
Abstract
Background and aims
Predicting the clinical course of Crohn’s disease (CD) is relevant for treatment selection. Currently, such diagnostic tools are lacking. In a previous pilot study, morphometric tissue image analysis showed promise in predicting the clinical phenotype and need for surgery. In this study, we aimed to validate our previous results on a larger cohort.
Methods
Colonic biopsies from CD patients with colonic or ileocolonic disease and at least five years of post-biopsy clinical follow-up were analyzed. The results were used to predict post-biopsy clinical phenotypes and outcomes. Data analysis was performed using multivariate regression models, discriminant score (DS) computations and Neural Network (NNET).
Results
Multivariate analysis of morphometric variables differentiated between B1 and B2 phenotypes (sensitivity 81%, specificity 74%, accuracy on cross-validation 75%; area under the curve (AUC) of 0.74 (CI 0.6–0.84; NNET model sensitivity 87%, specificity 67% on the testing population)). Differentiation between B1 and B3 phenotypes was also possible (sensitivity 69%, specificity 76%, accuracy 70.5% on cross-validation; AUC 0.78 (CI 0.68–0.89); NNET model sensitivity 78%, specificity 77% on the testing population)). Differentiating between B2 and B3 phenotypes was not possible using morphometric variables. Multivariate analysis predicted surgery (sensitivity 67%, specificity 72.5%, accuracy 69%; AUC 0.72 (CI 0.61–0.82); NNET model sensitivity 80%, specificity 91% on the testing population)).
Conclusions
This study validates previous results and suggests that morphometric image analysis of early biopsies from Crohn’s colitis patients may contribute to the prediction of future outcomes such as clinical phenotype and surgery. Prospective validation on larger cohorts is still needed.
Keywords
Introduction
Crohn’s disease (CD) is characterized by chronic inflammation of the gastrointestinal tract. The inflammatory process is thought to result from an interaction between genetic background, environmental factors, the host immune system and the gut microflora.1,2 The clinical phenotype of CD can be classified into three main categories as previously described in detail. 3 B1 phenotype implies an inflammatory type disease without stricturing or penetrating complications. B2 phenotype is dominated by luminal stricture formation and B3 phenotype by penetrating complication such as fistulas and abscesses. Disease course and phenotype may change over the years and up to 80% of patients may develop disease complications.4,5 Histopathological findings are important tools in the diagnosis of CD. No findings are pathognomonic; however, some are considered highly suggestive when coupled with a likely clinical scenario, endoscopic findings and imaging results. 6
Current management of CD may include the use of early aggressive therapy with immunosuppressive, biological agents or a combination of both. This strategy may offer advantages by disease course modification,7–10 but entails significant short- and long-term complications such as increased risk of infections and malignancy.11–13 Balancing efficacy and risks is a major therapeutic challenge, which can be significantly assisted by the ability to predict disease course. Previously, multiple clinical, serological and genetic characteristics have been shown to correlate with disease phenotype and complications.14–22 However, despite these observations, to date, prediction of disease course and complications is suboptimal and presents a major medical need.
Morphometry is a quantitative field that investigates changes in shape, size, architectural complexity and orientation of objects. Several methods for extraction of morphological parameters from an object exist. These include length, angles, perimeter shape and distribution in the space. Architectural complexities are typically analyzed by fractal and lacunar geometry algorithms. 23 Morphometry has been used to predict lymph node metastasis, tumor progression and patient survival in squamous cell carcinoma of the vulva and renal cell carcinoma, and in the assessment of dysplasia and progression to adenocarcinoma in Barrett’s esophagus.23–26
In a previous pilot study, we were able to show that morphometric analysis may contribute to the prediction of the clinical phenotype and surgery in patients with Crohn’s colitis. 27 In the present study, we sought to further evaluate and validate the histomorphometric features of early colonic biopsies from patients with Crohn’s colitis and their relationship to evolving clinical phenotypes.
Methods
Patients
CD patients with colonic involvement were selected from our database according to clinical phenotypes as outlined in the Montreal classification. 3 Patients had either isolated colonic disease or a combination of small-bowel and colonic disease. We analyzed biopsies obtained at the first documented colonoscopy for each patient, which was around the time of diagnosis in the majority of cases. All patients had at least five years of post-biopsy follow-up. Clinical data were extracted from patient files and included the clinical phenotype, medical and surgical history. The clinical data were coded and subsequently analyzed and correlated with the histological findings. The observer who performed the morphometric analysis was completely blinded to the clinical variables and patient identity. The study was approved by the institutional review board.
Morphometric analysis
New slides were prepared from the original paraffin blocks. The histological stains included: hematoxylin and eosin (H&E) for diagnosis, confirmation and evaluation of the inflammatory cells type and numbers; pancytokeratin (CK) to highlight and quantify the mucosal crypts; and Mason-Tri-chrome (TC) and reticulin (RET) for the presence of mature and young collagen, respectively. Staining was performed according to standard procedures. Slides were scanned using the 2.1 Dotslide virtual microscopy system (Olympus, Germany and Japan). From each slide, three to four representative images were collected. The number of scanned fields and the magnification used were identical for all slides with each histological stain. The ImagePro plus 7.0 program (Media Cybernetics, USA) was used to analyze and quantify the collagen fibers, the inflammatory cells and the crypt architecture. The MATLAB program (MathWorks, USA) was used to analyze the fractal and lacunar dimensions and the orientation of the crypts in order to assess architectural complexity and distortions of the mucosal crypts. Figure 1 shows the morphometric analysis of different quantitative features in the colonic mucosa.
Examples of morphometric measurements. The left image in each pair represents the clean stained histological specimen whereas the right image displays the quantified variable during image analysis (1a + 1b: CK stain highlighting the crypts; 2a + 2b: CK stain negative highlights the inflammatory cells; 3a + 3b: reticulin stain highlighting young collagen; 4a + 4b: Mason TC stain highlighting mature collagen; 5a + 5b: image masking highlights the mucosal architecture). CK: pancytokeratin; TC: Tri-chrome.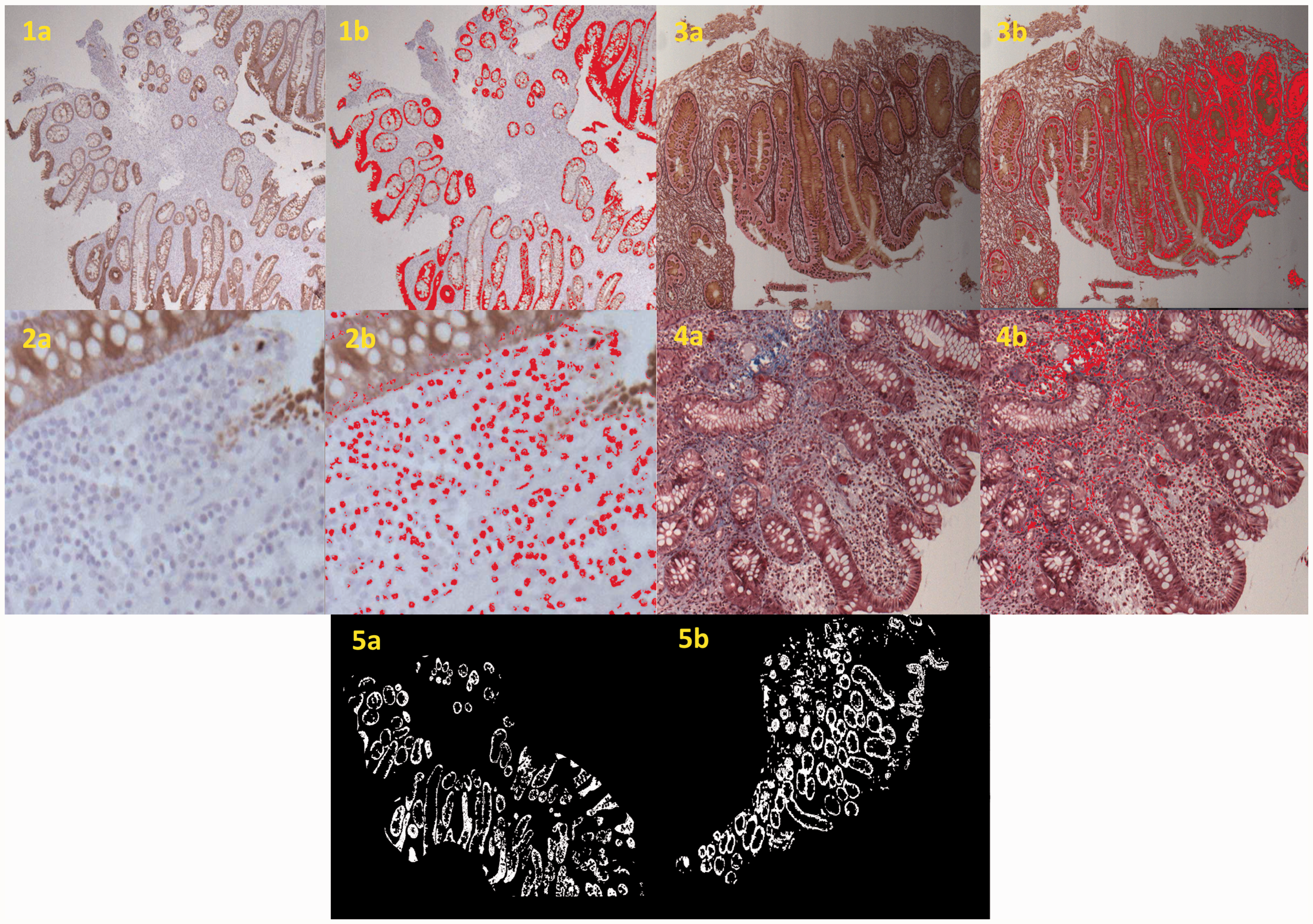
Statistical analysis
Univariate analysis was performed and morphometric variables associated with specific clinical characteristics and evolving clinical phenotype were identified. Variables identified as significant on univariate analysis were then used in a multivariate model (discriminant analysis) to adjust for confounding variables and to single out independent and significant predictors of disease phenotype. Validation of the results was obtained by using the “leave one out method.” Using the independent variables and their coefficients, discriminant scores (DS) were computed and receiver operating characteristic (ROC) analysis of the DS was calculated to obtain an area under the curve (AUC). In order to better handle the complexity and the large number of variables, a neural network (NNET) model with a feed forward architecture was trained using the morphometric variables data in order to develop a mathematical classifier that best predicts the clinical phenotypes. Our model used for function fitting a two-layer feed forward network with a sigmoid transfer function both in the hidden and the output layers. The output data consisted of the patients’ clinical phenotype. We used 50%–70% of the cases as the training population for our model, and 30%–50% of the cases as the testing population. Statistical analysis was performed with SPSS version 23 (SPSS Inc, Chicago, IL, USA).
Results
Patients
Patient characteristics.
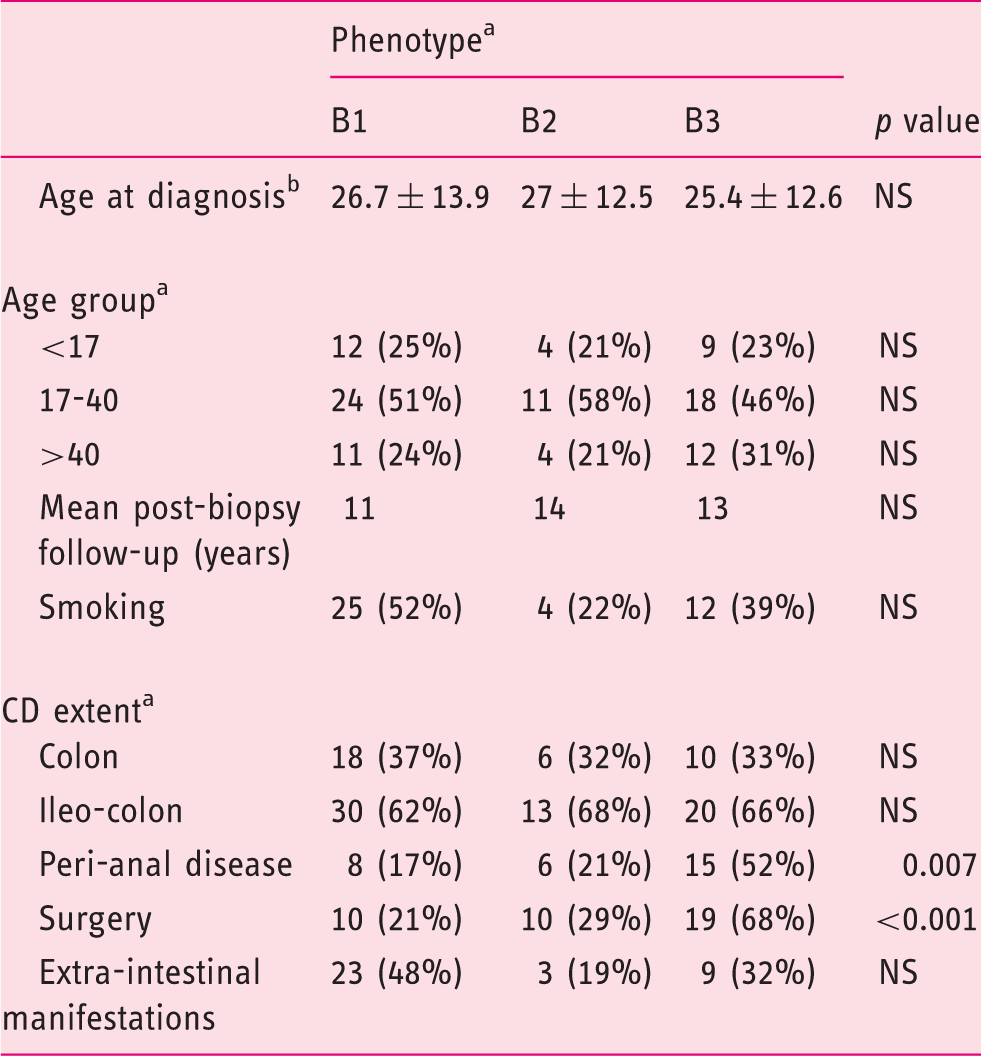
According to Montreal classification. bMean ± standard deviation. CD: Crohn’s disease.
Morphometry and its correlation to clinical variables and disease phenotypes
Association between morphometric variables and specific clinical characteristics of the cohort.
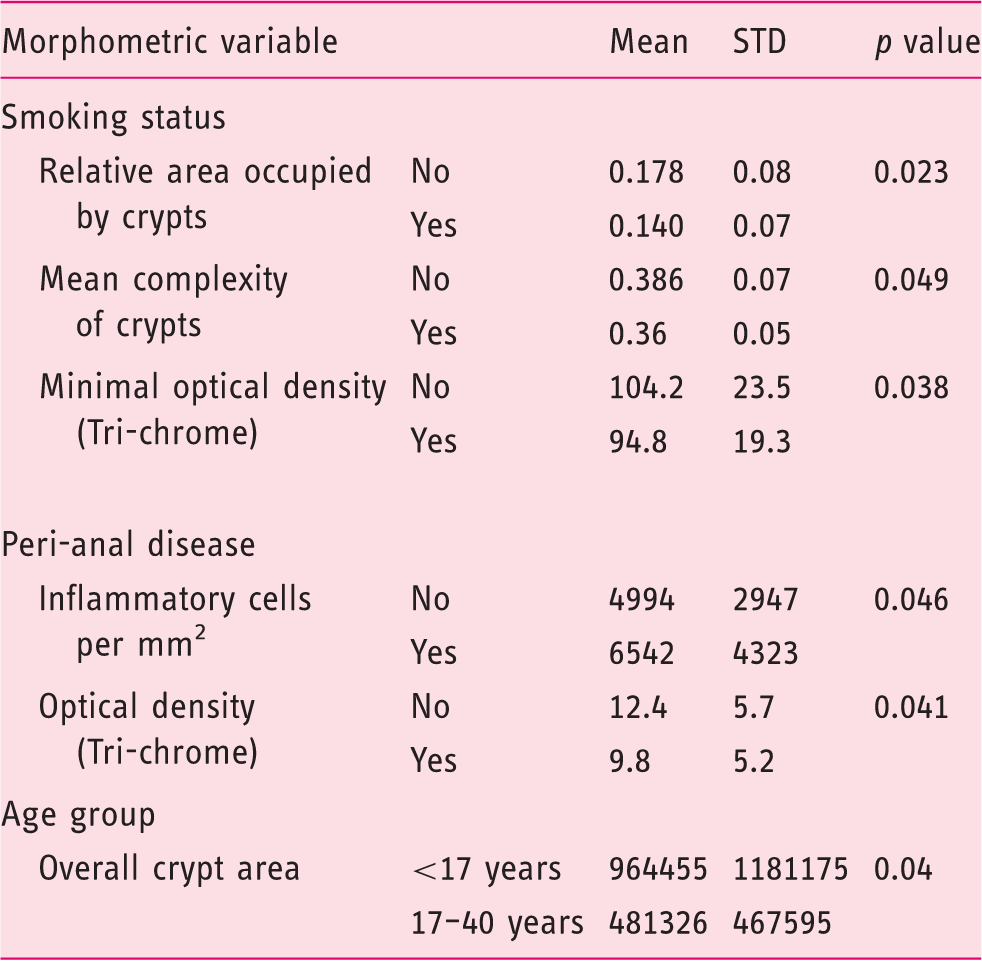
STD: standard deviation.
Univariate analysis of the correlation between morphometric variables and the evolving clinical phenotypes.
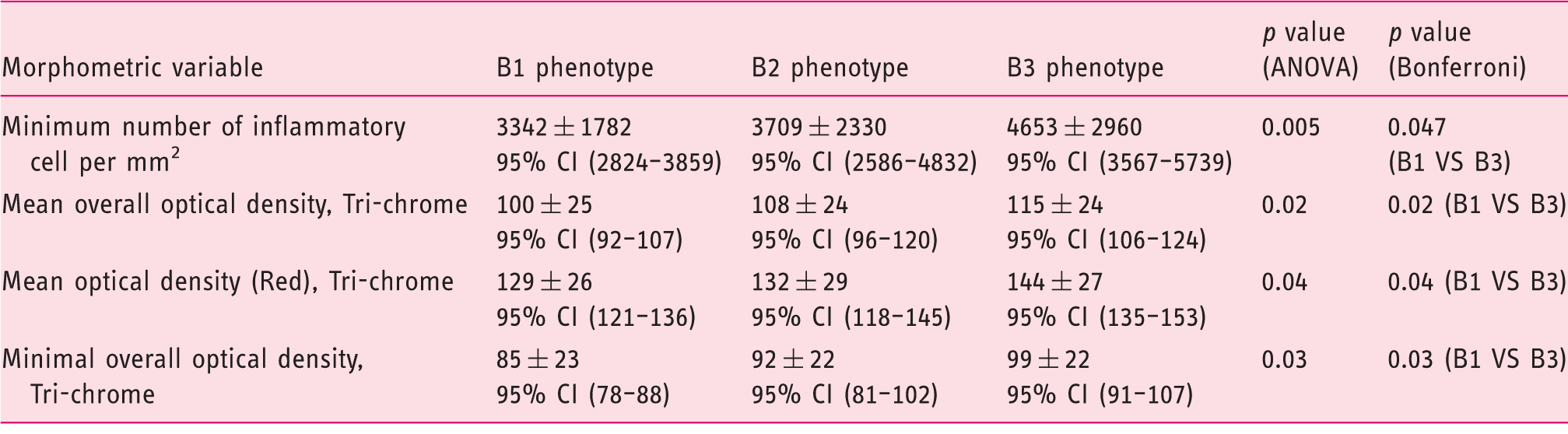
Values are mean ± standard deviation. ANOVA: analysis of variance; CI: confidence interval.
Independent predictors found in multivariate analysis for distinguishing between disease phenotypes and the need for surgery.
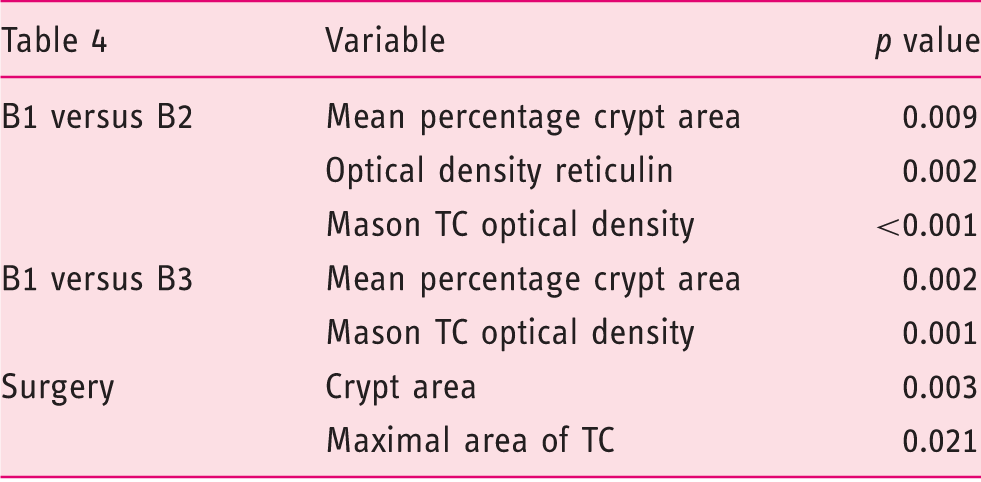
TC: Mason Tri-chrome.
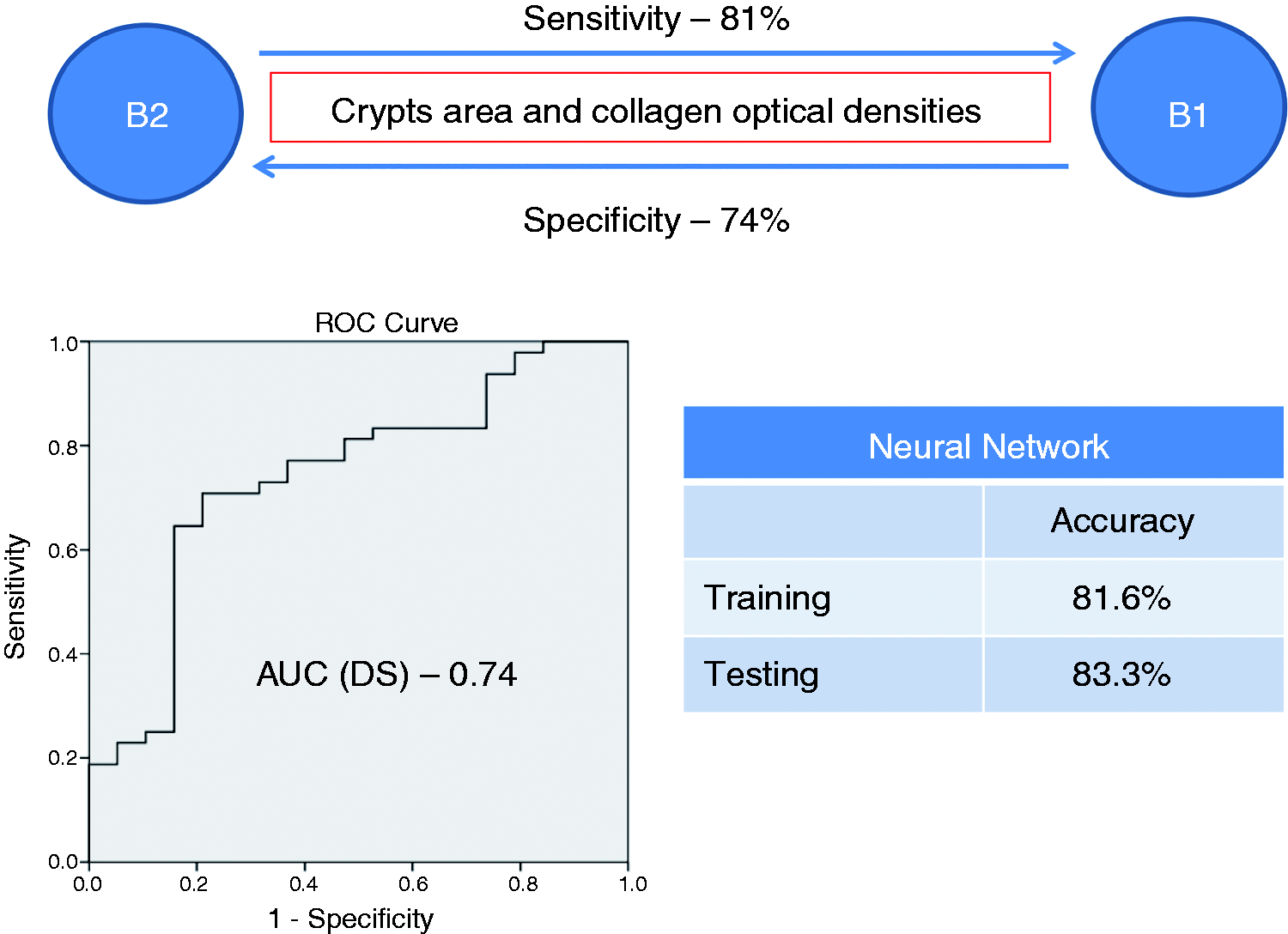
A schematic presentation of multivariate analysis and NNET model for predicting between B1 and B2 phenotypes. NNET: neural network; AUC: area under the curve; DS: discriminant score.
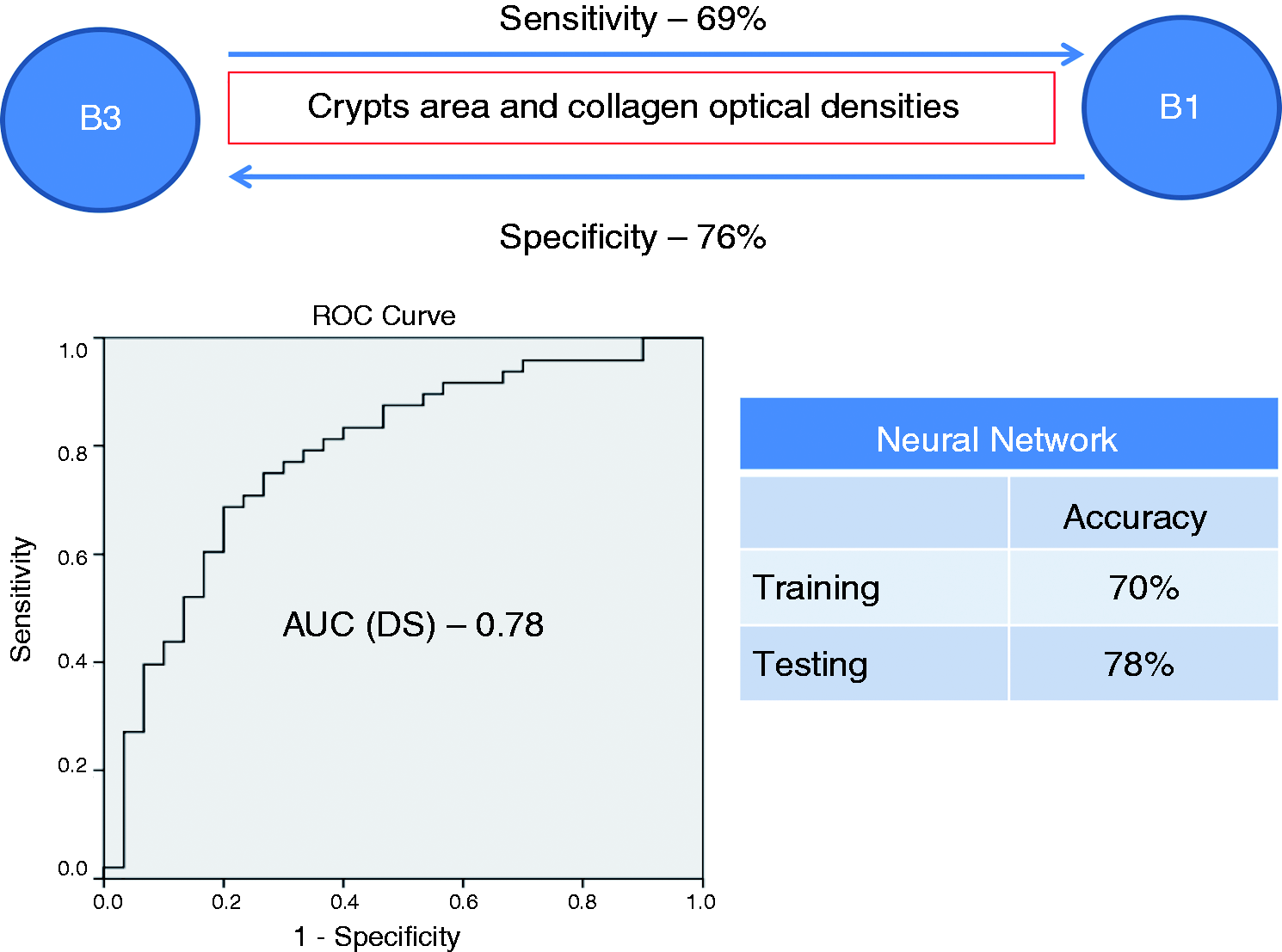
A schematic presentation of multivariate analysis and NNET model for predicting between B1 and B3 phenotypes. NNET: neural network; AUC: area under the curve; DS: discriminant score.
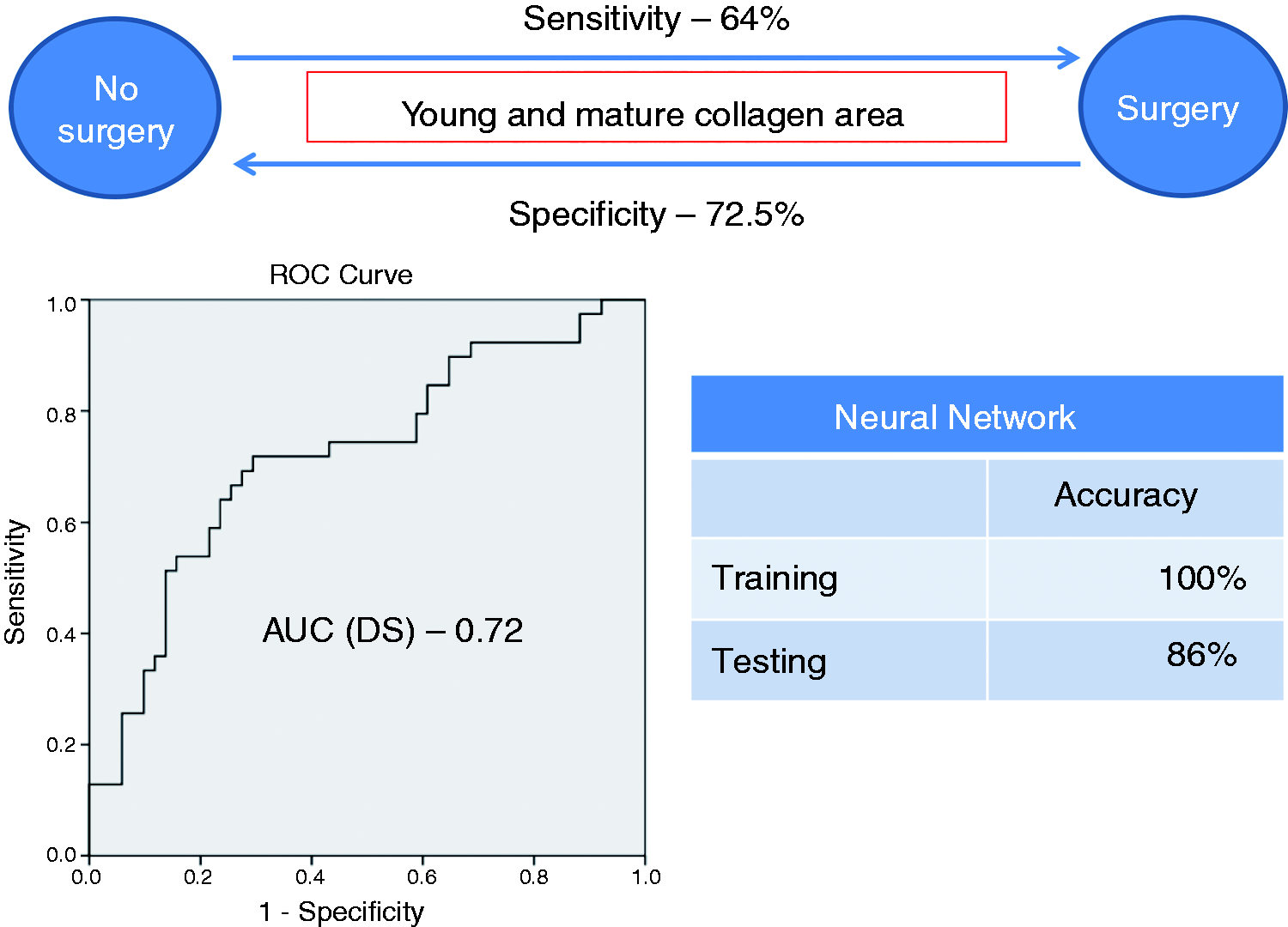
A schematic presentation of multivariate analysis and NNET model for predicting the need for surgery. NNET: neural network; AUC: area under the curve; DS: discriminant score.
Discussion
The present study describes the use of morphometric analysis for quantitative measurements of various elements in endoscopic colonic biopsies in order to evaluate their associations and potential role in predicting disease course and complications.
We found an association between smoking and crypt size and complexity and level of collagen optical density. This observation implies that smoking may have an effect on tissue inflammation and fibrosis early in the disease course. An association was also seen between the presence of peri-anal disease and the amount of inflammatory cells and levels of collagen optical density. This is very interesting as both smoking and peri-anal disease have been shown to be associated with more severe disease and inflammation.21,22 Further research into this area and the potential molecular mechanisms behind these phenomena is needed.
Currently, prediction of disease phenotype is suboptimal. Genetic factors such as NOD2 mutations are associated with a fibro-stenosing phenotype and an increased need for surgery. 14 However, genetic variables, naturally available upon diagnosis, are useful in only approximately one-third of patients, and are even less relevant in certain geographical areas. A prominent example of this limitation is the low prevalence of NOD2/CARD15 mutations in the eastern Asian CD patient population as compared to Western populations. 28 Serology may be an additional useful tool. Antibodies to anti-Saccharomyces cerevisiae antibodies (ASCA) and anti-CBIRL (anti-flagelin) are associated with small-bowel and penetrating disease, respectively.15–17 Antibodies to perinuclear anti-neutrophil cytoplasmatic antibodies (pANCA) correlate with an ulcerative colitis (UC)-like disease. 18 Furthermore, multiple positive serologies are associated with propensity for disease complications.19,20 However, although serological findings may be present at least to some extent at diagnosis, only limited data are available regarding the association of serology at early disease stages and late outcomes.29,30 Clinical characteristics such as cigarette smoking, early use of steroid and the presence of peri-anal disease have also been shown to be suggestive of a complicated disease course.21,22 However, despite these observations, to date, prediction of disease course and complications is suboptimal and presents a major medical need. In this study, several morphometric variables emerged as significant for prediction of disease phenotype and the need for surgery in the multivariate analysis and NNET model (crypts and collagen optical densities for comparison between B1 and B2 phenotypes; crypts and collagen area and optical densities for comparison between B1 and B3 phenotypes; collagen area for prediction of surgery). Using two different mathematical models provided an adequate validation of the potential predictive ability of morphometry in this cohort. These observations, in combination with known predictors, may enhance our ability to predict disease course and complications.
We recognize this study’s limitations: Firstly, this was a retrospective study of a small group of patients. A small number of patients in our cohort (four) received 5ASA or steroid therapy prior to biopsy, which theoretically could have influenced the histological findings. However, since this is a minority, we believe it did not significantly influence the average result of the different variable for each phenotype group. Validation of our results using additional, larger blinded cohorts and eventually in a bona fide prospective manner is needed. Secondly, we examined biopsies from patient with colonic CD involvement and did not include small-bowel biopsies. In addition, some patients had isolated colonic disease whereas others within our cohort had a combination of colonic and small-bowel disease, which may already confer a different clinical phenotype. We did not have detailed information regarding patients’ past complications (i.e. stricture location and extent, or nature of penetrating complications). However, since complicated disease can occur both in the small bowel and the colon, we felt these patients could be grouped into one cohort. Patients with isolated colonic disease represent only 25%–50% of CD patients, and further studies are needed in order to characterize and quantify the histological findings in other gastrointestinal segments in patients with combined small-bowel and colonic disease and in patients with isolated small-bowel disease.
In conclusion, this study validates our preliminary results that quantitative morphometric data may enable differentiation and prediction of clinical phenotypes and outcomes such as surgery. Because histological sampling is almost universally used in the workup of CD patients, this novel approach may be combined with other biologic variables and clinical predictors to significantly increase the ability to classify and predict the clinical course of CD colitis patients, thus improving their management. Prospective validation on larger cohorts is still needed.
Footnotes
Declaration of conflicting interests
Yehuda Chowers is a member of the Rambam Committee of Interns and Residents (CIR) and has served as a consultant and received lecture fees from Abbott, Schering Plough, Janssen and Takeda.
Funding
This work was supported by the departments of Gastroenterology and Pathology at the Rambam Health Care Campus.