
Abstract
Background
Self-expandable metal stents (SEMSs) are the main palliative modality used in inoperable oesophageal cancer. Other palliative modalities, including argon plasma coagulation (APC), have also been used.
Objective
The purpose of this study was to assess the relative efficacy of SEMS and APC regarding the survival of patients with inoperable oesophageal cancer, not receiving chemo/radiotherapy.
Methods
Single centre, retrospective analysis of all patients (n = 228) with inoperable oesophageal cancer between January 2000 and July 2014, not receiving chemo-radiotherapy, treated with SEMS (n = 160) or APC (n = 68) as primary palliation modalities. Cox regression analysis was performed to identify individual factors affecting survival and Kaplan–Meier curves were created for patients treated with APC and SEMS for stage III and IV disease. Survival intervals were compared by the log-rank test.
Results
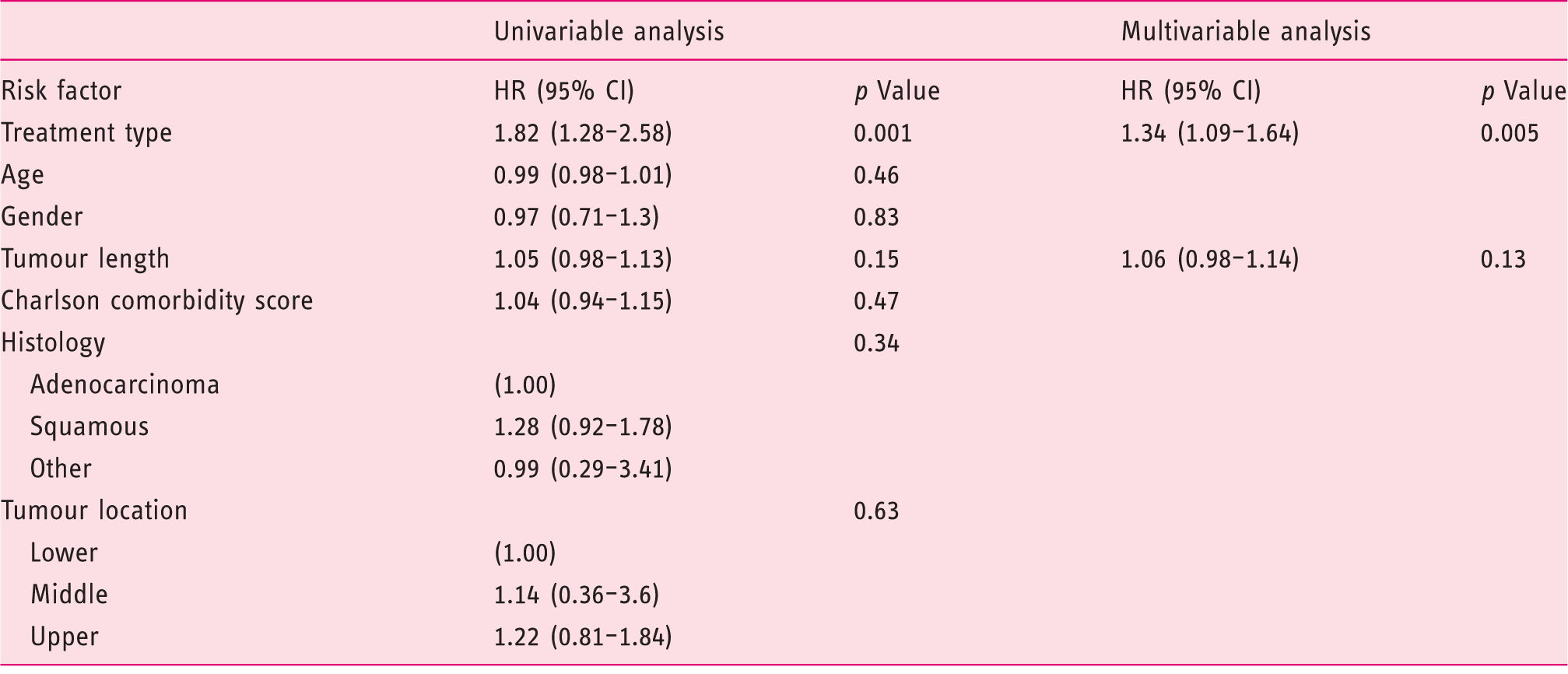
Type of treatment was the only statistically significant factor affecting survival, after disease stage stratification (hazard ratio (HR): 1.36, 95% confidence interval (CI): 1.13–1.65 of SEMS over APC, p: 0.002). Median survival for patients treated with APC and SEMS was 257 (interquartile range (IQR): 414, 124) and 151 (IQR: 241, 61) days respectively in stage III disease. It was 135 (IQR: 238, 43) and 70 (IQR: 148, 32) days respectively in stage IV disease. Both differences were statistically significant (p = 0.02 and 0.05 respectively).
Conclusions
APC is a promising palliation modality in inoperable oesophageal cancer, when patients are not candidates for chemo-radiotherapy. A randomized controlled trial will be needed to confirm those results.
Introduction
The crude incidence of oesophageal cancer in the European Union is 4.5 cases/105/year and the mortality is 3.5/105/year. 1 Even after complete tumour resection the long-term survival in localized disease with lymph node involvement does not exceed 25%. In extensive disease the combination of surgery with other treatment modalities is a standard approach, but complete tumour resection is not possible in 30–50% of primary tumour stage T3 or T4 (pT3-T4) pT3-T4 cases. 1 The best palliative treatment for patients with inoperable oesophageal cancer has not yet been established. Treatment options most commonly used for palliation include self expandable metal stent (SEMS) placement,2–4 thermal ablative techniques (laser, argon plasma coagulation (APC)),5,6 external beam radiation in combination with brachytherapy, 7 brachytherapy as a single treatment 8 and chemotherapy. 9 In many cases combination of palliative treatments are implemented. Although SEMSs have no direct antitumour activity, they are thought to extend the survival of symptomatic inoperable patients by improving nutritional intake and preventing starvation, dehydration, and aspiration. Other studies confirmed the effectiveness of APC as palliative treatment in oesophageal cancer, either alone10–12 or in combination with other modalities. 13
The relative effect of SEMS compared to APC on survival in patients with oesophageal cancer, who are not candidates for surgery or chemoradiotherapy, is unknown. In clinical practice, both modalities are available and in many cases they are both used in the same patients. The aim of this study was to compare the effectiveness of two different palliation strategies using either APC or SEMS as primary treatment, followed by the other as needed, on survival of patients with inoperable carcinoma of the oesophagus, not receiving other palliative treatments in the form of chemotherapy or radiotherapy.
Methods
Patient selection
This was a retrospective observational clinical study of consecutive patients with inoperable carcinoma of the oesophagus treated with SEMS or APC, conducted at a single centre over a 14-year period.
Patients referred for palliative treatment of oesophageal or oesophago-gastric junction cancers extending to the oesophagus were recruited. All had been assessed in a multidisciplinary team (MDT) meeting on upper gastrointestinal (GI) cancer, where it was agreed that surgery treatment was inappropriate because of locally advanced disease, metastases, severe comorbidity or a combination of these conditions. The decision-making process was based not on predefined variables but on consideration of multiple doctors’ opinions, and on an individual basis taking into account age, serum albumin, magnitude of weight loss, comorbidities and performance status. The endoscopic palliative treatment modality was decided on the basis of social circumstances and patient preferences after detailed discussion regarding each technique’s characteristics. Informed consent was obtained from all patients prior to the initiation of treatment.
All patients who were diagnosed with inoperable oesophageal or oesophago-gastric junction cancer (Siewert type I) between January 2000 and July 2014, and received either APC or SEMS were considered eligible for inclusion in this study. Patients who received chemotherapy or radiotherapy either before or after SEMS or APC were excluded. Patients intolerant to the initial chemotherapy treatment, not being able to conclude a cycle of therapy, were also included since a single dose of chemotherapy was not considered as significant to alter the outcome. Patients lost to follow-up or with incomplete staging or treatment data were excluded.
Computerized medical records dated between 2000 and 2014 were searched for patients meeting the inclusion criteria. Patient cases were identified using four different sources: hospital electronic records system (since 2004), the upper GI cancer MDT records, the electronic endoscopy reporting system and the South-East of Scotland Cancer network database. The following data were retrieved from the medical, pathology and endoscopy records as well as the death register: gender, age, date of diagnosis, date of first treatment, dates of subsequent treatments, date of death, tumour location, histology, staging and comorbidities. For the latter, the comorbidity component (Charlson Comorbidity Score (CCS)) of the Charlson Comorbidity Index (CCI) was used. Charlson Comorbidity Index (CCI) has been widely used and proved to be a reliable tool for use in trials of cancer patients. CCI score is consistently correlated with disease specific survival, overall survival, or treatment-related adverse events, confirming its predictive validity. After controlling for age, cancer stage, and type of treatment, increasing comorbidity remained significantly predictive of increased all-cause mortality 14 and, as is the case with other comorbidity indices, has been shown to be more predictive of disease outcome than single comorbid conditions. 15 For the purposes of this study, the score was calculated taking into consideration all the comorbidities known prior to the diagnosis of cancer. Therefore, patients without any other health problems apart from oesophageal cancer were assigned a CCS of zero.
Staging procedure
Staging was based on endoscopic findings, histology and imaging studies. CT scan of abdomen and thorax was performed in all patients, as well as an endoscopic ultrasound (EUS) until 2010. Since 2010, a positron emission tomography (PET) scan was also performed and the EUS was used in cases of uncertainty. Oesophago-gastric junction cancers extending to the oesophagus (Siewert type I) were categorized as lower oesophageal. The most recent edition (6th or 7th)16,17 of the American Joint Committee on Cancer (AJCC) Tumour-Node-Metastasis (TNM) classification for oesophageal cancer available at the date of diagnosis was used for each case.
Techniques
All endoscopic procedures were performed under conscious sedation with the use of midazolam for biopsies to confirm the diagnosis of cancer. When EUS was performed, staging was done with a variety of radial or linear echoendoscopes (Olympus Corporation, Japan). In general, oesophageal dilatation was avoided prior to MDT discussion and management decision.
APC
The APC treatment goal was tumour debulking and oesophageal lumen recanalization. Argon gas flow was set at 2 l/min and power at 40–65 W. Four different catheters were used; 2.3 mm axial beam catheters were used most commonly through standard scope channel, whereas those of 3.2 mm were used through a therapeutic endoscope for extensive tumour debulking. The side fire conical beam and the circumferential beam catheters were used on few occasions. Both forced and pulsed APC techniques were used as needed. During procedures, the gas produced was regularly aspired and coagulum from the tip of the probe was cleaned when necessary. The duration of each session was between 25 and 40 min. Initially patients were treated at 2–4 week intervals, until achieving lumen patency and symptom relief and then were regularly treated at 8–12 weeks intervals. Those intervals were subject to change according to tumour response and symptoms recurrence.
Oesophageal stents
For patients treated with stent placement a partially covered SEMS was used. SEMSs were available in lengths of 10, 12 and 15 cm with a proximal diameter of 23 mm and a distal diameter of 18 mm (Ultraflex, Boston Scientific, USA). The stent was introduced and deployed either by direct endoscopic monitoring or a combination of both endoscopic and fluoroscopic monitoring. When the latter was used, proximal tumour margin was identified and marked internally by injection of a radiographic contrast medium into the submucosa of the oesophageal wall through a sclerotherapy needle. After placement, deployment of the stent was assessed endoscopically and fluoroscopically.
Statistical analysis
The two treatment groups were compared with respect to base-line characteristics using the Mann–Whitney U test for continuous variables and the chi-square test for categorical variables. Analysis was based on intention-to-treat. Univariate analysis with Cox regression was performed for each of the patients’ characteristics in order to assess its potential association with survival. Analysis was stratified for disease stage. Variables found to be associated with survival in univariate analysis with p≤0.1 were included in a multivariate Cox regression analysis. Statistical significance was set at 0.05 for the variables to be retained in the multivariate model. Differences in survival were tested with life-table analysis using the Kaplan–Meier method. This was constructed by using the number of days between the first procedure and death. Survival intervals were compared by the log-rank test. Survival comparisons were performed separately for stage III and IV. Survival of patients still alive at the time of the analysis was censored. In order to minimize the effect of potential selection bias (i.e. allocating more frail patients preferentially to one type of treatment), survival comparisons were also performed after excluding patients surviving less than a month. A p value of <0.05 was considered significant. All analyses were performed with IBM SPSS Statistics version 21.0 (IBM Corp, Armonk, New York, USA).
Ethics consideration
This study was conducted in accordance with UK research ethics guidelines (http://ukrio.org). After review by the local ethics committee, further specific ethical review and approval were not required, as the study was considered as a retrospective clinical audit work using data already obtained as part of regular patient care.
Results
Between January 2000 and July 2014 a total of 388 patients received a diagnosis of inoperable oesophageal cancer and were treated with a palliative modality. A total of 160 patients were excluded. Of these 86 were excluded because they were initially treated with chemotherapy, radiotherapy or laser. Fifty patients (10 in APC group and 40 in SEMS group) were also excluded due to inadequate staging data. In those patients it was unclear whether the local invasion of the tumour could be classified as T2 or T3 and thus it was unclear whether they should be categorized as stage II or III. A further 24 patients were also excluded due to inadequate data regarding their treatment. The majority of those patients were referred to our centre by other hospitals in Scotland for stent placement and then returned to the referring sites, being lost from our follow-up. Of the remaining 228 patients, 68 were treated with APC as a primary modality and 160 were treated with SEMS. There were six out of 228 (2.6%) patients still alive at the end of follow-up, five of whom were treated with APC and one with SEMS. A flow chart describing the exclusion process, as well as the need for further endoscopic interventions, in addition to the initial modality used, is presented in Figure 1.
Flow chart describing the screening and exclusion process of patients with inoperable oesophageal cancer diagnosed between 2000 and 2014, as well as the type of initial treatment they received (APC or SEMS). Further types of treatments required are also presented for both the APC and SEMS groups. APC: argon plasma coagulation, SEMS: self-expandable metal stent.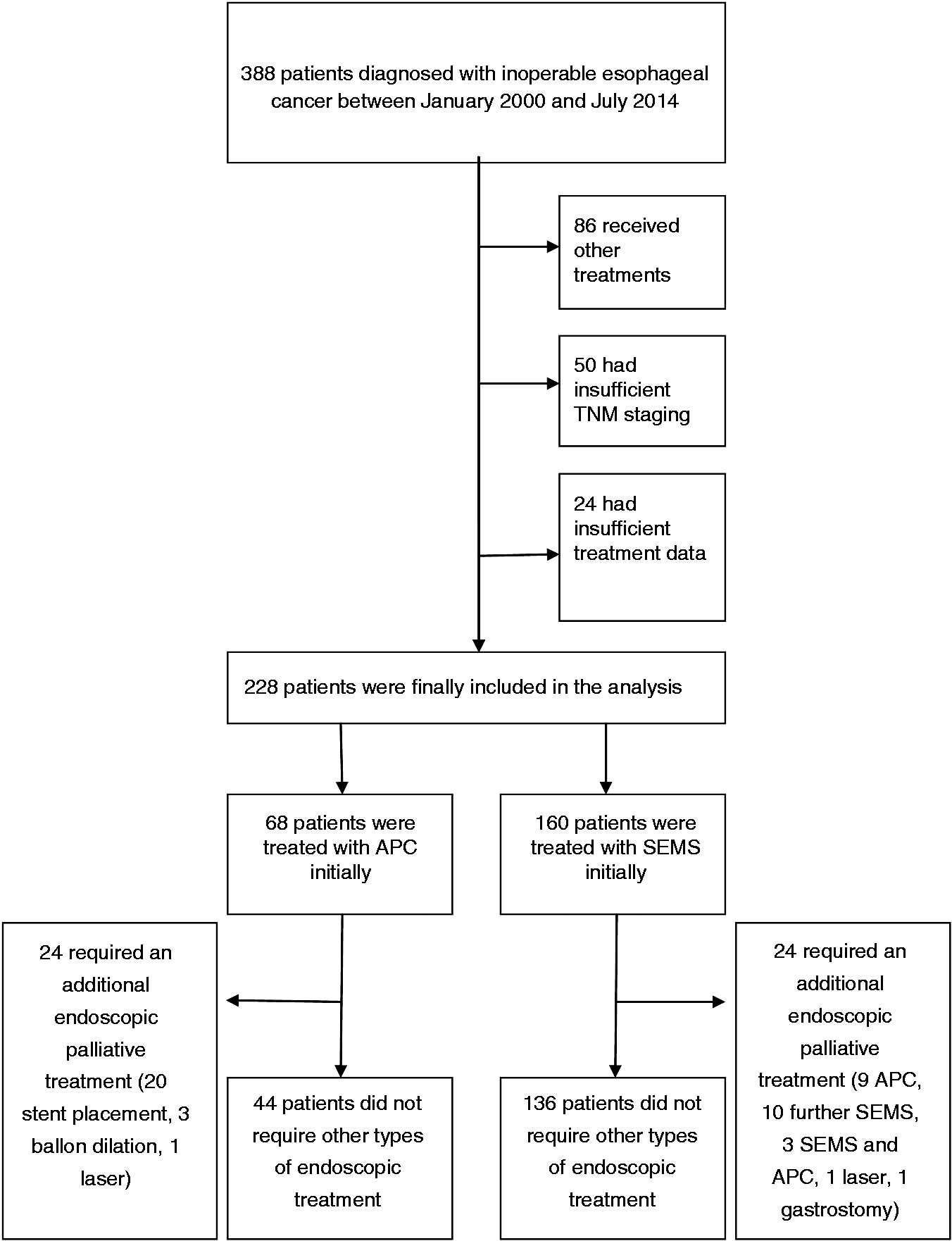
Baseline population characteristics in self-expandable metal stent (SEMS) and argon plasma coagulation (APC) treatment groups. Comparisons between groups were performed using the Mann–Whitney U test for continuous variables and chi-square test for categorical variables. Relevant p values are presented for each comparison
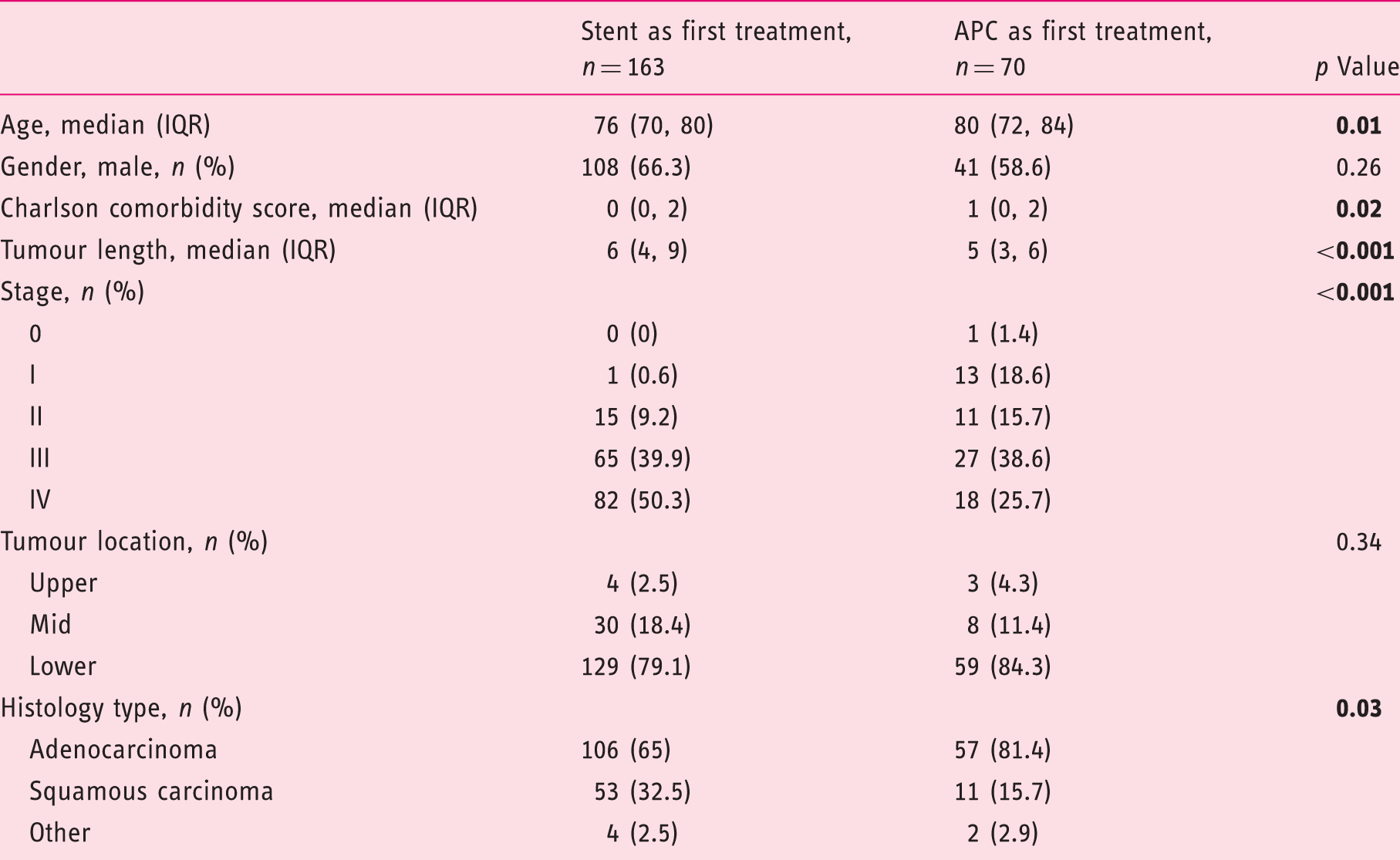
IQR: interquartile range.
In the APC group, a median of three (IQR: 2, 5) APC sessions were required to maintain lumen patency. In 44 (64.7%) of them, APC treatment was able to maintain patency until death or end of follow up period (July 2014) in surviving patients. Twenty-four of them (35.3%) required an additional endoscopic palliative treatment (20 stent placement, three balloon dilation, one laser). In the SEMS group, 24 (15%) patients required additional treatment. Nine of them (5.6%) required APC treatment for tumour overgrowth, 10 (6.3%) at least a second stent, three required both an additional stent and APC, one received laser treatment and one had eventually a percutaneous endoscopic gastrostomy after a second stent placement.
Univariate and multivariate analyses of risk factors affecting the survival of patients with inoperable oesophageal cancer, not receiving chemo- or radiotherapy, who had argon plasma coagulation (APC) or self-expandable metal stent (SEMS) as primary palliation modality, after stratification for disease stage. The only statistically significant factor in both analyses was treatment type (APC or SEMS)
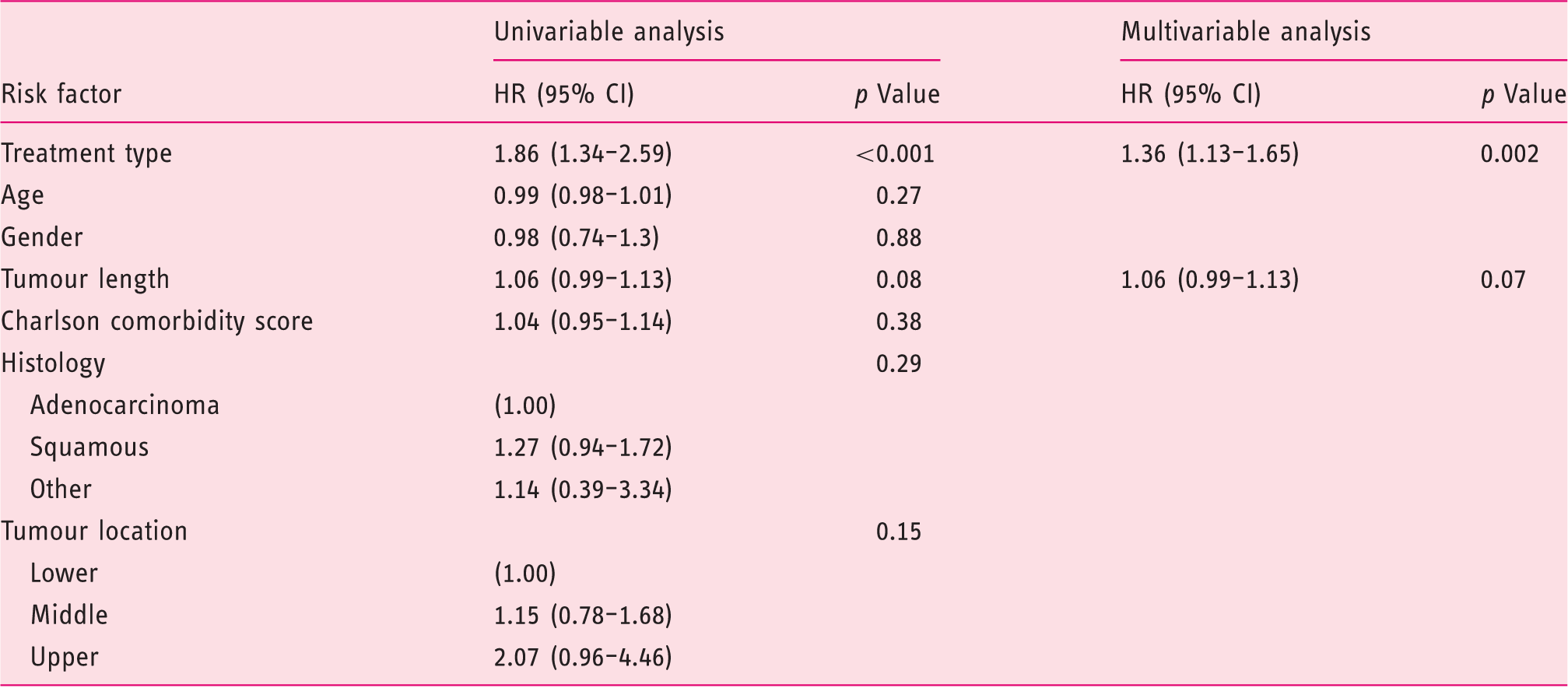
CI: confidence interval; HR: hazard ratio.
The overall median survival was 257 (IQR: 485, 135) and 102 (188, 41) days in the APC and SEMS group respectively. Patients treated with APC had significantly better median survival (log rank p < 0.001). Kaplan–Meier survival curves for stage III and IV patients treated with APC or SEMS are presented in Figures 2 and 3 respectively. Comparisons between treatment groups for patients belonging to less advanced stages were not performed due to small numbers, especially in SEMS group.
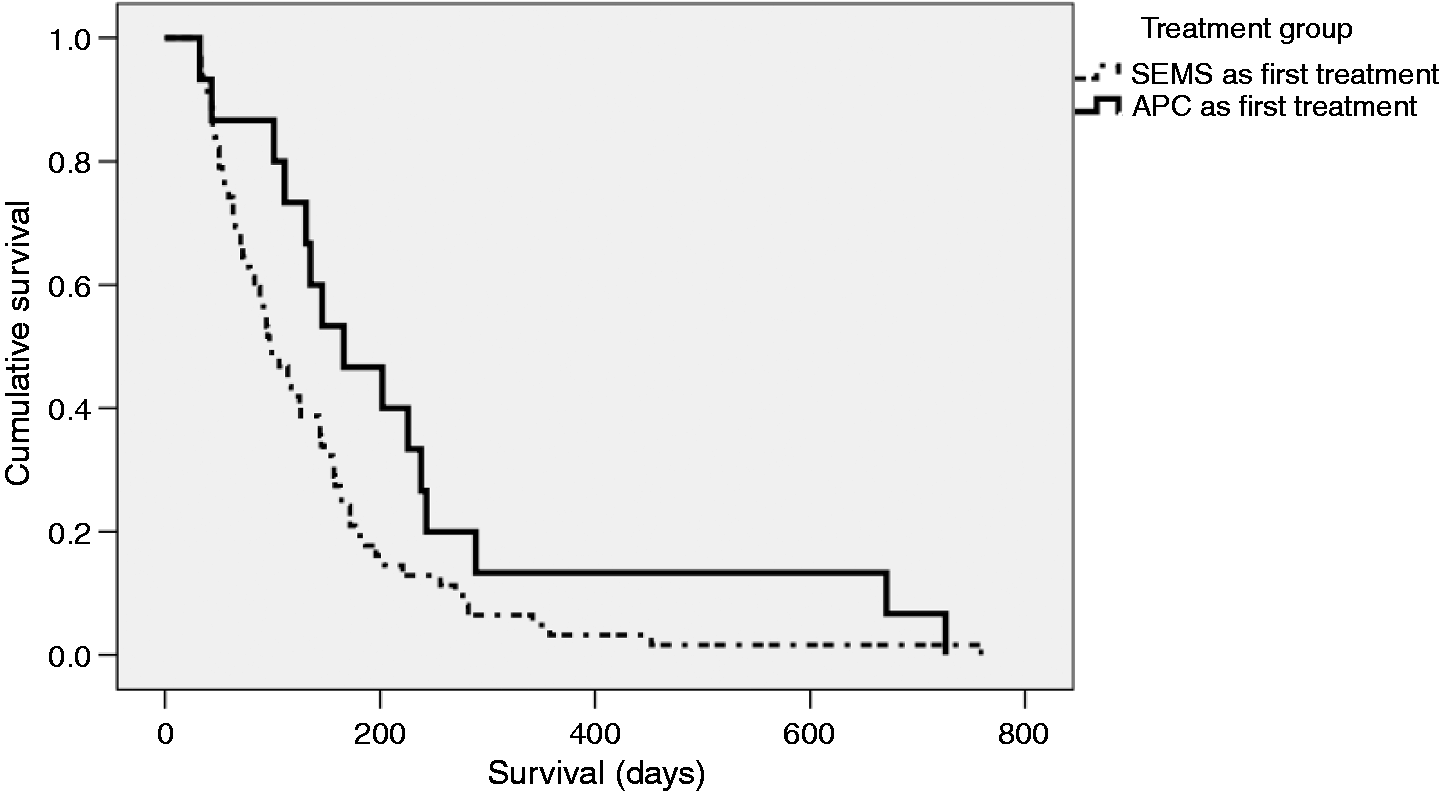
Kaplan-Meier survival curves for patients with stage III inoperable, oesophageal cancer, not receiving chemo- or radiotherapy, having either argon plasma coagulation(APC) or self-expandable metal stents (SEMSs) as initial palliative treatment. Median survival was higher in the APC group (257 days, IQR: 414, 124) compared to SEMS group (151 days, IQR: 241, 61). This difference was statistically significant (log rank p = 0.02). Kaplan-Meier survival curves for patients with stage IV inoperable, oesophageal cancer, not receiving chemo- or radiotherapy, having either argon plasma coagulation (APC) or self-expandable metal stents (SEMSs) as initial palliative treatment. Median survival was higher in the APC group (135 days, IQR: 238, 43) compared to SEMS group (70 days, IQR: 148, 32). This difference was statistically significant (log rank p = 0.05).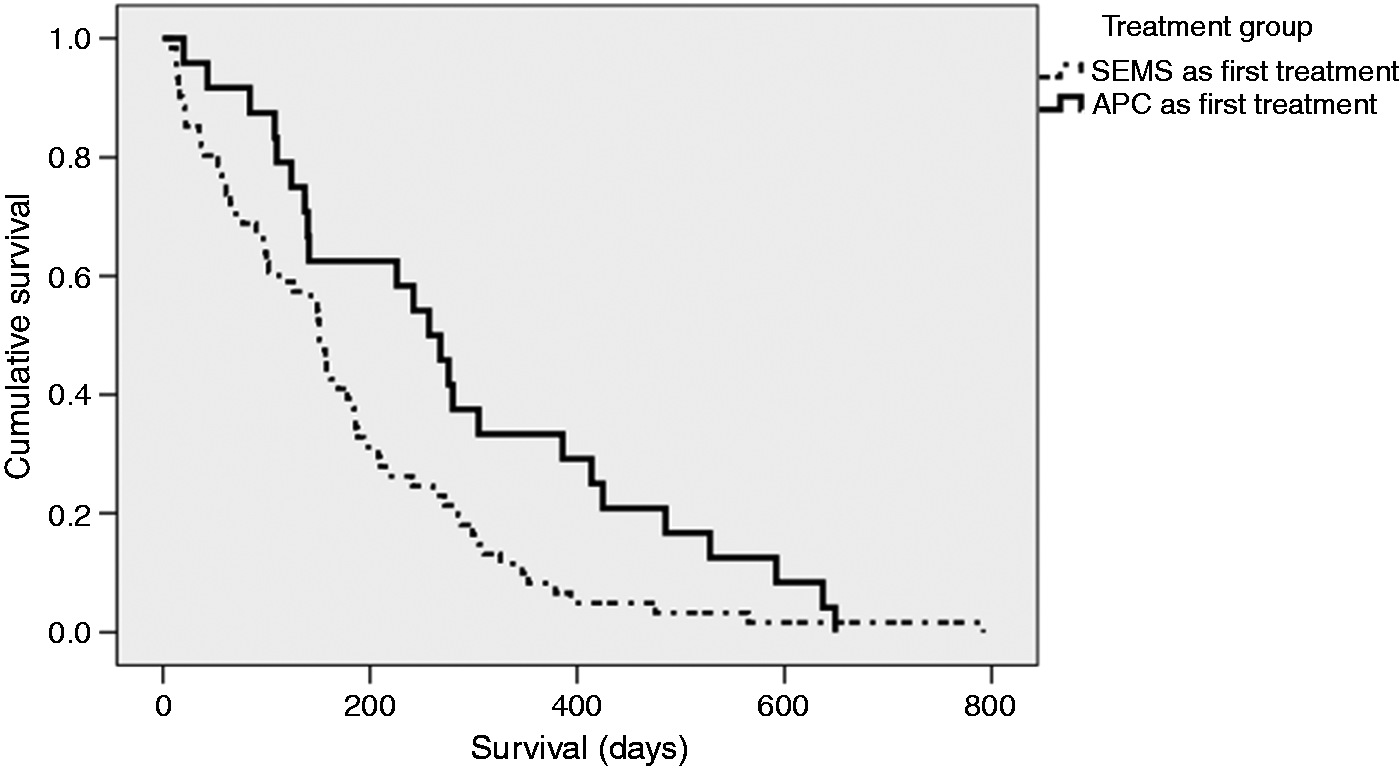
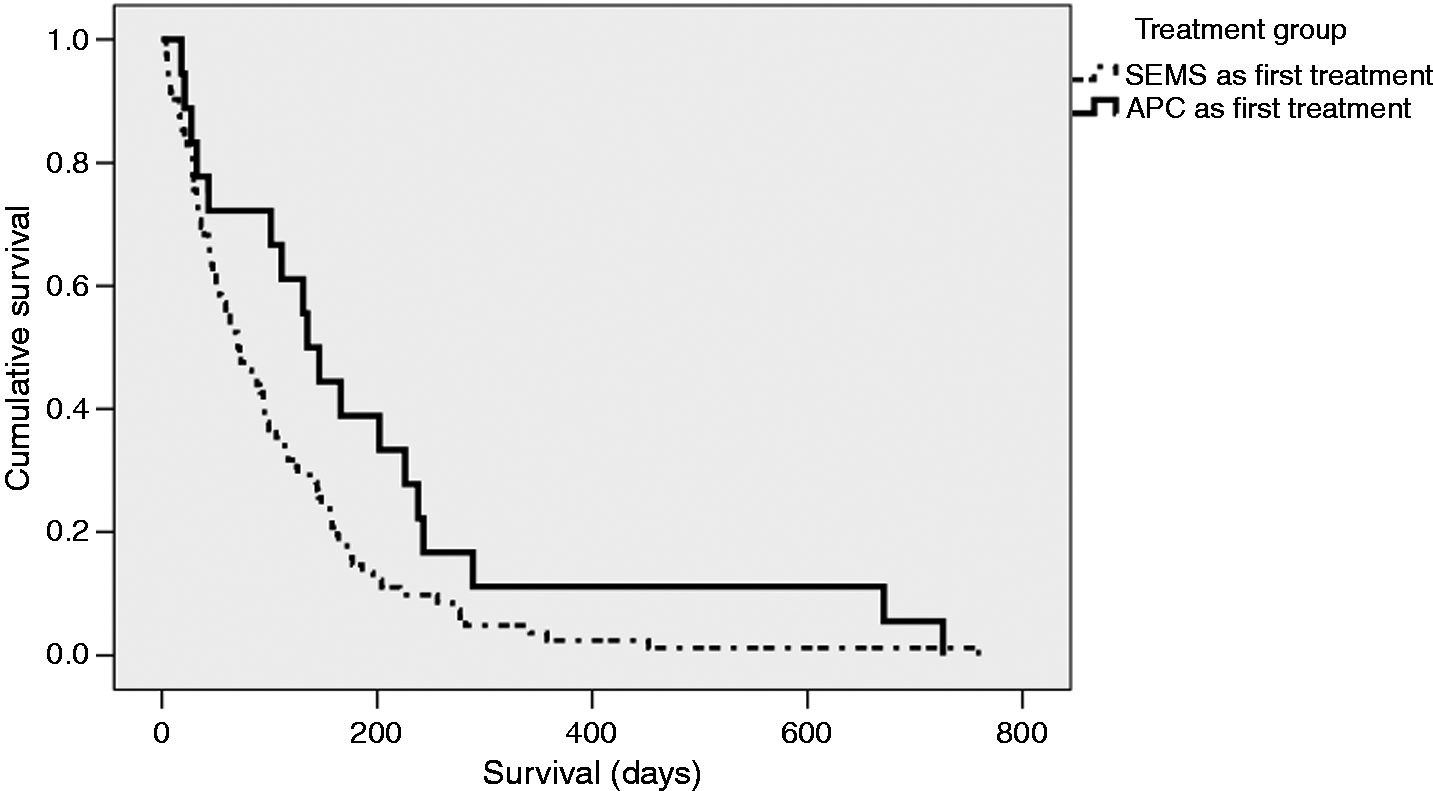
The overall median survival of stage III patients was 158 days (IQR: 285, 84). Stage III patients treated with APC had a median survival of 257 days (IQR: 414, 124), while patients treated with SEMS had a median survival of 151 days (IQR: 241, 61). Survival of patients treated with APC was significantly better (log rank p = 0.02).
Stage IV patients had an overall median survival of 83 days (IQR: 158, 32). Median survival of the APC group in stage IV disease was 135 days (IQR: 238, 43), while patients treated with SEMS had a median survival of 70 days (IQR: 148, 32). The difference was statistically significant (log rank p = 0.05).
Patients treated with SEMS had a 14-day mortality rate of 8.1%, compared to 0% in patients treated with APC. The respective 30-day mortality rates for SEMS and APC were 18.8% and 5.9%. Both differences were statistically significant (p = 0.01 for both).
Further analysis of the data set after excluding patients not surviving more than a month showed that again the type of treatment (APC or SEMS) was found as the only statistically significant factor in Cox regression, while stratifying for disease stage. In this sub-group analysis, median survival in stage III patients was 268 days (IQR: 425, 137) for APC, compared to 162 (IQR: 272, 99) for SEMS and in stage IV disease, median survival was 166 days (IQR: 243, 111) for APC compared to 97 (IQR: 164, 59) for SEMS. The difference was statistically significant in stage III (p = 0.04), whereas it was not in stage IV (p = 0.07). The relevant Kaplan-Meyer curves are presented in Figures 4 and 5, while the relevant Cox regression analysis is presented in Table 3.
Kaplan–Meier survival curves for patients with stage III inoperable, oesophageal cancer, not receiving chemo- or radiotherapy, having either argon plasma coagulation (APC) or self-expandable metal stents (SEMSs) as initial palliative treatment. Patients surviving less than 30 days were excluded. Median survival was higher in the APC group (268 days, IQR: 425, 137) compared to SEMS group (162 days, IQR: 272, 99). This difference was statistically significant (log rank p = 0.04). Kaplan–Meier survival curves for patients with stage IV inoperable oesophageal cancer, not receiving chemo- or radiotherapy, having either argon plasma coagulation (APC) or self-expandable metal stents (SEMSs) as initial palliative treatment. Patients surviving less than 30 days were excluded. Median survival in the APC group was 166 days (IQR: 243, 111). Median survival in SEMS group was 97 days (IQR: 164, 59). This difference was not statistically significant (log rank p = 0.07). Univariate and multivariate analyses of risk factors affecting the survival of patients with inoperable oesophageal cancer, not receiving chemo- or radiotherapy, having either argon plasma coagulation (APC) or self-expandable metal stent (SEMS) as primary palliation modality, after stratification for disease stage. Patients not surviving more than 30 days following the first treatment session (either APC or SEMS) were excluded. The only statistically significant factor in both analyses was treatment type (APC or SEMS). Tumour length was included in the multivariable analysis despite not being statistically significant, to enable direct comparison with the analysis presented in Table 2 of the main manuscript CI: confidence interval; HR: hazard ratio.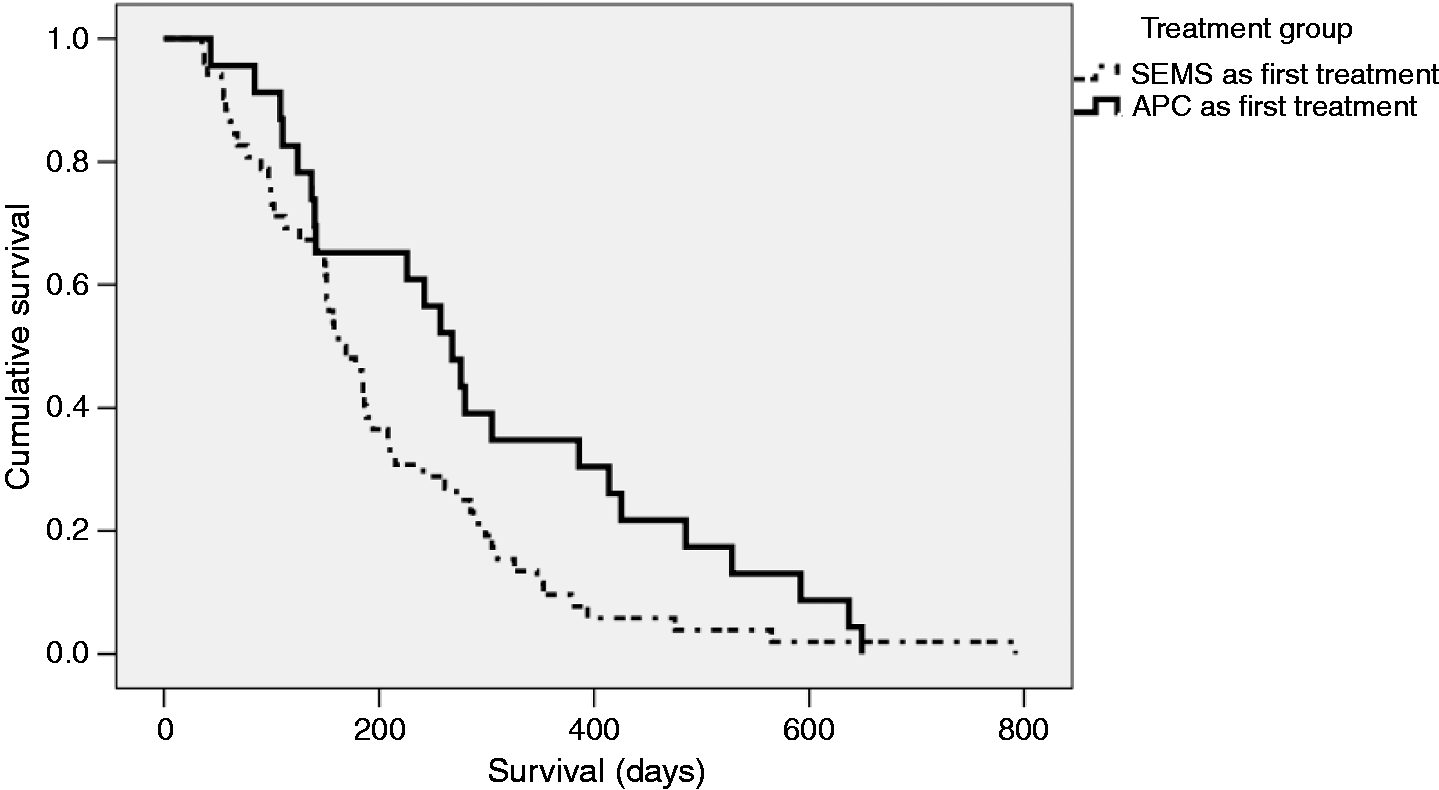
Discussion
The aims of palliation in patients with advanced oesophageal cancer are to overcome dysphagia and optimize quality of life by using interventions that have minimal adverse events. Even though chemo-radiotherapy is an option for dysphagia palliation in advanced oesophageal cancer and also conveys an advantage in survival compared with palliative endoscopic stenting alone, 18 a significant proportion of patients are not candidates for such treatments. The palliation modalities most widely used in such patients are stent insertion, brachytherapy and thermal ablation techniques.2–8 It has been shown, that that MDT assessment significantly improves staging accuracy for gastro-oesophageal cancer and ensures that correct management decisions are made for the highest number of individual patients. In an audit from our unit, overall staging accuracy as determined at the MDT meeting was high and resulted in only 2/118 (2%) patients being under-treated. 19
SEMSs are the mainstay of palliative treatment for malignant oesophageal obstruction. The apparent advantage of this approach is the relative ease of application in a single session achieving immediate results in relieving dysphagia. In contrast, ablative techniques require multiple sessions and significant administrative co-ordination efforts and therefore are less appealing, especially in busy tertiary centres. Nevertheless, the apparent dominance of SEMS in oesophageal cancer palliation over ablative techniques in not based on solid evidence. On the contrary, a single centre, randomized, prospective study demonstrated a significantly longer median survival of patients receiving laser treatment for palliation of inoperable oesophageal cancer compared to patients treated with stents. 5 An increased survival rate of patients treated with various ablative techniques including APC, over SEMS, was also documented in a randomized, controlled, multicentre study. 22 Those results raise the question whether SEMS dominance of the field is at least partially explained by their certain advantage in logistics rather than in a clear benefit in patient palliation and survival. This study tried to provide some insight into this issue.
Most studies regarding SEMS included patients who were unfit for chemotherapy and/or radiotherapy and hence median survival was low, ranging from 68–145 days.2,3,5,8,18 This is in accordance with the results of this study which showed an overall median survival of 102 days in patients receiving SEMS as a primary palliation modality.
The effectiveness of APC in tumour debulking has been studied in a number of studies. Eickhoff et al. showed a significant effect of both pulsed and forced APC in achieving tumour debulking in GI cancers, with a response to treatment exceeding 80%. 10 In a retrospective analysis 6 of 83 patients who had APC for oesophageal malignancy, Heindorff et al. reported a mean of six APC sessions to maintain lumen patency. This was higher compared with the median of three (mean = 4), reported in this study. This could be explained by different intervals between the consecutive sessions adopted by each centre. The same study reported an average survival of 146 days in 63 of patients who died in the investigation period, which is significantly lower compared with our study’s overall median survival of 257 days. However, the proportion of stage IV patients in the aforementioned study was 41%, which was significantly higher compared with our study (25.7%) in the APC group.
To our knowledge so far, the only direct comparison of APC versus SEMS in inoperable oesophageal cancer followed a different study design. 23 In that retrospective study by Kofoed et al. the study population was divided in three groups: patients receiving APC alone, SEMS alone and a combination of APC and SEMS. A proportion of patients in all categories also received chemo-radiotherapy. There was no difference in survival between ‘SEMS alone’ and ‘APC alone’ groups. The former had a mean survival of 134 days and the latter 114 days. Significantly better survival was observed in patients receiving a combination of both modalities compared to either modality alone. Additionally, patients receiving chemo-radiotherapy and SEMS plus/or APC had a better survival compared to the rest of the cohort. Direct comparison to our results is impossible since only patients with adenocarcinoma were included, the results were not stratified by disease stage (only distribution of T, N and M was reported) and patients also received chemo-radiotherapy. Furthermore, we chose not to compare APC or SEMS alone as distinct modalities, but rather to compare two different treatment strategies: APC first, followed by SEMS when repeat APC was found ineffective and SEMS as primary modality, followed by APC in cases of tumour overgrowth. In that sense, our analysis was more on an intention-to-treat basis.
This study has certain caveats. It is a retrospective, single centre study and results presented should be appreciated in that context. It is difficult to claim immunity to selection bias in a retrospective study, especially when some baseline characteristics are different between patient groups. Some of those patient characteristics would be expected to negatively affect the prognosis in the APC group (e.g. older age, higher CCS), while the shorter median tumour length could potentially improve it. In order to control for all those factors and find the ones independently associated with survival, Cox regression was used after stratification for disease stage. It was clear that treatment type was the only factor independently correlated to survival after stratification for disease stage, in the multivariate analysis.
In order to minimize any potential selection bias effect (i.e. assigning the most frail patients in the SEMS group), further analyses, excluding the patients who died in the first month, were performed and confirmed that the only factor found to be statistically significant in the multivariate model was the type of treatment (data shown in Table 3). In addition, the survival benefit of APC remained, at least in stage III disease.
The 30-day mortality in the SEMS group was comparable to previously reported results ranging from 11–40%.24–27 Although such results could raise the concern that selection of more frail patients for SEMS could be an explanation for the higher mortality, it is certain from the demographic data that patient frailty was not a set criterion when discussing treatment options.
Cost is an important factor in every medical intervention and the need for repeat APC applications certainly needs further consideration from this point of view. Virtually all patients had more than one APC application and 35.3% needed other endoscopic procedures (mainly SEMS placement). However, 15% of patients in the SEMS group also required repeat endoscopic procedures including further stent insertions, while re-intervention rates as high as 38% have been previously reported after SEMS placement. 28 In view of the significantly higher cost of SEMS compared to APC catheters (approximately five times more expensive in the UK), the actual difference in cost of the two treatment strategies appeared to be determined primarily by the costs related to the number of endoscopic procedures rather than the cost of consumables used. Patients treated with APC survived longer and thus had a higher number of interventions resulting in higher costs. Any future prospective studies should address the cost effectiveness of APC versus SEMS placement for palliation of oesophageal cancer in detail.
This retrospective study has several strengths. We followed a rigorous protocol in patient inclusion and analysis. Staging was of very high standards, using all the available modalities available (CT, EUS, PET) and was based on a multidisciplinary decision thus making it as accurate as possible. Detailed demographics were available for all patients included and procedure related factors as well as mortality were documented prospectively with accuracy on case notes and electronic records.
The palliation of inoperable oesophageal cancer is a challenging issue and multiple factors should be taken into consideration. This study provided evidence that a strategy based on APC as the primary palliation modality, supplemented by the placement of SEMS only after APC failure or when patients become intolerable of repeated endoscopies, might actually provide a significant survival benefit, compared to SEMS as the primary treatment. Those findings need to be interpreted in the context of a retrospective study and therefore, further, prospective, randomized studies are needed to confirm those results.
Footnotes
Acknowledgements
The authors would like to thank Michelle Gibson and Louise Graham for their help with data collection.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of interest
None declared.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.