
Abstract
Background and aim
Endoscopy and magnetic resonance imaging (MRI) are used routinely in the diagnostic and preoperative work-up of rectal cancer. We aimed to compare colonoscopy and MRI in determining rectal tumor height.
Methods
Between 2002 and 2012, all patients with rectal cancer with available MRIs and endoscopy reports were included. All MRIs were reassessed for tumor height by two abdominal radiologists. To obtain insight in techniques used for endoscopic determination of tumor height, a survey among regional endoscopists was conducted.
Results
A total of 211 patients with rectal cancer were included. Tumor height was significantly lower when assessed by MRI than by endoscopy with a mean difference of 2.5 cm (95% CI: 2.1–2.8). Although the agreement between tumor height as measured by MRI and endoscopy was good (intraclass correlation coefficient (ICC) 0.7 (95% CI: 0.7–0.8)), the 95% limits of agreement varied from –3.0 cm to 8.0 cm. In 45 patients (21.3%), tumors were regarded as low by MRI and middle–high by endoscopy. MRI inter- and intraobserver agreements were excellent with an ICC of 0.8 (95% CI: 0.7–0.9) and 0.9 (95% CI: 0.9–1.0), respectively. The survey showed no consensus among endoscopists as to how to technically measure tumor height.
Conclusion
This study showed large variability in rectal tumor height as measured by colonoscopy and MRI. Since MRI measurements showed excellent inter- and intraobserver agreement, we suggest using tumor height measurement by MRI for diagnostic purposes and treatment allocation.
Introduction
Endoscopy is the preferred diagnostic method for evaluation of rectal cancer. In the preoperative work-up of patients with rectal cancer, pelvic magnetic resonance imaging (MRI) is performed routinely for locoregional tumor staging.1,2 Clinicians often use either one or both modalities to determine rectal tumor height.
Rectal tumor height can be defined as the distance between the distal end of the tumor and one of the following landmarks: the anorectal junction (ARJ), dentate line, or anal verge. The ARJ, which is the upper margin of the anal canal, is the junction between the rectal columnar epithelium and the squamous epithelium of the anal canal. Just above the ARJ, the rectum will be increasingly surrounded by perirectal fat of the mesorectum. The mesorectum is important for surgeons to ensure a free resection margin to the mesorectal fascia.
Endoscopic landmarks include the dentate line and anal verge. The dentate line lies just beneath the ARJ and is a scalloped demarcation formed by the anal valves, the beginning of the columns of Morgagni. The anal verge is the junction of hair-bearing skin of the buttocks to non-hair-bearing skin of the anal canal and both are covered with squamous epithelium.
There is radiological consensus as to how to measure rectal tumor height by MRI using the ARJ as a landmark, which is used preferably by surgeons. 3 However, according to international clinical guidelines, rectal tumor height should be measured by rigid sigmoidoscopy and is defined as the distance from the anal verge.1,2 Rigid sigmoidoscopy is not used consistently in clinical practice, and is increasingly replaced by flexible endoscopy. Furthermore, for flexible endoscopy a standardized method for rectal tumor height measurement is lacking. Hence, measurements by these various techniques may differ, potentially leading to alternative treatment strategies. It is well established that neoadjuvant therapy, surgical treatment, and patient outcome differ between lower and higher rectal tumors, with lower rectal tumors being associated with a higher local recurrence rate and worse survival.1,2,4–8
In the literature, no consensus exists on the preferred method to determine rectal tumor height. In addition, data on the interchangeability of flexible endoscopy and MRI in determining rectal tumor height are lacking. Major trials on rectal cancer did not use a uniform definition of rectal tumor height, particularly regarding the distal end of the rectal tumor.4,9–11 Universal adoption of a standardized technique for assessment of rectal tumor height would likely facilitate comparison of study results of rectal cancer treatment.
Given the varying landmarks for defining rectal tumor height and their repercussions on treatment management and outcome, the primary aim of this study was to compare colonoscopy and MRI for determining rectal tumor height. Since there is no consensus on what method should be used for determining the rectal tumor height, we aimed to select the best method to improve standardized reporting of rectal tumors.
Patients and methods
Patient selection and database
Data of all patients with pathologically confirmed rectal carcinoma at a large urban teaching hospital between January 2002 and January 2012 were extracted from the Netherlands Cancer Registry. All patients with available MRI data and complete endoscopy reports (with tumor height) were included. This study was approved by the medical ethics research committee under registration number W13.018.
Endoscopy
Endoscopy reports of all patients were reviewed. Patients were included only if an exact rectal tumor height was mentioned in the endoscopy report. Since endoscopy was always performed before MRI, endoscopic tumor height data were independent from MRI results. To obtain insight in the techniques used for the endoscopic determination of rectal tumor height, a survey among regional endoscopists was conducted.
MRI protocol and measurements
Since 2006, MRI was added in our center as standard procedure for staging rectal cancer. Images of the lower pelvis were obtained using a 1.5 T MRI scanner (Philips Medical Systems International BV, Best, The Netherlands). Standard MRI protocol consisted of T2-weighted sequences in three planes perpendicular to the rectal wall at the level of the rectal mass, an axial T1-weighted sequence, and diffusion-weighted imaging. Two abdominal radiologists reviewed in consensus all MRI studies for assessment of rectal tumor height. Both radiologists were blinded to endoscopy results. The sagittal T2-weighted sequence was used to determine the shortest distance in centimeters between the ARJ to the lower pole of the rectal tumor. The ARJ was identified as the transition from the puborectal complex (low signal on T2-weighted sequence) and the rectal wall (intermediate signal on T2-weighted sequence).3,12
To assess the reproducibility of MRI-defined tumor height, we performed an interobserver agreement analysis between reassessed rectal tumor heights and those mentioned in the initial reports. Also, intraobserver agreement analysis was performed one year after the MRI measurements by both radiologists in consensus in a randomly chosen group of 20 MRIs, blinded to the initial rectal tumor height results and endoscopy results.
Statistical analysis
Data were analyzed using SPSS version 22 for Windows (SPSS Inc, Chicago, IL, USA). Means with standard deviation (SD) and ranges were calculated. Differences between MRI and endoscopy were tested using a paired T-test. Agreement between the measurements was tested using intraclass correlation coefficient (ICC) (two-way mixed, consistency, single measures) and Bland-Altman analysis. 13 Inter- and intraobserver variability was assessed using ICC. 14 ICC values ≥0.75 were considered as excellent agreement, 0.4–0.75 as fair to good agreement, and <0.4 as poor agreement. 14
Subsequently, data were stratified into three groups, with rectal tumor location classified as low from 0 to 5 cm, as middle from 5.1 cm to 10 cm, and as high from 10.1 cm to 15 cm, with respect to the ARJ. Lesions with rectal tumor height more than 15 cm from the ARJ were defined as sigmoid tumors. Differences between the MRI and endoscopy groups were tested using a McNemar test. A p value of <0.05 was considered statistically significant.
Results
Patient characteristics
During the study period, a total of 513 patients with pathologically confirmed rectal carcinoma were identified, of whom 265 patients (51.7%) underwent MRI as part of the preoperative work-up. Of these, 54 patients were excluded because of incomplete (n = 9) or no (n = 45) endoscopy report available for review. The final study cohort consisted of 211 patients (41.1%), of whom 60.2% were male. Mean age was 65 years (range, 36–91). Clinical stage of included patients was stage I, 11.8%; stage II, 8.1%; stage III, 57.8%, and stage IV, 22.3%. A flowchart of patient selection is shown in Figure 1.
Flow diagram of patient selection.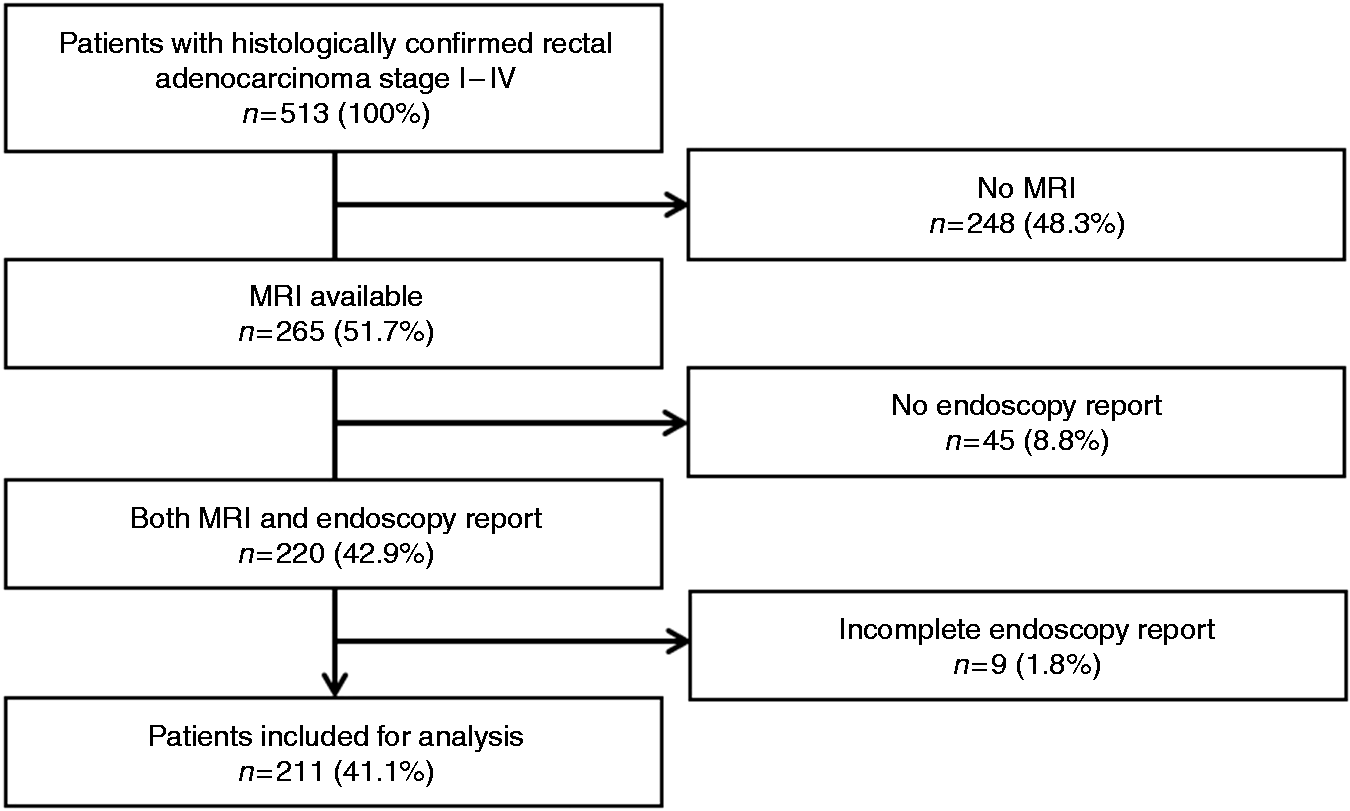
Endoscopy results
Mean rectal tumor height of 211 patients measured by endoscopy was 6.7 cm (±SD 4.4 cm, range 0–15 cm).
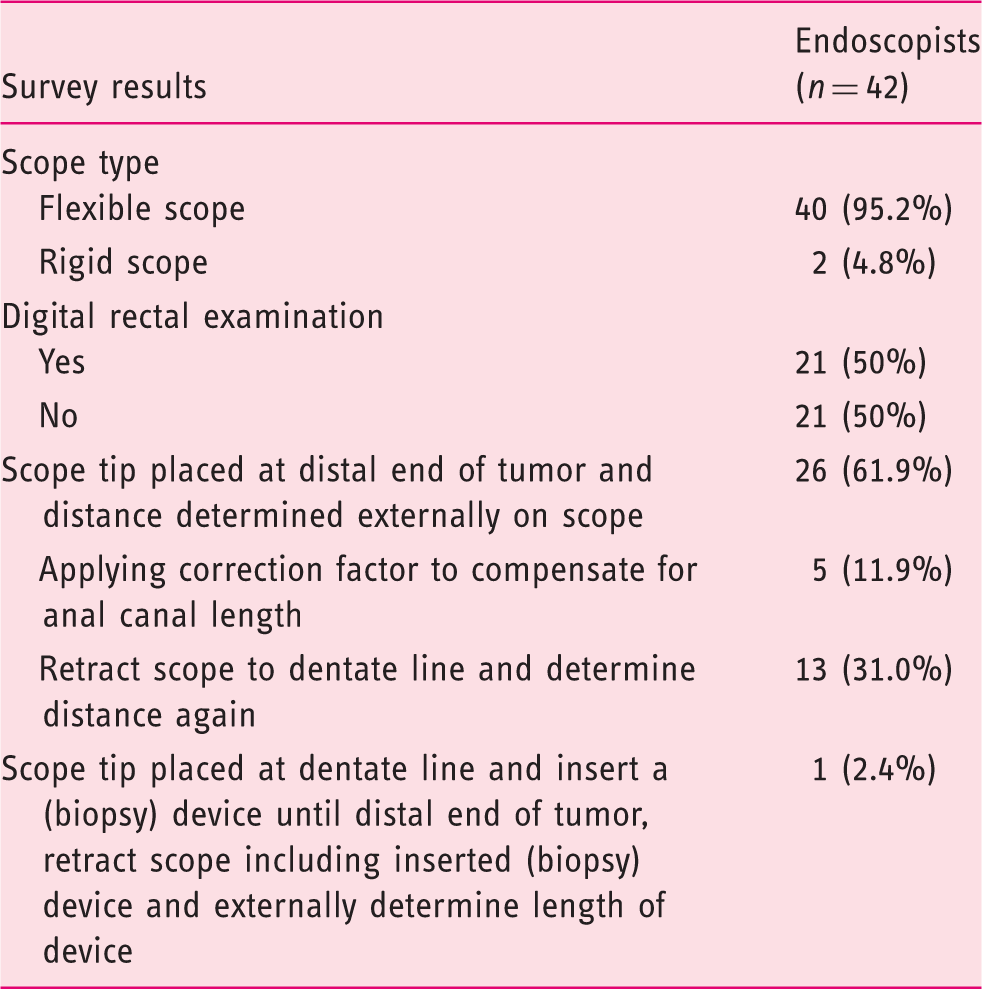
Survey results
Survey results
MRI results
The mean rectal tumor height of 211 patients measured by MRI after reassessment was 4.2 cm (±SD 3.3 cm, range 0–15 cm). All tumors were detected by both radiologists. In only 80 of 211 initial reports (37.9%) was an exact rectal tumor height mentioned. The remainder of 131 reports did not mention tumor height and the majority of these were dated before 2010 (74%). The mean rectal tumor height of these 80 patients was 4.8 cm (±SD 4.0 cm, range 0–15 cm). This was slightly higher than the reassessed mean rectal tumor height of these 80 patients (3.9 cm (±SD 3.6 cm, range 0–15 cm)) with a mean difference of 0.9 cm (95% confidence interval (CI): 0.4–1.4, p < 0.001). The distribution of tumor stages and locations was: T1 n = 16 (22%), T2 n = 16 (22%), T3 n = 22 (30%) and T4 n = 19 (26%), respectively, “low” n = 51 (64%), “middle” n = 24 (30%) and “high” n = 5 (6%). The interobserver agreement was excellent (ICC 0.8 (95% CI: 0.7–0.9), Figure 2(a)).
(a) Relation between reassessed magnetic resonance imaging (MRI) tumor heights and tumor heights mentioned in initial MRI reports (n = 80). X-axis depicts reassessed MRI tumor heights (cm), Y-axis depicts tumor height mentioned in initial MRI reports (cm). (b) Relation between MRI tumor height measurements and MRI tumor heights measured one year later by both radiologists (n = 20). X-axis depicts MRI measurements (cm), Y-axis depicts MRI measurements one year later (cm).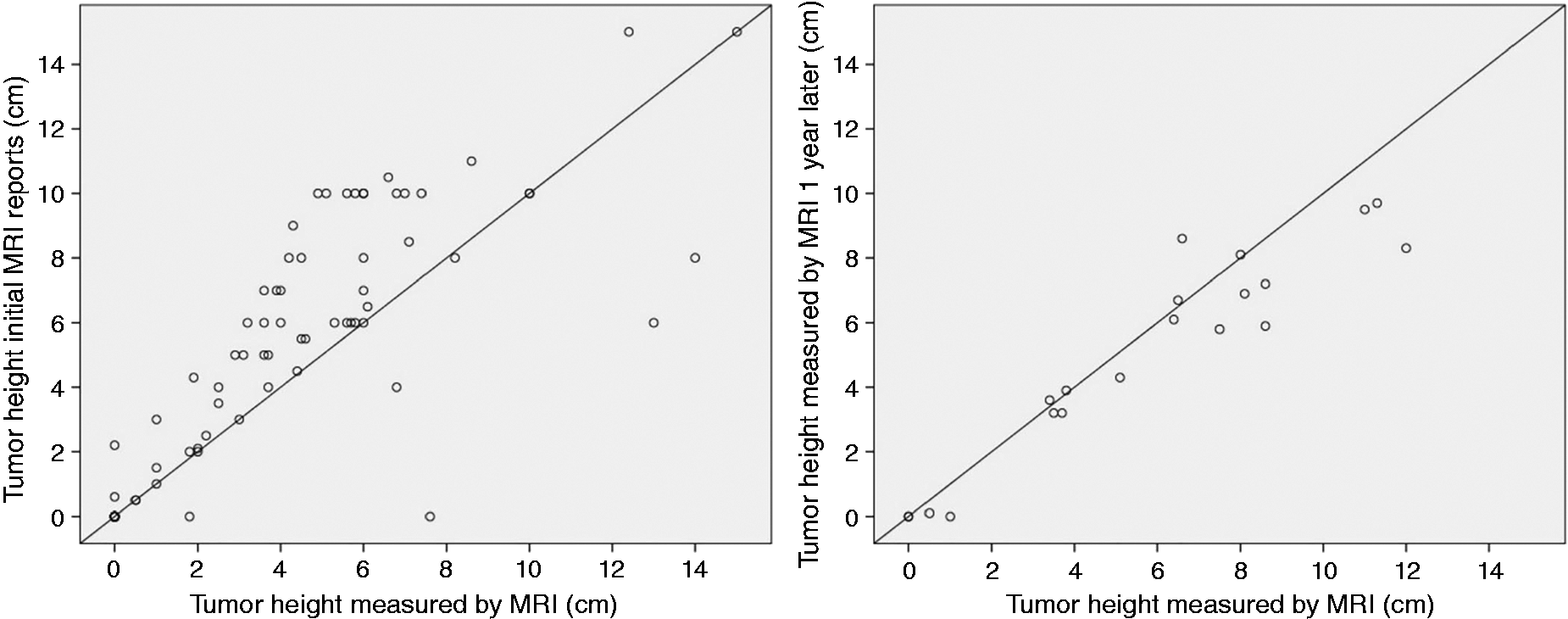
Review of 20 MRIs one year later by both radiologists resulted in a mean rectal tumor height of 5.1 cm (±SD 3.2 cm, range 0–15 cm). This was slightly lower than the initial rectal tumor heights (5.8 cm (±SD 3.7 cm, range 0–15 cm)) with a mean difference of 0.7 cm (95% CI: 0.2–1.3, p = 0.015). The distribution of tumor stages and locations was: T1 n = 4 (20%), T2 n = 6 (30%), T3 n = 7 (35%) and T4 n = 2 (10%), one missing data (5%), respectively, “low” n = 8 (40%), “middle” n = 9 (45%) and “high” n = 3 (15%). The intraobserver agreement was excellent (ICC 0.9 (95% CI: 0.9–1.0), Figure 2(b)). There was no significant difference in agreement between the group of 80 patients and the group of 20 patients (p = 0.51).
Rectal tumor height and correlation between MRI and endoscopy
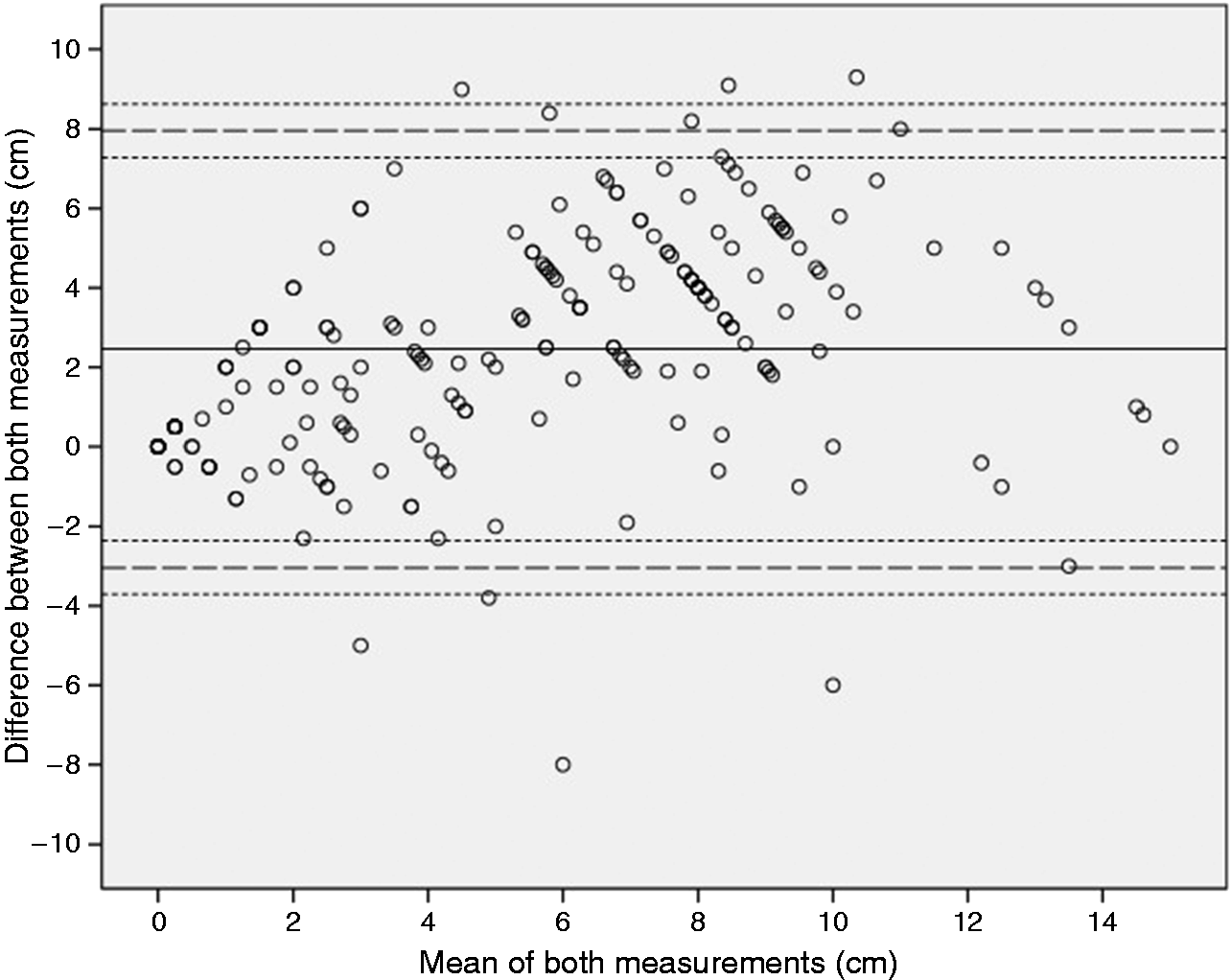
Rectal tumor height was significantly lower when assessed by MRI than by endoscopy, with a mean difference of 2.5 cm (95% CI: 2.1–2.8, p < 0.001). The agreement between rectal tumor height measured by MRI and endoscopy was good (ICC 0.7 (95% CI: 0.7–0.8), Figure 3). However, the 95% limits of agreement between endoscopy and MRI measurements varied from –3.0 cm (95% CI: –3.7 to –2.4) to 8.0 cm (95% CI: 7.3 to 8.6). Figure 4 shows the Bland-Altman plot with mean differences and limits of agreement, clearly showing large variability between endoscopy and MRI measurements.
Relation between endoscopic and magnetic resonance imaging (MRI) tumor height measurements (n = 211). X-axis depicts endoscopy measurements (cm), Y-axis depicts MRI measurements (cm). Bland-Altman plot of difference in measurements of tumor height using endoscopy and magnetic resonance imaging. Differences between measurements are given in centimeters. Reference interval given 95% limits of agreement (dashed lines) and their corresponding 95% confidence interval (dotted lines).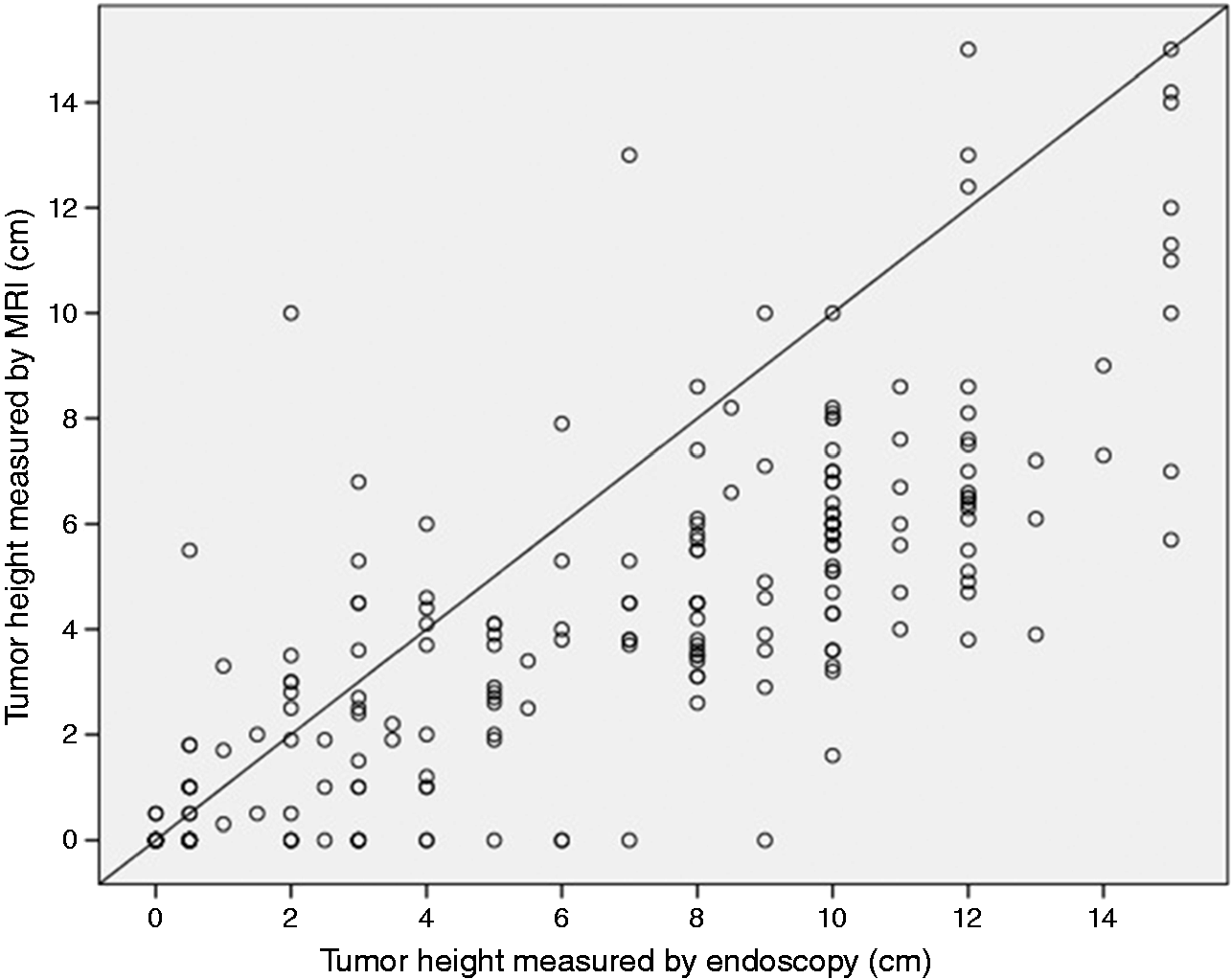
Tumor distribution
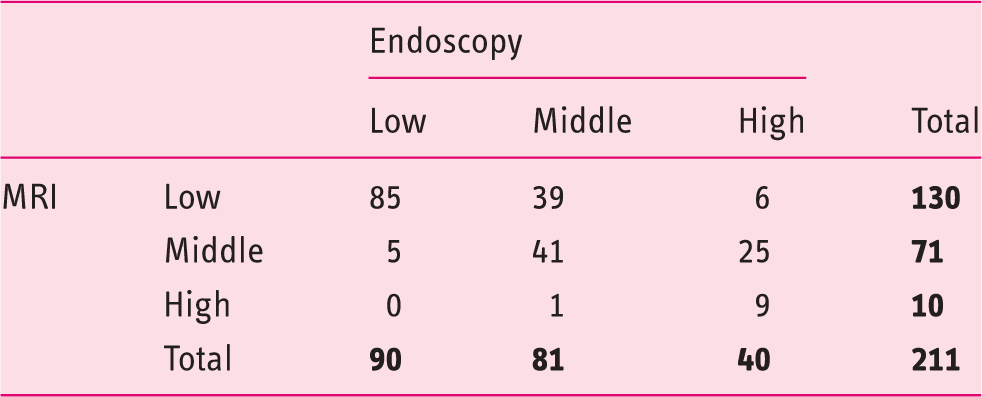
Tumor distribution in groups as measured by magnetic resonance imaging (MRI) and endoscopy
Discussion
The main finding of this study is that measurement of rectal tumor height is significantly lower (2.5 cm) when assessed by MRI compared with flexible endoscopy. Although the ICC was good (0.7), the wide 95% limits of agreement (–3.0 cm to 8.0 cm) show a large variability between both measurements. Furthermore, the Bland-Altman analysis showed that no standard correction factor can be applied to account for the discrepant measurements. Our study revealed that a significant proportion of rectal tumors were endoscopically classified as middle–high but as low by MRI assessment. This may result in considerable consequences for patient management and surgical decision making.
The results of our survey among regional endoscopists confirmed that no consensus exists concerning the determination of rectal tumor height by endoscopy. We found that endoscopists use various ways to technically measure rectal tumor height. Obviously, these measurements are subjective and not easily reproducible. Although rigid sigmoidoscopy is recommended by international clinical guidelines in determining rectal tumor height, only 2% of the responders indeed use both rigid sigmoidoscopy and flexible endoscopy. Importantly, flexible and rigid proctosigmoidoscopy for determining rectal tumor height are not interchangeable according to Schoellhammer et al. Their study showed that treatment options changed significantly in 25% of rectal cancer patients. Consequently, some patients with colon cancer in whom the tumor is incorrectly localized in the rectum, may be overtreated with neoadjuvant chemoradiation, while others may have benefited from neoadjuvant chemoradiation before resection. 15 Three previous retrospective studies have compared rigid proctosigmoidoscopy with MRI-defined tumor height. These studies concluded that measurements by both techniques indeed differ significantly and are not interchangeable.16–18 Only one small study by Paparo et al., including 66 patients, concluded that MRI measurements of rectal tumor height correlated well with rigid proctosigmoidoscopy. These authors used the anal verge as a landmark and their levels of agreement were –15.7 cm to 4.7 cm, clearly showing a large variability between the measurements. 19 In regular clinical practice, flexible endoscopes are used that may bend and thereby add a few centimeters to the true distance. Furthermore, the distance hallmarks on the endoscopes are spaced 5 cm apart, which may lead to mistakes in measuring distances. Finally, determining rectal tumor height by endoscopy is subjective and not easily repeatable.
In the radiologic literature, there is consensus on the best method to measure rectal tumor height at MRI by using the ARJ as a referencing landmark. 3 In our study, the inter- and intraobserver agreement in determining rectal tumor height at MRI was excellent. Moreover, in contrast to endoscopy measurements, MRI measurements are easily repeated, reproducible, and verifiable during multidisciplinary tumor board meetings.
As aforementioned, the use of different landmarks has considerable implications, because distally located rectal tumors are treated differently and carry worse prognosis.4–8 Depending on tumor stage, low rectal tumors may be treated by neoadjuvant radiotherapy because of the small distance to the mesorectal fascia. 1 When a tumor is wrongly diagnosed as middle–high at endoscopy instead of low by MRI, the opportunity of transanal endoscopic microsurgery is missed. 2 Also, the surgical decision between a low anterior resection and an abdominoperineal resection is location dependent. 2 Moreover, low rectal tumors carry an increased risk of postoperative complications and local tumor recurrence, resulting in worse survival.4–8 Although international clinical guidelines recommend the anal verge as a landmark, determination of the anal verge or dentate line is subjective and dependent on the experience of the endoscopist. Consequently, surgeons favor the use of the ARJ—the landmark used by radiologists—as this represents the distal border of perirectal fat in the mesorectum, which is important to ensure a free resection margin to the mesorectal fascia.
Our study has some strengths. To our knowledge this is the first study comparing colonoscopy and MRI in determining rectal tumor height.16–18 Our study was sufficiently powered to detect differences between MRI and endoscopy. Furthermore, all MRI studies were reviewed for the study purpose and assessment was performed systematically and standardized for determining the ARJ and rectal tumor height.3,12
The main limitation of this study is the retrospective design. Patient data were extracted from the database alone. Potentially relevant information not included in the database could have been missed. Also, the effect of intraobserver bias in the endoscopic measurements could not be studied, e.g. potential differences in measurement may depend on the experience of the endoscopist.
In conclusion, this study showed that MRI and colonoscopy differ considerably in determining rectal tumor height. A significant proportion of rectal tumors are endoscopically classified as middle–high but low by MRI. This may lead to a less-effective treatment strategy in some patients. There is no consensus among endoscopists as to how to technically measure rectal tumor height, and the interobserver variability of endoscopically determined rectal tumor height is unknown. Conversely, measurement of rectal tumor height by MRI showed excellent inter- and intraobserver agreement. As opposed to landmarks used by endoscopists and those recommended by clinical practice guidelines, the MRI-defined ARJ is highly relevant for surgeons for optimal treatment planning. In line with radiological guidelines, we suggest using rectal tumor height as measured by MRI for diagnostic purposes and treatment allocation in patients with rectal cancer.
Footnotes
Acknowledgments
All authors declare that they have read and approved the final version of the manuscript and that they all participated in the design, execution, and analysis of this paper. This manuscript is not under publication or consideration for publication elsewhere.
Declaration of conflicting interests
None declared.
Ethics approval
This study was approved by the medical ethics research committee under registration number W13.018.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Informed consent
Not applicable. Since this study is retrospective and does not involve prospective enrollment of subjects no consent is required.