
Abstract
Background
Little is known about interval cancers (ICs) in colorectal cancer (CRC) screening.
Objective
The purpose of this study was to identify IC characteristics and compare these with screen-detected cancers (SCs) and cancers in non-participants (NPCs) over the same time period.
Design
This was an observational study done in the first round of the Scottish Bowel Screening Programme. All individuals (772,790), aged 50–74 years, invited to participate between 1 January 2007 and 31 May 2009 were studied by linking their screening records with confirmed CRC records in the Scottish Cancer Registry (SCR). Characteristics of SC, IC and NPC were determined.
Results
There were 555 SCs, 502 ICs and 922 NPCs. SCs were at an earlier stage than ICs and NPCs (33.9% Dukes’ A as against 18.7% in IC and 11.3% in NPC), screening preferentially detected cancers in males (64.7% as against 52.8% in IC and 59.7% in NPC): this was independent of a different cancer site distribution in males and females. SC in the colon were less advanced than IC, but not in the rectum.
Conclusion
ICs account for 47.5% of the CRCs in the screened population, indicating approximately 50% screening test sensitivity: guaiac faecal occult blood testing (gFOBT) sensitivity is less for women than for men and gFOBT screening may not be effective for rectal cancer.
Keywords
Introduction
In the context of iterative cancer screening, the term ‘interval cancer’ denotes a cancer that has been diagnosed after a negative screening test result in the interval before the participant has had an opportunity to repeat the test. 1 Thus, in colorectal cancer (CRC) screening programmes that use biennial guaiac faecal occult blood testing (gFOBT) as the initial investigation, such as are currently in place across the UK, an interval cancer (IC) represents a cancer that has been diagnosed within two years of a negative test result.
While CRC may arise de novo in the interval between screening invitations, this is almost certainly a rare event, and, for the most part ICs are likely to be cancers that have been missed by the screening test, either at a non-invasive (adenoma) or an earlier invasive stage. The percentage of cancers arising in the screened population that are IC is therefore a key performance indicator of a population screening programme, since it provides a pragmatic index of test sensitivity, i.e. the ability of the test to detect CRC.
Despite this, relatively little is known about IC in CRC screening programmes. Worldwide, the most commonly employed non-invasive CRC screening tests involve the detection of haemoglobin in faeces, and this is predicated on the results of population-based trials of gFOBT, all of which demonstrated a reduction in disease-specific mortality with biennial screening. 2 However, these studies have little data on interval cancers, and there have been only two reports describing the pattern of IC occurrence in pilot studies of gFOBT screening, one from Scotland 3 and one from Catalonia, 4 and none from national programmes that have been fully rolled out.
In Scotland, a demonstration pilot 5 based on the Nottingham randomised trial 6 ran from 1 March 2000–31 May 2007 for individuals aged 50–69 years and comprised three rounds of screening, involving only three of the 14 National Health service (NHS) Boards in Scotland responsible for patient care, less than 20% of the population. As a result of the success of the pilots, 5 CRC screening was rolled out across the country starting on 1 June 2007 and was offered to an expanded age range, those between the ages of 50–74 years using a novel two-tier reflex screening algorithm. Here, the characteristics of IC arising in all individuals invited to participate in the now fully rolled-out Scottish Bowel Screening Programme (SBoSP) between 1 June 2007–31 May 2009, and followed up until 30 November 2011, are reported. This interval was chosen to allow time for reliable identification of the ICs from the Scottish Cancer Registry and to ensure that complete data for CRC was available on the Registry. We also compare the ICs with the screen-detected cancers (SCs) and the cancers diagnosed in those who chose not to participate in screening during the same time period, termed non-participant cancers (NPCs).
Methods
When the SBoSP was rolled out to the rest of the country, the screening process differed from that employed in the pilot in two important respects. First, the age range was extended from 50–69 years to 50–74 years. Second, instead of using a second gFOBT for a weak positive result (i.e. for those who had one to four of the six windows positive in the gFOBT), a qualitative faecal immunochemical test (FIT) (Hema-Screen SPECIFIC, Immunostics Inc., Ocean, New Jersey, USA) was employed. 7 This was based on work that had demonstrated improved performance of this novel two-tier reflex gFOBT/FIT screening algorithm in terms of fewer false positives. 8 Moreover, although some resident in the three NHS Boards participated one, two or three times in the demonstration pilot, particularly with the age range extension, this study can be considered to be concerned with prevalence round screening.
For the purposes of this report, the following definitions were employed: an SC was defined as a CRC diagnosed as a result of investigations (usually colonoscopy) carried out in response to a positive test result, an IC was defined as a CRC diagnosed within two years of a negative test result or time between negative test result and next round invitation, whichever occurred first. A NPC was defined as a cancer arising in an individual who had been invited to participate in the SBoSP but had not done so. A missed cancer was defined as a CRC diagnosed within two years of a negative colonoscopy carried out in response to a positive test result and a miscellaneous cancer as a CRC diagnosed in an individual who either defaulted before a final test result was achieved, refused investigation after a positive test result, was found to be unfit for colonoscopy, was already undergoing investigations for symptoms, was admitted as an emergency, or died between screening investigations.
A right-sided (R) colonic cancer was defined as a cancer recorded as being between (and including) the caecum and the splenic flexure (ICD-10 codes C180–C185). A left-sided (L) colonic cancer was a cancer recorded as being between (and including) the descending colon and sigmoid colon (ICD-10 codes C186–C187). A rectal (RE) cancer was defined as a cancer recorded as being in the rectum or recto-sigmoid junction (ICD-10 codes C19–C20). There were also a small number of not otherwise specified colonic cancers (NoSCs) (ICD-10 codes C188–C189) which were included in the analysis for completeness.
In order to categorise the CRCs in the manner described above, all screening records were linked with confirmed CRC records in the Scottish Cancer Registry (SCR). This permitted the calculation of the time between the final test result being generated and the date that the CRC was diagnosed.
The stage at diagnosis of the CRCs was described using the Dukes’ staging system and, although polyp cancers (cancers removed by polypectomy at colonoscopy) were identifiable in the SC group, such data were unavailable from the registry data. Thus, all polyp cancers were included in the ‘A’ Dukes’ category for the current analysis.
Socio-economic deprivation was estimated using the Scottish Index of Multiple Deprivation (SIMD) 2009, which is based on small area data zones each containing around 250 households which can be identified by postcode. Seven different aspects of deprivation are identified in the SIMD: employment, income, health, education, access to services, crime and housing. The index provides a relative ranking for each data zone and this is commonly divided into quintiles, with quintile one representing the most deprived, and quintile five the least deprived. The results presented here are from the ‘population-weighted’ SIMD 2009, which allows for a more accurate analysis of the deprived population rather than deprived areas.
The SCR utilises multiple sources, and routine indicators of data quality indicate very nearly complete case ascertainment. A study of the year 1992 estimated completeness of ascertainment of 96.5% for all cancers and 98.5% for CRCs. 9
In all cases, the Chi-squared test was used to test the statistical significance of the distribution of the results.
Results
Overall distribution of cancers.
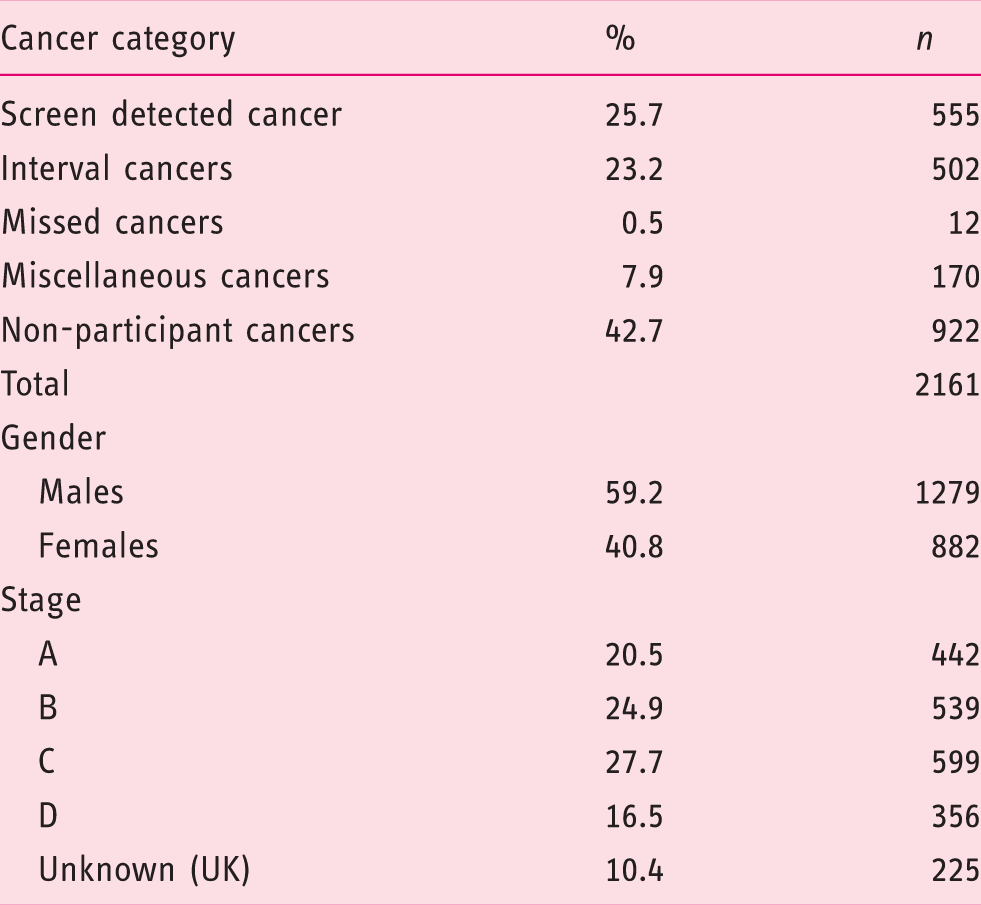
Distribution of screen-detected cancer (SC), interval cancer (IC) and non-participant cancer (NPC) by gender and ratios of IC to all cancers and IC to all participant cancers.

SC vs IC: χ2 = 15.42, p < 0.0001; IC vs NPC: χ2 = 6.26, p = 0.0124; SC vs NPC: χ2 = 3.71, p = 0.0542.
Distribution of screen-detected cancer (SC), interval cancer (IC) and non-participant cancer (NPC) by stage and ratios of IC to all cancers and IC to all participant cancers.
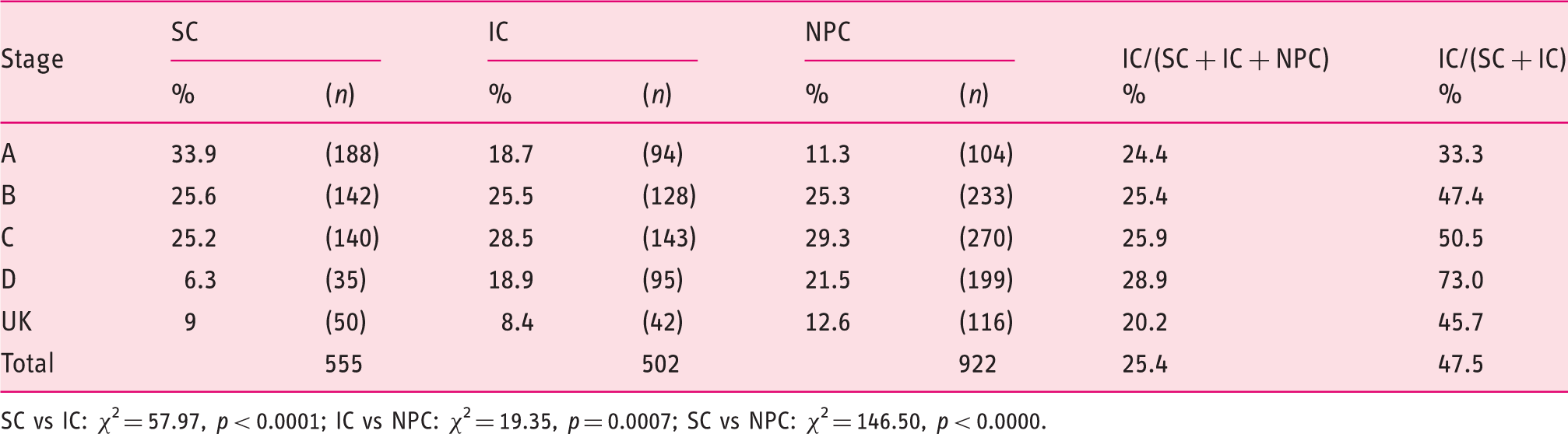
SC vs IC: χ2 = 57.97, p < 0.0001; IC vs NPC: χ2 = 19.35, p = 0.0007; SC vs NPC: χ2 = 146.50, p < 0.0000.
Distribution of screen-detected cancer (SC), interval cancer (IC) and non-participant cancer (NPC) by site and ratios of IC to all cancers and IC to all participant cancers.
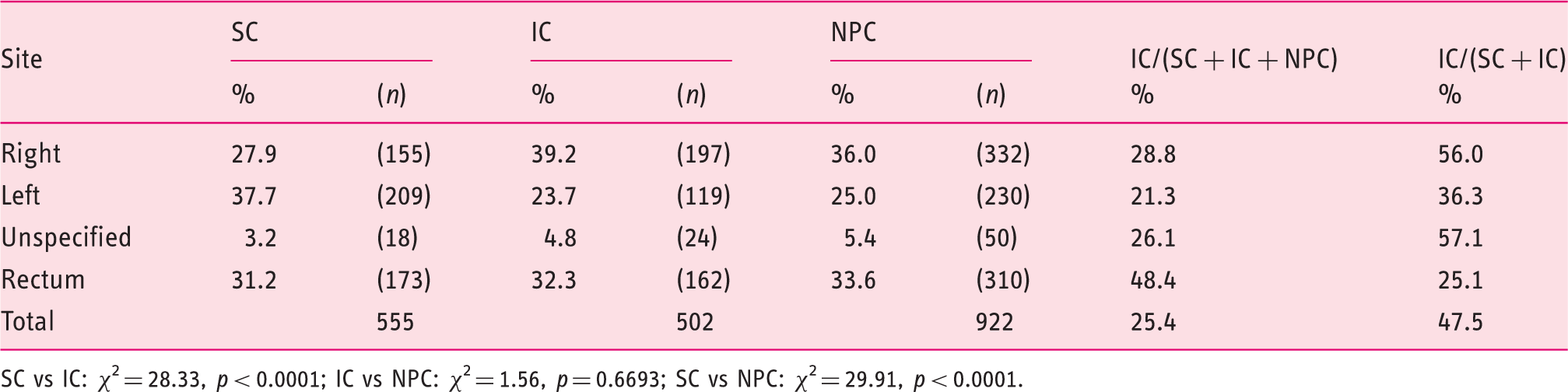
SC vs IC: χ2 = 28.33, p < 0.0001; IC vs NPC: χ2 = 1.56, p = 0.6693; SC vs NPC: χ2 = 29.91, p < 0.0001.
Distribution of screen-detected cancer (SC), interval cancer (IC) and non-participant cancer (NPC) by age group (years) and ratios of IC to all cancers and IC to all participant cancers.
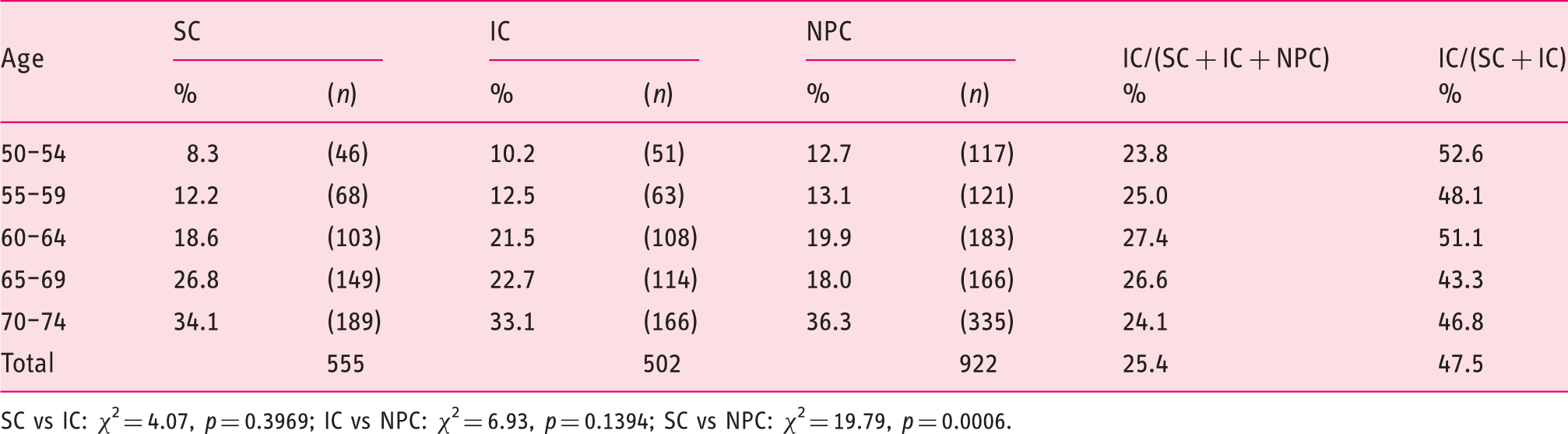
SC vs IC: χ2 = 4.07, p = 0.3969; IC vs NPC: χ2 = 6.93, p = 0.1394; SC vs NPC: χ2 = 19.79, p = 0.0006.
Distribution of screen-detected cancer (SC), interval cancer (IC) and non-participant cancer (NPC) by deprivation category (1: most deprived, 5: least deprived) and ratios of IC to all cancers and IC to all participant cancers.
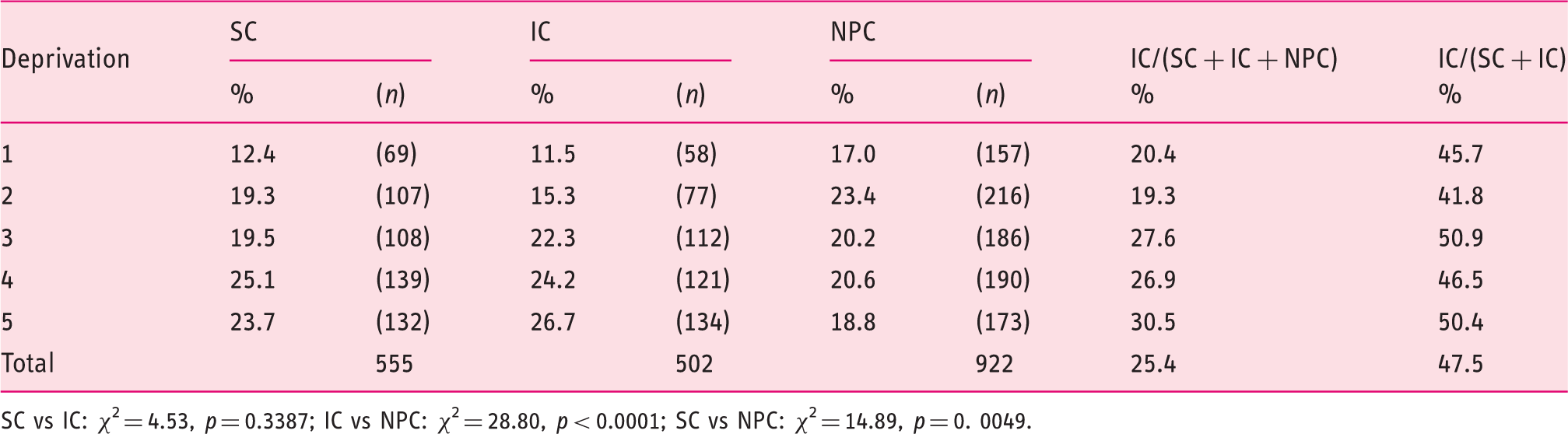
SC vs IC: χ2 = 4.53, p = 0.3387; IC vs NPC: χ2 = 28.80, p < 0.0001; SC vs NPC: χ2 = 14.89, p = 0. 0049.
There were also more males than females amongst the NPC cases, and this was less pronounced than in the SC group and more than in the IC group. It can be seen that the stage distribution was more favourable in the SC group than in both the IC and NPC groups, and that the distribution in the IC group was more favourable than in the NPC group. The site distribution indicates that R colon cancers were less common in the SC group than in either the IC or the NPC groups. The age distribution indicates a younger population in the NPC group than the SC group, but little difference between SC and IC or IC and NPC. There was a trend towards the more deprived end of the spectrum in the NPC group when compared to both SC and IC, but no difference between SC and IC groups.
Overall relationship between tumour site and stage.
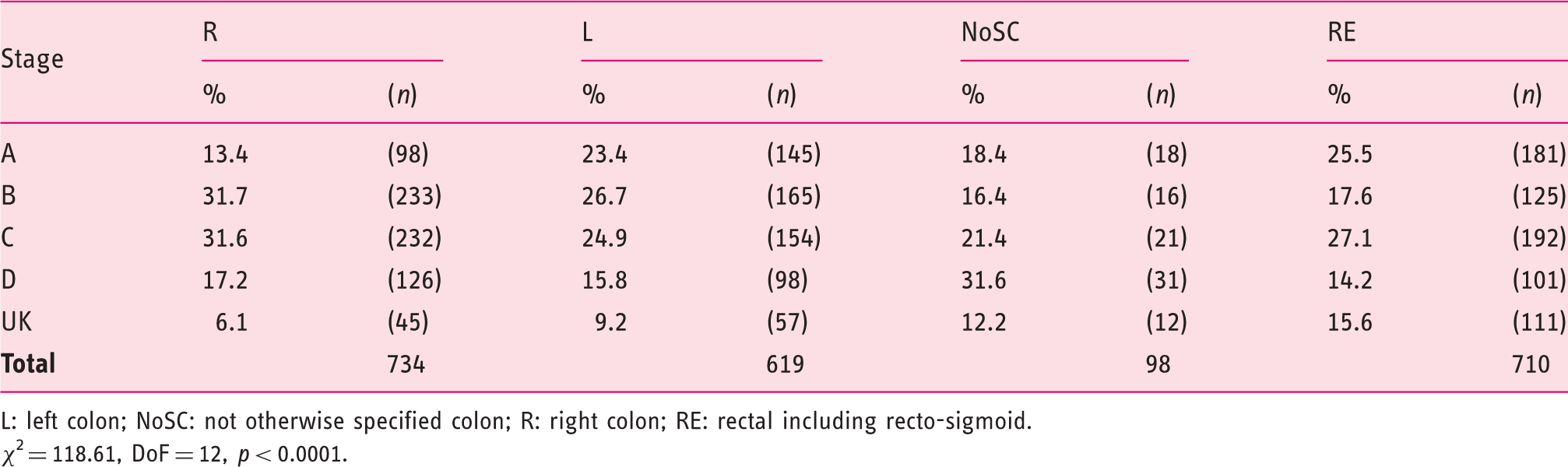
L: left colon; NoSC: not otherwise specified colon; R: right colon; RE: rectal including recto-sigmoid.
χ2 = 118.61, DoF = 12, p < 0.0001.
Overall relationship between tumour site and gender.
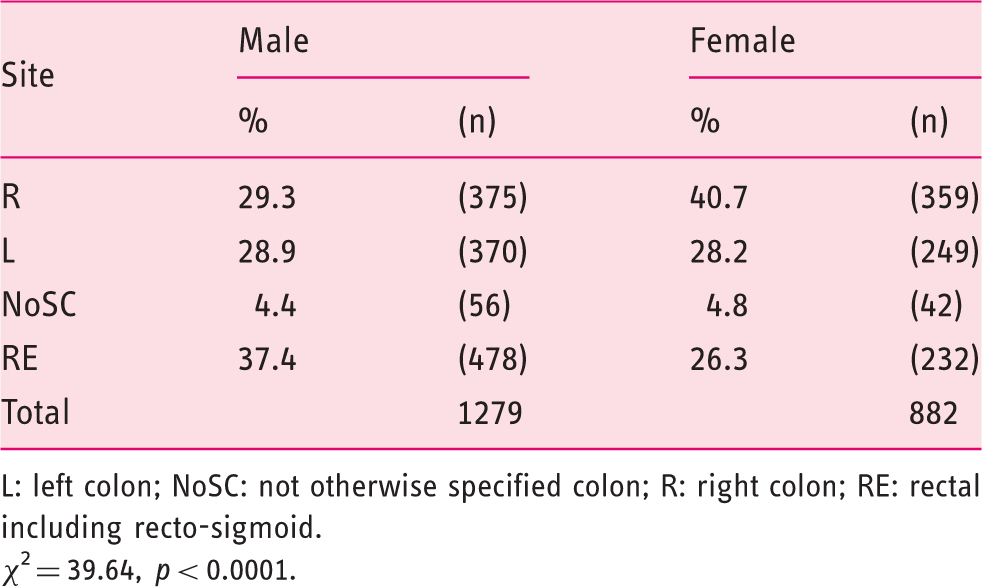
L: left colon; NoSC: not otherwise specified colon; R: right colon; RE: rectal including recto-sigmoid.
χ2 = 39.64, p < 0.0001.
Overall relationship between tumour stage and gender.

χ2 = 8.67, p = 0.069.
Relationship between site, screening status and stage.
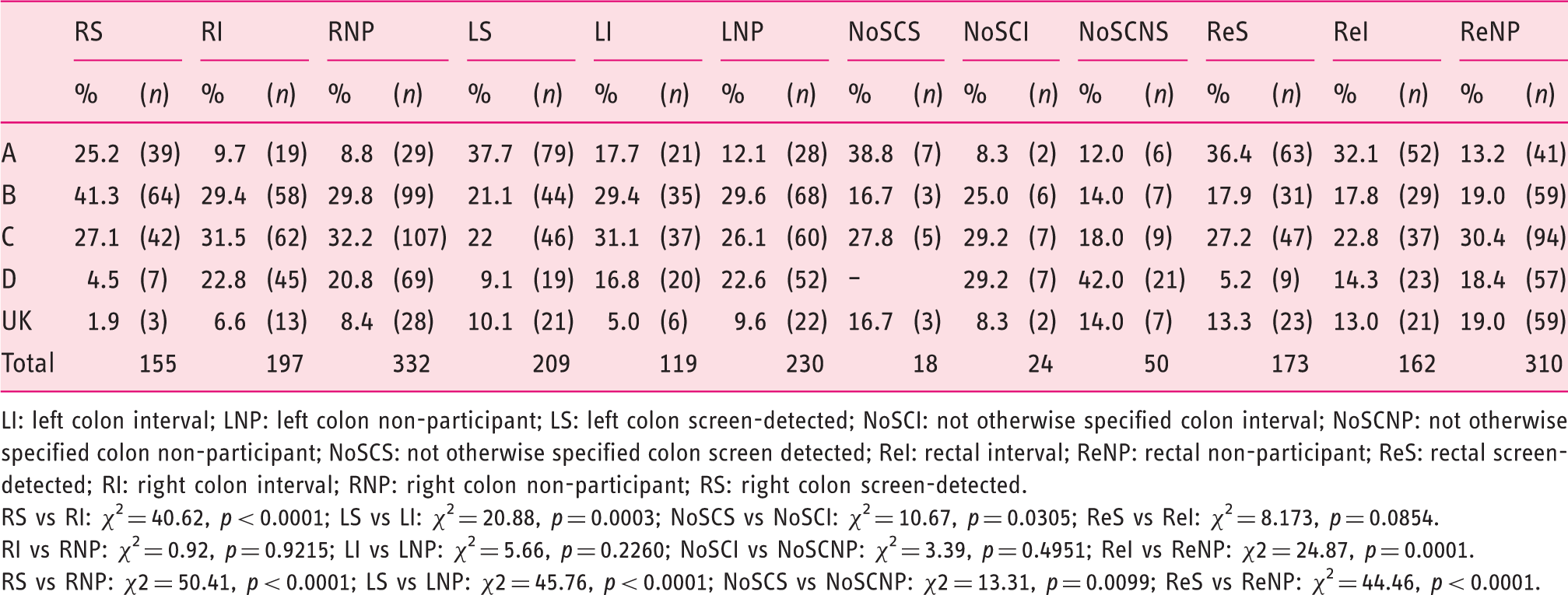
LI: left colon interval; LNP: left colon non-participant; LS: left colon screen-detected; NoSCI: not otherwise specified colon interval; NoSCNP: not otherwise specified colon non-participant; NoSCS: not otherwise specified colon screen detected; ReI: rectal interval; ReNP: rectal non-participant; ReS: rectal screen-detected; RI: right colon interval; RNP: right colon non-participant; RS: right colon screen-detected.
RS vs RI: χ2 = 40.62, p < 0.0001; LS vs LI: χ2 = 20.88, p = 0.0003; NoSCS vs NoSCI: χ2 = 10.67, p = 0.0305; ReS vs ReI: χ2 = 8.173, p = 0.0854.
RI vs RNP: χ2 = 0.92, p = 0.9215; LI vs LNP: χ2 = 5.66, p = 0.2260; NoSCI vs NoSCNP: χ2 = 3.39, p = 0.4951; ReI vs ReNP: χ2 = 24.87, p = 0.0001.
RS vs RNP: χ2 = 50.41, p < 0.0001; LS vs LNP: χ2 = 45.76, p < 0.0001; NoSCS vs NoSCNP: χ2 = 13.31, p = 0.0099; ReS vs ReNP: χ2 = 44.46, p < 0.0001.
Relationship between gender and site broken down by screening status.
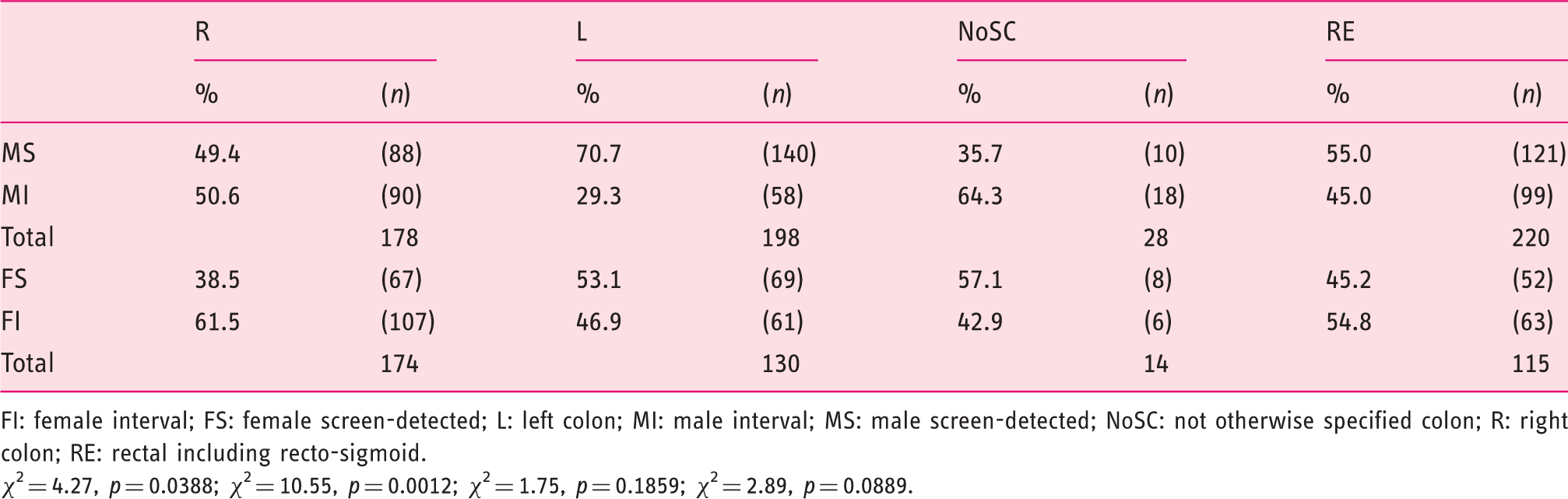
FI: female interval; FS: female screen-detected; L: left colon; MI: male interval; MS: male screen-detected; NoSC: not otherwise specified colon; R: right colon; RE: rectal including recto-sigmoid.
χ2 = 4.27, p = 0.0388; χ2 = 10.55, p = 0.0012; χ2 = 1.75, p = 0.1859; χ2 = 2.89, p = 0.0889.
This analysis demonstrated that SC had a more favourable stage distribution than IC and NPC in both the R and L colons, but that there was no difference between IC and NPC. In the RE, however, there was no difference in the stage distribution between SC and IC, but both had a significantly more favourable distribution than NPC.
Additionally, since screen-detection was found to be related to both gender and site, SC and IC were broken down by site for males and females separately. This is shown in Table 11, which demonstrates that SCs were more common in males for both R and L cancers, but not significantly so for RE.
Discussion
This detailed study of cancers diagnosed in the population invited to participate in the first mainly prevalence screening round of the SBoSP confirms that SCs are diagnosed at an earlier stage than ICs and NPCs, that screening preferentially detects cancers in males (as evidenced by the significant gender difference in the proportion of SCs and ICs), that cancers in the right colon are less common in the screen-detected group, that right-sided colon cancers have a less favourable stage distribution than left-sided and that right-sided cancers are less commonly seen in males than females. In addition to confirming, in greater detail, the findings presented in previous reports, both by our group
3
and others,3,10 the results described here pose two important new questions:
Firstly, since right-sidedness is associated with both poorer stage and a resistance to screen-detection, is early diagnosis by screening a function of the site of the tumour? Secondly, since right-sidedness is associated with female gender as well as a resistance to detection through screening, is the well-documented better sensitivity of gFOBT screening in males compared with females also related to tumour site?
We have been able to answer these new questions from our current analysis. It is clear that both right-sided and left-sided screen-detected colonic cancers do have a more favourable stage distribution than either ICs or NPCs, indicating that the screening process does indeed identify earlier stage disease in the colon and results in down-staging. In the rectum, however, this does not seem to be the case. The stage distribution was very similar in the SCs and the ICs, and both were more favourable than NPCs.
It is interesting to speculate why this should be. Rectal cancer more often presents with rectal bleeding than colon cancer, and in the Nottingham trial of gFOBT screening it was observed that during the study the stage at presentation of rectal cancer improved in the control group as well as in the group offered screening, but that this was not seen in colon cancer. 11 It can be hypothesised that this was caused by a halo effect of the screening programme which raised awareness of the significance of the presence of frank blood seen in faeces, both in those not offered screening, and amongst general practitioners. A similar argument may be applied to our findings; it is possible that those who had taken up the offer of screening had an already heightened awareness of the implications of signs of rectal bleeding, so that, if this occurred after a negative test result, they engaged with primary care promptly, whereas those who had not taken up the offer of screening were less likely to appreciate the importance of this symptom, either because they were less health conscious or because they had not been exposed to the messages delivered by engaging with the SBoSP.
We have also been able to show that screen-detection occurs more often in males than in females in both the right and the left colon. This may also be the case in the rectum, although this did not reach statistical significance. Thus the difference in sensitivity of gFOBT for CRCs between males and females is not explained by the gender difference in tumour site. Why this difference in sensitivity should exist is not clear but, in an evaluation of quantitative FIT in a population in Scotland, we have shown that men tend to have significantly higher faecal haemoglobin concentrations than women. 12 This finding, confirmed in other countries 13 although currently of obscure aetiology, may explain the differential sensitivity phenomenon.
Our findings with respect to age and deprivation are also worthy of comment. Firstly, the age of people diagnosed with screen-detected disease was slightly greater than those with CRC who had not participated in screening. This is in keeping with previous findings that uptake of screening and faecal haemoglobin concentrations tend to increase with age, 12 and this may have the effect of exaggerating the association between age and CRC risk. Secondly, both the SC and IC groups exhibited a deprivation gradient, with more cancers being diagnosed in the less deprived categories, and this was not seen amongst the NPCs. This undoubtedly reflects the well-described deprivation gradient associated with screening uptake and the decrease of positive predictive value of gFOBT with increasing deprivation. 14 Moreover, although socioeconomic deprivation impacts on uptake and thereby proportion of SCs to non-SCs, this does not affect the sensitivity of the screening episode (screen-detected divided by screen-detected + interval CRC).
Conclusions
In summary, this study is the first to address ICs in a rolled-out national population-based screening programme for CRC using gFOBT as the initial screening modality. It demonstrates that ICs make up a substantial proportion of cancers diagnosed in the screened population when a biennial screening strategy using an initial gFOBT yielding a positivity of around 2% is used, and serves to reinforce current advice to participants not to regard a negative test result as a ‘certificate of health’ and not to ignore symptoms. It is likely that the proportion of ICs will increase with time, as demonstrated in our previous study of three biennial pilot screening rounds, 5 but it is not yet clear at what level and when this proportion will plateau. In any event, moving into the future, an IC rate of this magnitude is unlikely to be acceptable to the population being offered screening and efforts to overcome this problem constitute an essential component of screening research and development.
It is also interesting that rectal cancer is diagnosed at roughly the same stage in the group accepting screening regardless of whether or not the gFOBT result is positive or negative, suggesting that an alternative strategy may be required to detect rectal cancer more effectively through screening.
Finally, women are at a disadvantage in CRC screening employing gFOBT, both because they are at higher risk of right-sided cancers, which are less likely to generate a positive test result, and because they are inherently less likely to have a positive test result with CRC at any site.
The solution to these issues may be multifactorial, and a screening programme that offers both faecal testing for the presence of blood and endoscopy of the rectum and distal colon may pay dividends. 15 equally important, however, is the advent of the use of automated quantitative FIT analysis which offers a much more flexible approach to CRC screening. Using this technology, it is possible to set the cut-off faecal haemoglobin (f-Hb) concentration to suit colonoscopy capacity and to take account of gender and age differences in f-Hb concentrations,12,13 and possibly deprivation. 16 In addition, it is plausible that decreasing the cut-off f-Hb used so as to increase the sensitivity while extending the screening interval to offset the increase in colonoscopy demand or determining the screening interval on the basis of the index f-Hb could improve the performance of a screening programme.
Footnotes
Funding
This study was funded by the Chief Scientist Office of the Scottish Government Health Department. Project: Establishing a Bowel Screening Research Unit (Grant Ref: CZH/6/4). The funder had no role in the study design, data collection, statistical analyses, interpretation of the results, or writing of the manuscript.
Conflict of interest
CGF has acted as a consultant for Immunostics Inc., Mode Diagnostics and Kyowa-Medex Co. Ltd, and has received support for travel from Alpha Labs Ltd. All other authors declare no competing interests.