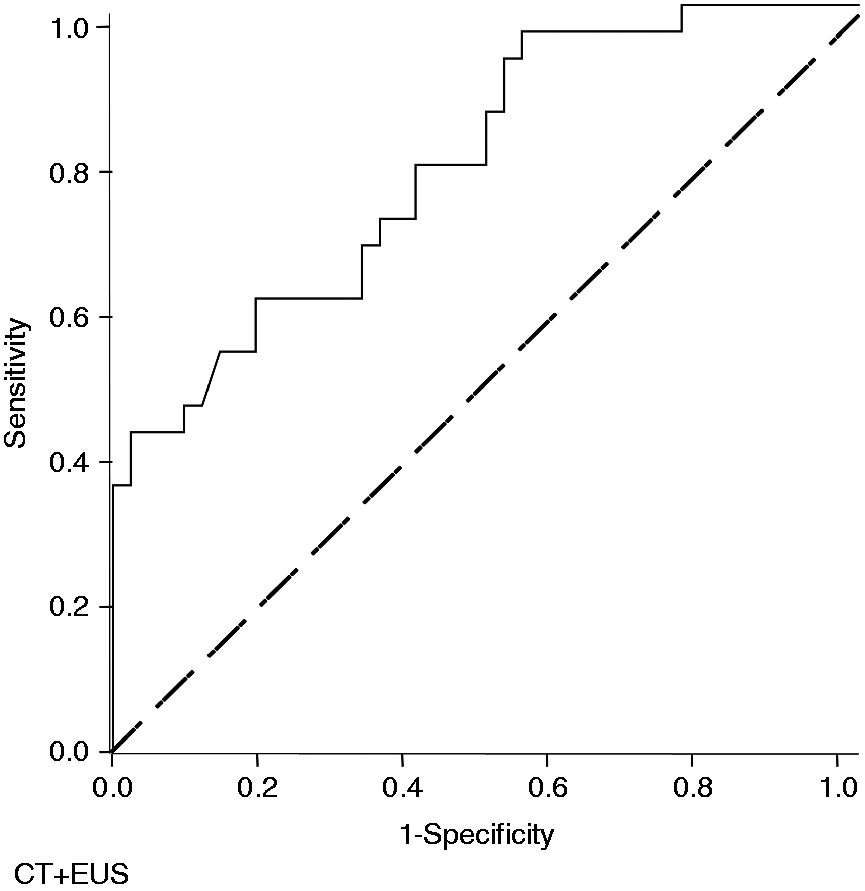
Based on 13 predictors, a risk score for curative surgery was developed by logistic regression (X = −0.217*[EUS B stage] + 1.654*[EUS T stage]−27.975*[EUS PV stage] + 5.579*[EUS HA stage] + 0.368*[EUS N stage] + 21.824*[EUS M stage] + 0.342*[CT B stage] + 2.231*[CT T stage]−0.305 [CT PV stage]−0.087*[CT HA stage]−2.619*[CT N stage]−4.199*[CT M stage] + 0.820 [V stage]−0.441). Using ROC analysis and AUC calculation, the correlation of predicted rates with actual rates of eligibility for surgery reached AUC values of 0.652 and 0.758 for EUS and CT scan, respectively (p < 0.05 each, Figures 1 and 2). Best significant correlation between predicted curative surgery and the actual curative surgery was found by ROC with combination of EUS and CT (AUC: 0.786; 95% CI 0.679–0.892, p < 0.0001), Figure 3).
Correlation of predicted (EUS) versus actual rates of eligibility for surgery in the patient cohort with Klatskin tumors (AUC:0.652; 95%CI 0.530–0.775, p = 0.022). Bold line: ROC curve. Correlation of predicted (CT) versus actual rates of eligibility for surgery in the patient cohort with Klatskin tumors (AUC:0.758; 95%CI 0.643–0.873, p < 0.0001). Bold line: ROC curve. Correlation of predicted (EUS and CT) versus actual rates of eligibility for surgery in the patient cohort with Klatskin tumors (AUC:0.786; 95%CI 0.679–0.892, p < 0.0001). Bold line: ROC curve.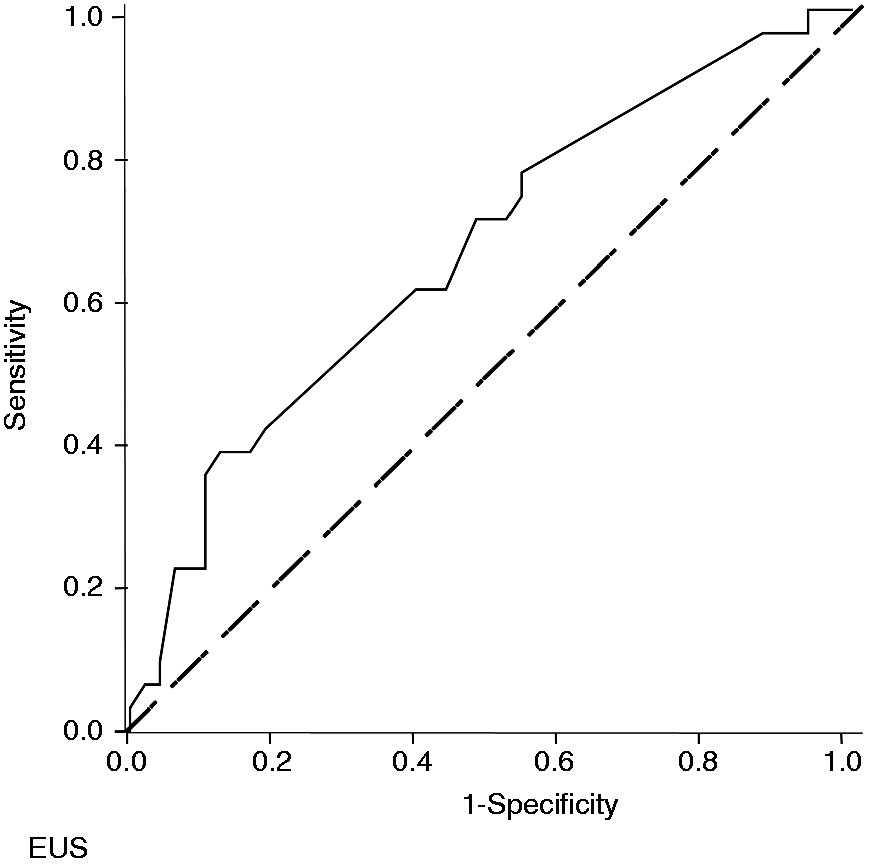
For clarification, predicted versus actual rates of curative surgery are presented in Figure 4: The predicted median rates of curative surgery were between 6% and 93% (first (lowest) quarter by curative surgery prediction 13% (IQR 6–19%), second quarter 35% (29%–42%), third quarter 65% (61%–71%), fourth (highest) quarter 90% (89%–93%)).
Predicted versus actual rates of curative surgery. Patients were classified into quarters according to their individual predicted probability of curative surgery (boxes represent the IQR; whiskers indicate the minimum and maximum values, but are not longer than 2 times the length of the corresponding box), which is plotted against the actual curative surgery rate for the quarters.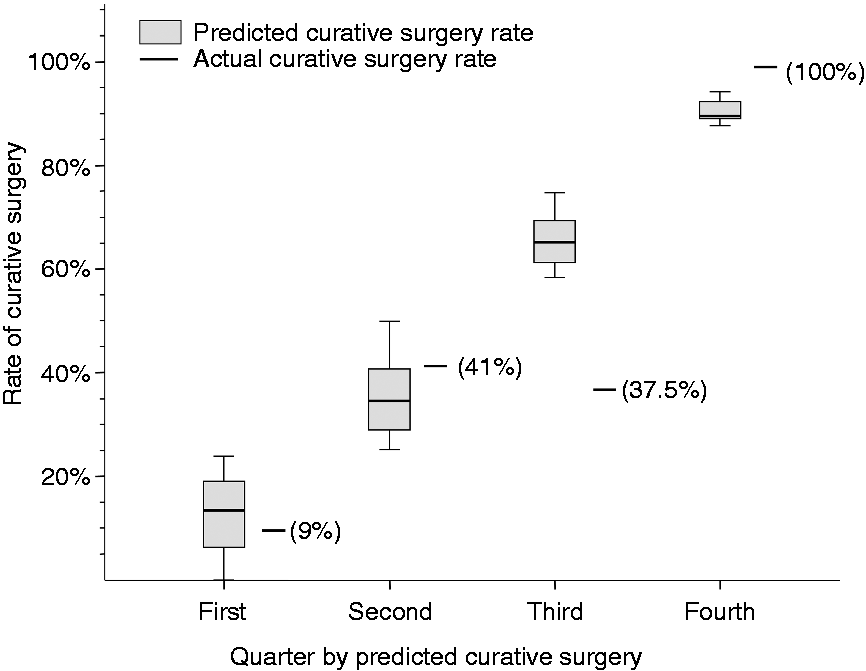
Sensitivity and specificity rates of risk score pSurg predicting curative surgery.
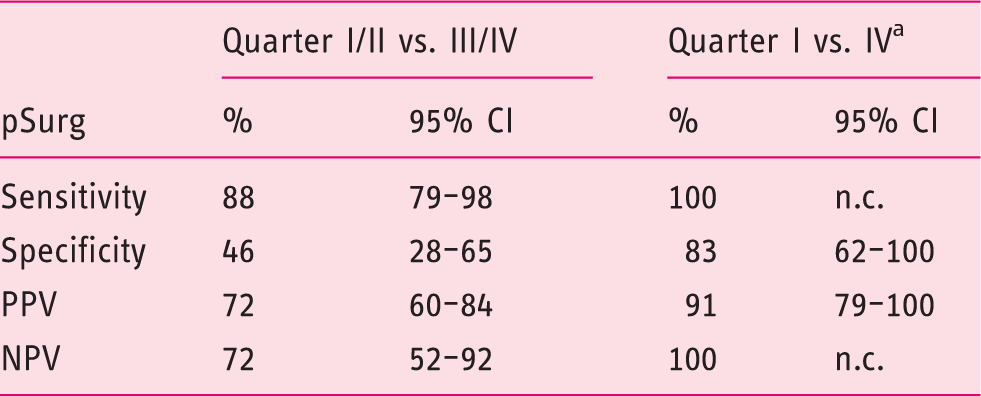
pSurg lowest quarter considered as inoperable, highest quarter as operable.
pSurg: final probability of curative surgical option; PPV: positive predictive value; NPV: negative predictive value; n.c.: not calculable because all cases considered were truly curative operable; CI: confidence interval.
Discussion
Surgical resection is the main column of potentially curative treatment for pCCA. However, less than 25% of patients present with early-stage tumor disease and can be resected with curative intention. 18 Furthermore, surgical resection of pCCA is associated with high mortality and morbidity rates up to 6% and 38%,19–22 respectively, indicating that only selected patients might achieve beneficial effects from operative treatment. Thus, adequate staging of tumor disease is crucial to guide further treatment and to avoid unnecessary surgery. Commonly used staging systems for pCCA include the Bismuth-Corlette classification, the Memorial Sloan-Kettering Cancer Center staging system and the American Joint Committee on Cancer/Union for International Cancer Control TNM system.23,24 However, these are based on surgical pathology and therefore cannot predict operability before surgery. In order to potentially overcome this limitation, a new ESS was published in 2011 7 and is continuously evaluated in a prospective registry ever since, but has not yet been validated.25,26 Recently, Ismael and colleagues retrospectively evaluated its clinical applicability in 47 patients admitted for resection of pCCA. 15 The authors criticized the ESS for the large number of variables needed to be assessed and because not all data seem available by preoperative diagnostics. In their study, 30% of patients required data from the preoperative, intraoperative and postoperative setting to be accurately staged. Thus, the authors concluded that ESS is limited for its use in surgical planning. However, the authors included only CT scanning for preoperative assessment of the variables. In our study, we combined endosonographic and radiology findings for the documentation of the variables. Except for F stage, all variables could be easily assessed preoperatively by the above-mentioned imaging modalities in our patient cohort, demonstrating applicability of the ESS in clinical practice. On the other hand, solely looking at the individual parameters of the ESS might not help in the process of decision making regarding operability.
The decision-making process might be facilitated if the treating physician had reliable clinical and biochemical markers for prediction of malignancy. By univariate and multivariate analysis, we identified various standard clinical and laboratory variables that were closely and independently associated with malignancy in bile duct obstruction.
For instance, multivariate analysis of the 13 factors that comprise the ESS revealed only EUS T stage (p = 0.038), CT T stage (p = 0.028), CT N stage (p = 0.003), CT M stage (p = 0.016) and CT V stage (p = 0.013) as independent predictors for operability (Table 2).
Contrariwise, the decision-making process might be accelerated if the treating physician had a quickly assessable and reliable calculating model on hand to predict operability in patients with pCCA. We therefore developed a stratified scoring system for the prediction of operability using the method described in our previous study. 27
Our prediction model (pSurg) is based on modified ESS criteria for staging pCCA using EUS and CT, thus making it easily applicable during routine clinical practice and predicting operability with high accuracy. When using our prediction model, AUCs of the ROC curves of predictive operability were 0.786; 95% CI 0.679–0.892, p < 0.0001 (Figure 3). In case of calculated probability for surgery between 25% and 75%, adequate conclusion of operability is less likely because of low sensitivity and specificity rates. In these patients, our predictive model is less practicable. However, patients in our cohort who were assigned to either the first or fourth quarter of our prediction model correlated well with the actual rate of operability allowing adequate assessment with high sensitivity and specificity rates of 100 and 83%, respectively. For simple use of our predictive model, we have developed a web-based application “pSurg” (www.pmal-score.org) to allow for rapid calculation of the probability of operability in patients with pCCA. It is speculative whether other complementary imaging techniques such as endoscopic cholangioscopy, magnetic resonance cholangiopancreatography (MRCP) or positron emission tomography CT would have an additional value in the prediction of operability.
In our opinion, MRCP or cholangioscopy would not add much value, since these methods do not permit any reliable statement on tumor extent; however, the diagnostic value for detection of pCCA remains unaffected. Contrast CT has its strength in detecting vascular involvement (portal vein and hepatic artery), more so than MRCP or MRI.28–31 However, the relationship between the tumor and the vasculature is an essential parameter of the ESS and therefore of our predictive score. Recently published European Society for Medical Oncology (ESMO) guidelines 32 recommend EUS especially for lymph node staging adjunct to radiographic imaging such as MRI or CT. Nevertheless, positron emission tomography CT could certainly play a role in better detection of distant metastases. Since MRI or MRCP were not available for all our included patients (n = 21), and only full datasets can be used for statistical analysis, we did not include these imaging modalities in our analysis.
Conclusions
This is the first predictive model for estimating the likelihood of curative surgery in patients with pCCA based on the extended ESS by DeOliveira et al. 7 Better prediction enables both earlier curative surgery of pCCA and improved management, which may result in better selection of patients with curative option and possibly reduced morbidity and mortality. Our score (pSurg) is an easy, simple and applicable method in the primary evaluation of patients with pCCA using only standard diagnostic imaging modalities. It can be used web based (www.pmal-score.org) to refer patients with pCCA to either potentially curative surgery or to primary non-surgical oncological treatment. However, whether an individual patient (in special circumstances) has to undergo surgical exploration to be sure of inoperability remains an individual decision.
Limitations
We acknowledge that possible misclassification or information bias as a result of the retrospective study design might affect the veracity of the findings of our study. In addition, all patients in our study cohort underwent surgery with a curative intention or for staging laparoscopy possibly leading to a potential patient selection bias and thus, possibly limiting the applicability of our predictive model. MRI variables were not used in the model because a minority of patients (n = 21) were evaluated with this modality. Furthermore, our newly developed score should be validated in an external validation cohort with the same imaging modalities as used in ours. Nevertheless, we are able to show that by combining various preoperative imaging modalities accurate prediction of operability by means of ESS seems highly feasible.
Footnotes
Declaration of conflicting interests
None declared.
Ethics approval
This study was performed in accordance with the Declaration of Helsinki 1975 and the International Conference on Harmonization Good Clinical Practice guidelines and was waived by the local ethical review board of Münster, Germany because of its retrospective study design (#2016-046-f-S; April 4, 2016).
Funding
This work was supported by grants to A. Hüsing-Kabar from the Dean’s Office of the medical faculty of the Westfälische-Wilhelms University of Münster, Germany.
Informed consent
Informed consent of patients prior to procedures and surgery was obtained in all cases.