
Abstract
Crohn’s disease is a chronic inflammatory bowel disease potentially involving any segment of the gastrointestinal tract. Extra-intestinal manifestations may occur in 6%–40% of patients, and disorders of the skin are among the most common. This manuscript will review skin manifestations associated to Crohn’s disease, with a particular focus on lesions associated to anti-tumour necrosis factor therapy.
Keywords
Introduction
Crohn’s disease (CD) is a chronic disorder of unknown aetiology characterised by noncaseating granulomatous inflammation of the gastrointestinal tract. Extra-intestinal manifestations may occur in 6%–40% of patients.1–6 Some of these manifestations are related to the activity of CD, whereas others have an independent course. 6 Epidemiological and clinical variables that may influence the development of extra-intestinal manifestations have not clearly been defined. In this review, we will analyse skin manifestations which may occur in CD patients. Moreover, mounting evidence suggests that a number of skin lesions in CD patients may be related to the use of tumour necrosis factor alpha (TNF-α) antagonists which are being increasingly used for the management of CD patients. Therefore, we will also focus on the prevalence of skin lesions related to anti-TNF therapy, including skin malignancies, such as malignant melanoma (MM) or non-melanoma skin cancers (NMSCs).
Skin and oral lesions
It is estimated that between 6% and 40% of all patients with CD may suffer from an extra-intestinal manifestation.1–6 A number of these manifestations may occur during treatment and may lead to interruption of therapy in order to assess whether they are drug related or simply linked to the underlying inflammatory bowel disease (IBD). 3
Cutaneous manifestations of CD are among the most common extra-intestinal disorders and have been classified into specific manifestations, characterised by granulomatous inflammation, and nonspecific manifestations, where the inflammatory process is not of the granulomatous type.
4
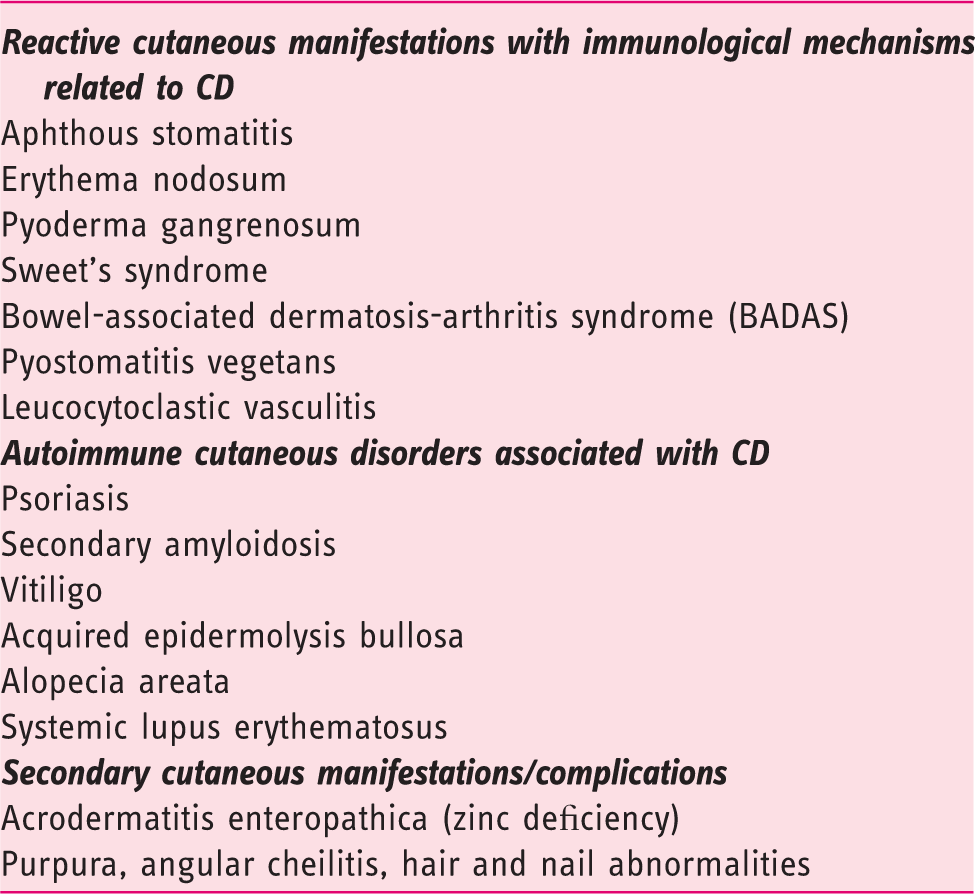
Nonspecific manifestations may be further differentiated into subtypes according to pathogenesis:
reactive cutaneous manifestations of CD with immunological mechanisms triggered by common antigens shared by gut bacteria and skin, cutaneous disorders or dermatosis associated with CD, secondary cutaneous manifestations due to complications of CD.
Specific cutaneous manifestations of Crohn’s disease

Non-specific cutaneous manifestations of Crohn’s disease (CD)
EN is the most common cutaneous manifestation of CD, affecting about 4%–15% of patients. Typical EN presents as painful, tender, warm nodules (1–5 cm in diameter), raised bluish-red subcutaneous lesions or plaques predominantly located on the anterior surface of the lower extremities. The clinical presentation is often associated with systemic symptoms, such as fever, chills or arthralgias. 6 The differential diagnosis may include metastatic skin cancer and histology may help ascertain the nature of the lesions. EN severity may parallel CD activity (90%) or may be independent of the underlying CD (10%).
Pyoderma gangrenosum (PG) and Sweet’s syndrome (SS) are two neutrophilic dermatoses, frequently associated with CD. The hallmark of these diseases is the accumulation of neutrophils in the skin and, rarely, in the internal organs. PG is a very debilitating chronic ulcerative skin disorder. The ulcers have sharply circumscribed and demarcated borders with a necrotic yellowish base (Figure 1). The lesions can be single or multiple, unilateral or bilateral, and may extend from several centimetres to the surface of an entire limb. PG often occurs on the extensor surface of the legs, but may appear anywhere.
5
SS is characterised by abrupt onset with fever, peripheral neutrophilia and leucocytosis. Cutaneous lesions consist of painful, tender, erythematous or purple papules or nodules that may coalesce into plaques, distributed in an asymmetrical fashion over the upper extremities, face and neck.
6
Pyoderma gangrenosum of the extensor aspect of the leg in a Crohn's disease patient.
Pyostomatitis vegetans is a rare cutaneous manifestation of IBD characterised by yellowish flat ulcerations on the oral and gingival mucosa, typically in the ‘snail tracks’ shape. 5
Malnutrition and/or malabsorption may be the cause of secondary cutaneous manifestations of CD such as purpura, angular cheilitis, hair and nail abnormalities. The most frequent is acrodermatitis enteropathica-like syndrome, due to zinc deficiency, that presents with eroded, crusted, sharply bordered erythematous patches, surrounded by vesicles or pustules, located at the extremities and peri-orificially. 7
Other skin alterations such as alopecia areata, psoriasis, vitiligo, or systemic lupus erythematosus (SLE) can be associated with CD but they are independent of the underlying disease and may simply reflect an increased susceptibility to autoimmunity. 3
The pathogenic mechanism underlying the development of cutaneous manifestations in CD patients is still unknown. Recent evidence from mouse models of intestinal inflammation suggests that T helper (Th)17-dependent interleukin (IL)-23 production is one of the major players in the pathogenesis of CD. 7 Because Th17 cells are involved in the pathogenesis of many autoimmune skin diseases, this might represent the mechanistic link between CD and cutaneous manifestations. 5 Moreover, neutrophil dysfunction, abnormal T-cell response, over-expression of pro-inflammatory cytokines such as IL-8, IL-16, IL-17, IL-23 and TNF-α, have been proposed as the possible pathogenic mechanism underlying neutrophilic dermatoses. 6
Skin lesions induced by anti-TNF therapy
An emerging problem in the course of CD is represented by the occurrence of skin lesions during anti-TNF therapy. Skin adverse events in patients treated with anti-TNF agents are classified as: a) local or systemic manifestations related to treatment such as diffused skin rash following drug administration or skin reaction at the injection site; b) skin infection; c) malignancy; d) autoimmune-related skin disease. 8
Anti-TNF agents, which are approved for the treatment of moderate to severe psoriasis, may paradoxically cause psoriasiform skin lesions in patients with IBD.
9
An incidence of psoriasiform lesions of 1.6%–8.8%, which is consistent with data derived from anti-TNF-treated patients with rheumatoid arthritis.7,10,11 has been reported. Psoriasiform lesions during anti-TNF therapy occur more frequently in patients with CD than in those with UC (i.e. 90%–96% vs 4%–10%, respectively).7,12 The main risk factors for developing psoriasiform skin lesions are: smoking (past or active), increased body mass index (BMI), female sex, familial history of inflammatory skin disease and short disease duration.
7
The most frequent localisation of psoriasiform lesions is hand palm or feet plant, scalp and flexures (Figure 2). The pathogenic mechanism of anti-TNF agents-related psoriasiform skin lesions is still an object of debate. Tillack et al. reported that psoriasiform lesions induced by anti-TNF therapy were characterised by infiltrates of IL-17/IL-22-expressing Th17 cells and interferon (IFN)-γ-expressing Th1 cells, the severity of lesions being correlated with the density of Th17 cell infiltrates. This suggests that Th1 and Th17 cells may play a pathogenic role in development of these lesions and indicates that anti-TNF-induced psoriasiform lesions and non-anti-TNF-related psoriasis may have a common pathogenic mechanism. In fact, in both conditions, an increased expression of the Th17-derived cytokines IL-17 and IL-22 has been demonstrated.7,13,14 Also, a role for over-production of IFN-α by plasmacytoid dendritic cells (pDCs) has been suggested.7,15 In fact, TNFα inhibits pDC maturation from haematopoietic progenitor cells and consequently inhibits IFN-α production.7,16 Therefore, anti-TNF treatment may result in unlimited IFNα production by pDCs, which might in turn favour the formation of psoriasiform lesions. In agreement with this hypothesis, Tillack et al. found increased IFNα protein expression in skin biopsy of patients with anti-TNF-associated psoriasiform lesions.
7
Other studies suggested that altered lymphocyte migration caused by anti-TNF therapy may also contribute to skin lesions through the expression of CXCR3 ligands which, by interacting with their receptor, regulate leucocyte trafficking.7,17,18 Finally, Scaldaferri et al. hypothesised that anti-TNF agents may induce a ‘patchy cutaneous’ immune suppression leading to the development of psoriasis-like lesions.
19
Palmar (a) and perianal (b) psoriasis in a Crohn's disease patient on anti-TNF therapy.
There are no clear guidelines for management of anti-TNF-induced psoriasiform lesions. Paradoxical psoriasis can be treated with topical corticosteroids, vitamin D analogues, phototherapy, methotrexate or cyclosporine, but it is occasionally refractory to conventional treatments.20,21 In the case of localised lesions, topical corticosteroids or vitamin D analogues are indicated. In the case of diffuse lesions, there is an indication for systemic treatment with steroids or methotrexate or cyclosporine. Discontinuation of anti-TNF therapy may be required in about 30% of patients with severe lesions or in those who do not respond to conventional therapy leading to an improvement of skin lesions in 24% to 88%. After the resolution of skin lesions, the reintroduction of anti-TNF therapy should be considered. If anti-TNF therapy does no longer represent an option, alternative therapies for IBD have to be considered. Some studies reported efficacy of ustekinumab, an anti-IL-12/IL-23 p40 antibody, in patients non-responsive to local therapy after stopping anti-TNF therapy. 7 Whether switching from one anti-TNF to another may have a positive impact on skin lesions is not completely clear. Tillack et al. 7 in a large prospective study found that in 21/434 (4.8%) patients on anti-TNF therapy who developed psoriasiform lesions the switching strategy resulted in no significant improvement. Afzali et al. 12 in a retrospective study including 1004 IBD patients on anti-TNF therapy found that 27 patients (i.e. 2.7%) developed psoriasiform skin lesions. In particular, skin lesions developed in eight of 620 (i.e. 1.3%) patients on infliximab, in 10/243 (i.e 4.1%) on adalimumab and in nine of 141 (i.e. 6.4%) on certolizumab. Of these 27 patients, six were managed by switching to another anti-TNF agent and four of these six patients showed a significant improvement in skin lesions. Therefore, therapeutic approach for paradoxical psoriasis must be discussed properly with patients because it may have a negative impact on the underlying intestinal disease and must be based on psoriasis severity, response to the standard therapy, and possibility of using alternative therapies for IBD.7,22
Anti-TNF therapy is associated with the development of skin lesions other than psoriasiform lesions with an incidence of approximately 18%. The most common non-psoriasiform skin disorders associated with anti-TNF therapy are infusion reactions to infliximab with skin erythema (5.8%), followed by viral skin infections (2.5%), eczematiform skin lesions (2.1%), xerosis cutis (2.1%) and bacterial skin infections (1.4%). 7 SLE is an uncommon phenomenon with most cases reported in rheumatological series with an incidence of about 1%. Ninety-four per cent of the cases responded to interruption of therapy.23,24
Cutaneous malignancies have also been reported in patients treated with anti-TNF agents or thiopurines. Askling et al., in a meta-analysis including 74 randomised controlled trials using anti-TNF therapy with over 22,000 patients reported a relative risk of NMSC (Figure 3) associated with all anti-TNF monotherapies equal to 2.02 (95% confidence interval (CI) 1.11–3.95).
25
Data from the Therapy, Resource, Evaluation, and Assessment Tool (TREAT) registry including 6273 patients, 3420 treated with anti-TNF agents and 2853 non-anti-TNF-treated, with a mean follow-up/patient of 5.2 years, show that there is no statistically significant difference in the incidence of NMSC between patients treated with anti-TNF and those treated differently (0.16 vs 0.18 events per 100 patient-years, respectively).
26
Biancone et al., showed that patients treated with anti-TNF agents have an increased risk of lymphoma and NMSC.
27
However, it has been questioned whether IBD by itself may carry an increased risk of NMSC. In this respect, Long et al. demonstrated that IBD patients have an increased risk of NMSC independently of anti-TNF therapy compared to non-IBD controls with an incidence rate ratio (IRR) equal to 1.64 (95% CI 1.51–1.78). Moreover, persistent use (>365 days) of both thiopurine (6 MP/azathioprine) and anti-TNF is associated to an increased risk of developing NMSC with an adjusted odds ratio (OR) equal to 2.18 (95% CI 1.07–4.46).
28
More recently, Long et al.
29
in a retrospective case-control study of administrative data including108,579 patients with IBD (50,920 CD, 56,390 ulcerative colitis and 1269 IBD of undefined type) demonstrated that IBD was associated with an increased incidence of MM (IRR, 1.29; 95% CI, 1.09–1.53). Risk was greatest among individuals with CD (IRR, 1.45; 95% CI, 1.13–1.85; adjusted hazard ratio (HR), 1.28; 95% CI, 1.00–1.64). The incidence of NMSC also increased among patients with IBD (IRR, 1.46; 95% CI, 1.40–1.53) and was greatest among those with CD (IRR, 1.64; 95% CI, 1.54–1.74). In this study, therapy with anti-TNF appeared to increase the risk of MM (OR 1.88; 95% CI, 1.08–3.29). Patients who had been treated with thiopurines had an increased risk of NMSC (OR, 1.85; 95% CI, 1.66–2.05).
25
Therefore, based on this study, use of biologics increases the risk of MM whereas the use of thiopurines increases the risk of NMSC. However, the absolute risk of developing MM or NMSC in IBD patients is as low as 57/100,000 person-years and 912/100,000 person-years, respectively. Therefore, taking into account the benefits of anti-TNF agents or thiopurines, the mildly increased relative risk of developing skin malignancies should not deter the use of these efficacious therapeutical agents. Avoidance of the sun, use of sun-protective agents or clothing may represent a valuable option for primary prevention of both MM and NMSC.
Bowen's disease (i.e. squamous cell carcinoma in situ) on the extensor aspect of the arm in a Crohn's disease patient on anti-TNF therapy.
While thiopurine-associated increase in the risk of NMSC may be linked to the activation of thiopurine into a mutagenic DNA-reactive moiety after exposure to ultraviolet light, 30 the mechanism whereby anti-TNF agents may increase the risk of skin malignancies is not fully understood. However, an alteration in immune surveillance due to anti-TNF may contribute.24,25 TNF-α has a complex effect on carcinogenesis and, depending on doses, promotes cell proliferation and thus tumour growth or induces apoptosis and inhibits angiogenesis, thus suppressing the development of a number of cancers.31–33 No causal association between anti-TNF agents and cancer has been demonstrated so far and caution is required when the available data are interpreted, because the follow-up of IBD patients treated with anti-TNF drugs is quite short. Multicentre studies in large populations with long-term follow-up are needed to address the issue of anti-TNF therapy and cancer development.
Summary and conclusion
Cutaneous lesions are the most common extra-intestinal manifestations associated with CD, with almost one-third of CD patients developing skin lesions during the course of their disease. The most frequent skin lesions are represented by EN and PG. 34 Neither of these two skin diseases is found exclusively in CD, and the finding of one or the other lesion is not specific for either major form of IBD. 34 The clinical course of these cutaneous manifestations often parallels the course of the underlying intestinal disease and generally improves with therapy.
An emerging problem is represented by the occurrence of skin lesions during anti-TNF therapy, psoriasiform skin lesions being the most common anti-TNF-related skin disease. These lesions generally respond to conventional therapy, but, in a number of cases, discontinuation of biologic therapy is needed and this may affect the course of the underlying intestinal disease. Switching from one anti-TNF to another is not always effective, but could be worth trying.
One major concern associated with the increased use of anti-TNF agents is the occurrence of MM. 35 However, a causal relationship between ant-TNF therapy and development and progression or reactivation of cutaneous malignancy has not yet been fully ascertained. Further long-term controlled clinical trials and registries are required to investigate this potentially serious association.36,37
In conclusion, this review strengthens once again the concept that CD needs a multidisciplinary approach and that, in particular, a careful medical history and assessment for dermatologic conditions should be carried out before starting any biologic therapy.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.