
Abstract
Background
Peroral endoscopic esophageal myotomy (POEM) represents a less invasive alternative, as compared with conventional laparoscopic Heller myotomy for treating achalasia patients. In the last years, a number of prospective and retrospective experiences with POEM use for achalasia have been published.
Methods
Relevant publications in which patients affected by achalasia underwent POEM treatment were identified by PubMed databases for the period 2010 – 2013. From each study, we extracted the number and type of major complications (defined as those requiring any additional medical or surgical intervention). Data were pooled, using random-effects models. Heterogeneity among studies was assessed by using Cochran's Q and the I2 statistic.
Results
We found 16 studies that provided data on 551 patients. The median surveillance period was 6 months (range: 3–12). The median of mean POEM duration was 156 minutes (range: 42–112). Median myotomy length was 10 cm (range: 6–14). Technical and clinical success were reported in 97% (95% CI: 94–98%) and 93% (407/428; 95% CI: 90–95%). No heterogeneity (I2 = 0%) or publication bias was present in both estimates. When limiting the analysis only to adverse events that require medical or surgical interventions, major adverse events occurred in 14% (95% CI: 11–17%); however, only one patient needed post-POEM surgery (0.2%; 95% CI: 0–0.5%).
Conclusions
POEM appeared to be a highly feasible and effective endoscopic treatment for achalasia. Despite POEM being apparently associated with relatively high morbidity, most patients are successfully managed conservatively, so that POEM appears as a very safe procedure; however, POEM should only be performed in centers able to treat POEM complications, such as pneumothorax or pneumoperitoneum.
Keywords
Introduction
Achalasia is a rare condition, of unknow causes, with an estimated annual incidence of one per 100,000 persons, characterised by a functional obstruction of the esophagus that is caused by failed relaxation of the lower esophageal sphincter (LES), in combination with absent peristalsis of the distal esophagus. 1
Patients mainly present with symptoms such as dysphagia for both solids and liquids, regurgitation of undigested food, respiratory complications, chest pain and weight loss. These symptoms result from impaired peristalsis and deficient or absent relaxation of the LES, which leads to stasis of food in the esophagus. 2 Treatment aims to disrupt or dissect the LES, to enhance transport of the bolus into the stomach.
In the modern era of achalasia treatment, disruption of the LES is best accomplished by pneumatic dilation, using Rigiflex balloons or laparoscopic Heller myotomy (LHM), and less effectively, by pharmacological-type agents, such as Clostridium botulinum toxin injection or calcium channel blockers.3–7
An innovative endoscopic method for dissection of the LES, using a needle-knife to cut the muscular fibers from the lumenal side, was first described by Ortega et al. 8 in 1980. Two decades later, Pasricha et al. 9 first described the feasibility of an endoscopic submucosal esophageal myotomy in a survival animal model. Finally, Inoue et al. 10 successfully performed the first peroral endoscopic esophageal myotomy (POEM) in humans, which appeared to be substantially less invasive, when compared with LHM. Following this preliminary experience, there have been published in the last years a number of prospective and retrospective experiences with POEM for achalasia, with controversial data in terms of adverse events and outcome.
The aim of this systematic review was to pool the results of POEM procedures, in terms of efficacy and safety, and also address relevant clinical and technical issues.
Methods
The methods of our analysis and inclusion criteria were based on Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) recommendations. 11
Eligibility criteria
We considered all clinical studies for the period from 2010 (i.e. when POEM was first applied to human subjects) to December 2013, in which patients affected by achalasia underwent POEM treatment. Animal studies were excluded. If there was any suspicion of cohort overlap between studies, only the most recent study was considered for inclusion.
Information sources
A literature search was performed on December 2013. Relevant publications were identified by PubMed. Abstracts were not included, because they were unlikely to provide all the necessary details, in terms of adverse events. Additional references were located through searching the bibliographies of related papers. Our search was limited to papers written in English. Case series with less than or equal to three patients were also excluded. The medical terms ‘POEM’ and ‘achalasia’ were used in the search, with the following algorithm: ‘POEM[All Fields] OR “peroral endoscopic myotomy” [All Fields]) AND (“esophageal achalasia” [MeSH Terms] OR (“esophageal” [All Fields] AND “achalasia” [All Fields]) OR “esophageal achalasia “[All Fields] OR “achalasia” [All Fields]’.
Study selection
Titles and abstracts of papers were screened by two reviewers. Any disagreements were resolved through discussion. Studies (the full report of the study) were independently pre-screened for relevance by two reviewers. Any disagreements were resolved through discussion. Data were extracted from relevant studies by one reviewer and checked by a second reviewer. Data from the included studies were extracted into tables. Any disagreements were resolved through discussion with a third reviewer. Information relating to the methodological quality of each study was also recorded.
Data collection process and list of items
From each report, reviewers independently abstracted:
Year of publication; Country where the study was performed; Single- or multi-center study; Study design; Population characteristics; Number of patients included; Number of patients eligible; Mean age distribution; Sex distribution; Technical/clinical success; Rate of post-POEM esophagitis; Duration of follow up; and Rate of adverse events requiring medical/surgical treatment (self-limiting pneumo-mediastinum/-peritoneum not requiring any drainage/treatment was not considered as an adverse event).
Risk of bias in individual studies
Information was recorded relating to the methodological quality of each study. Quality assessment was performed using the STROBE checklist for observational studies. 12 More information can be found in Appendix 1.
Summary measures
The primary end-points of this systematic review were to address the following:
1. What are the feasibility and clinical success (defined as clinically-relevant improvement of dysphagia) rates of POEM? 2. What is the risk of clinically-relevant adverse events, after POEM?
Planned methods of analysis
Data on feasibility, efficacy and safety were extracted where possible. The prevalence of the main outcome variables in each study was combined, to yield a pooled prevalence with a 95% CI for all studies. Data were pooled using random-effects models, to generate a more conservative estimate of the prevalence. Heterogeneity among studies was assessed by using Cochran's Q (reported with a χ2-value and p-value) and the I2 statistic, the latter describing the percentage of variation across studies that is due to heterogeneity, rather than chance, and presented with a 95% CI. Publication bias was measured using Egger’s regression. Statistical analyses were carried out using the R statistical software package, version 2.15.2. 13 P < 0.05 was considered statistically significant.
Results
Study selection
A flow diagram of this systematic review, with the number of papers retrieved, included and excluded, as well as the reasons for exclusion, is shown in Figure 1. In summary, 80 studies were identified by the included databases. After reviewing the title and abstract, 32 articles were retrieved as full text. Of these, 16 studies matched the inclusion criteria for our analysis. The reasons for exclusion of full-text studies are given in Appendix 2.
Flow chart of the systematic review.
Characteristics of the included studies
Study and population characteristics of the included studies

Group A: full-thickness myotomy; Group B: circular muscle myotomy
BMI: body mass index; NA: no done
Participants
Overall, there were 551 subjects included in the selected series. Despite that there was some heterogeneity in the distribution of gender among the series, overall, 48% of the enrolled subjects were female. The median of the mean ages from all studies was 44 years (range: 32–64 years). Body mass index (BMI) was available only in four series (median 26; range: 25–27). All but three studies adopted a predefined score to assess the severity of dysphagia, being the Eckardt score in most of the cases.
Interventions
Technical and clinical characteristics of POEM in the included series
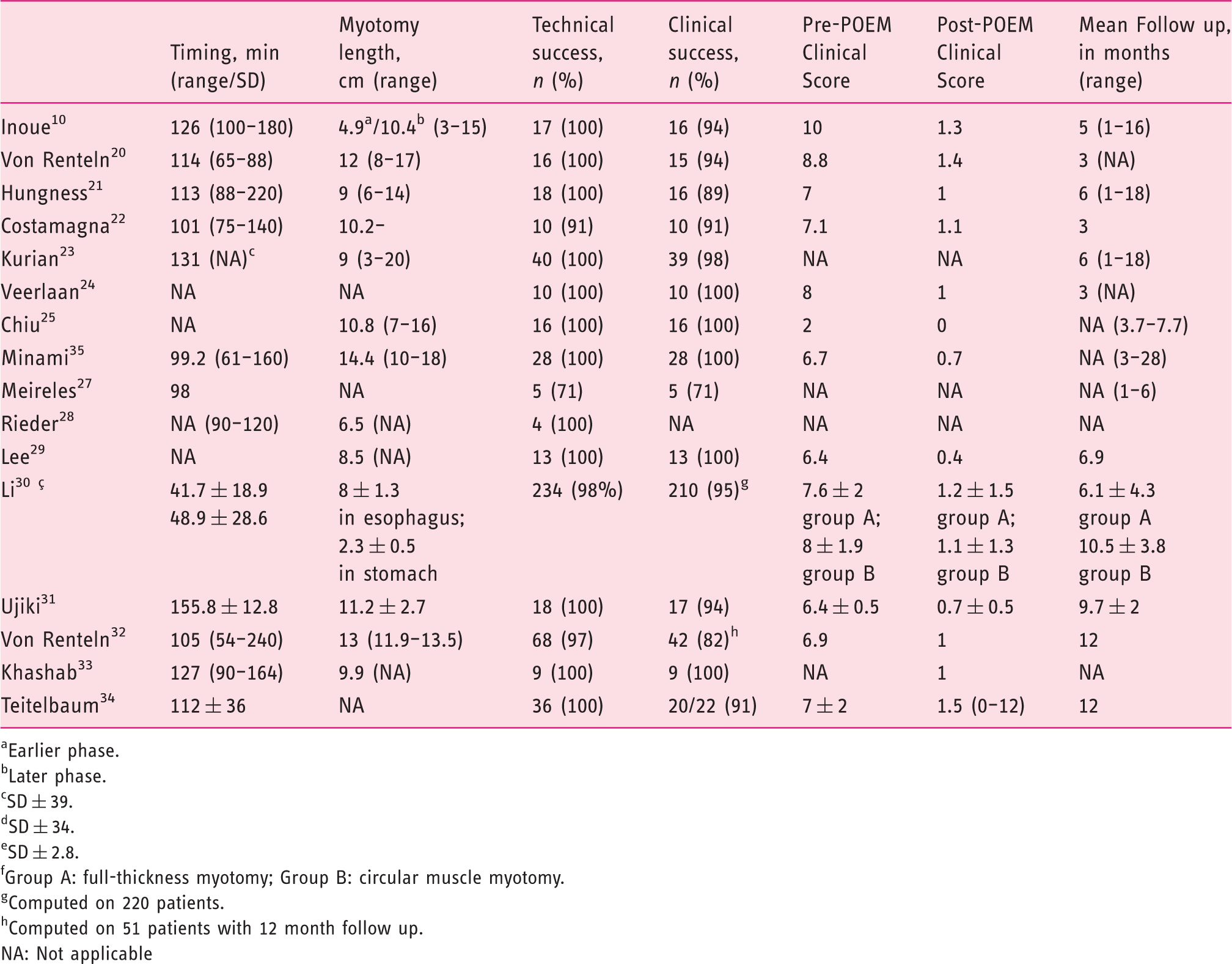
Earlier phase.
Later phase.
SD ± 39.
SD ± 34.
SD ± 2.8.
Group A: full-thickness myotomy; Group B: circular muscle myotomy.
Computed on 220 patients.
Computed on 51 patients with 12 month follow up.
NA: Not applicable
Outcomes
Efficacy
Technical feasibility was reported in all the series. Across the studies, the prevalence of successfully-performed procedures varied from 71% to 100% (Figure 2). The pooled prevalence was 97% (95% CI: 94–98%). As is shown in Figure 2, no significant heterogeneity was detected in the analysis of technical feasibility (χ2 = 13.59, p = 0.557, I2 = 0%; 95% CI 0–47.3%). Publication bias was not statistically significant (Egger’s regression: bias = – 0.27; standard error (SE) = 0.6; p = 0.697).
Forest plot of technical success rates and pooled estimates.
The clinical success rate was reported by all but one series, which specificially looked only at adverse events. Across the studies, POEM was associated with a favorable clinical outcome in 466 out of 493 patients. The pooled rate of clinical success prevalence was 93% (95% CIs: 90–95%), with no statistically significant heterogeneity among studies (χ2 = 13.86, p = 0.460, I2 = 0%; 95% CI 0–53%), as is shown in Figure 3. Publication bias was not statistically significant (Egger’s regression: bias = 0.64; SE = 0.5; p = 0.189). The mean of the dysphagia scores was reduced from 7 to 1 (p < 0.001; Student test) in the series in which the Eckardt score was used (all but two). The median follow-up was 6 months (range: 3–12).
Forest plot: clinical success rates and pooled estimates.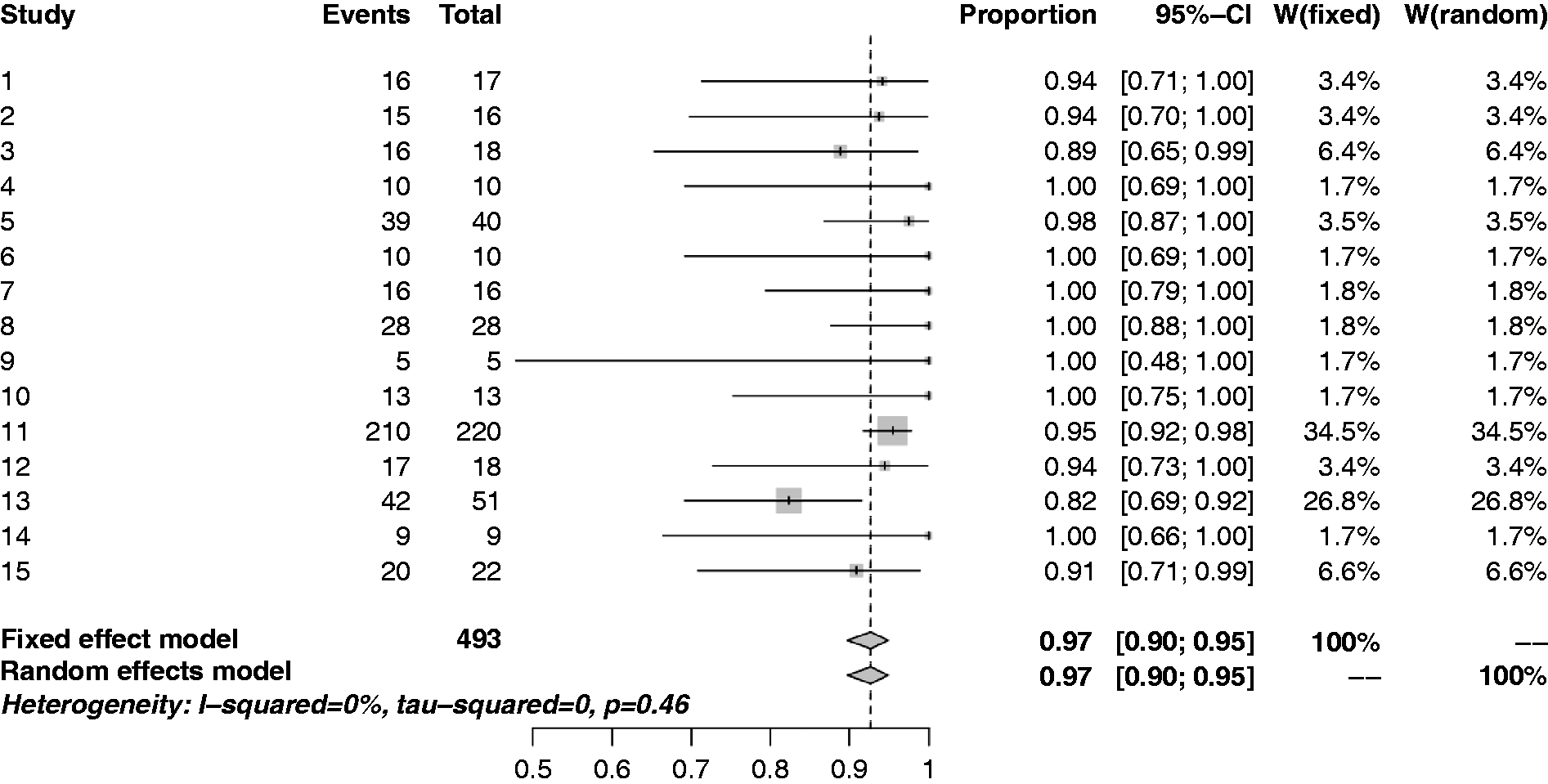
Safety
Post-POEM complications in the collected studies

Pneumoperitoneum treated with puncture (n = 1).
Pneumoperitoneum treated with puncture (n = 8). Also perforation treated with endoscopic clips (n = 1) and cardiac ulcer treated conservatively (n = 1).
Pneumoperitoneum treated with needle decompression (n = 7) and perforation treated with laparoscopy (n = 1).
Intraoperative mucosal perforation treated with clips.
Gastric/esophageal intraoperative perforation treated with clips (n = 19), pneumoperitoneum treated with needle decompression (n = 7), 1 pneumothorax treated with needle decompression (n = 1), post-operative hematemesis (n = 1), and leakage treated endoscopically with clips (n = 1).
Pneumonia treated with antibiotics and bronchial lavage.
Bleeding (n = 2), EJG perforation between submucosal tunnel (n = 1) and esophageal lumen treated with clip (n = 1).
Intraoperative pneumoperitoneum treated with Verres needle decompression (n = 2); intraoperative subcutaneous enphysema plus pneumothorax, treated with thoracic drainage (n = 1); postoperative thoracic drainage (n = 14); pleural effusion (n = 2); fever ≥ 38° (n = 6); submucosal tunnel infection (n = 1); epileptic seizure (n = 1); and bleeding in submucosal tunnel (unspecified if treated or not) (n = 1).
Pneumoperitoneum treated with Verres decompression (n = 3).
Mucosal injury through electrocautery or laceration (n = 3); bleeding requiring endoscopic hemostasis (n = 1); and mediastinal hematoma requiring hospital readmission (n = 1).
Group A: full-thickness myotomy; Group B: circular muscle myotomy.
Risk of bias in individual studies
In most of the studies, it was unclear whether enrollment was actually consecutive, so that a selection bias cannot be completely excluded. The efficacy of POEM was mainly evaluated by a complex reference standard, such as post-POEM cardiac relaxation, the regression of dysphagia and the clinical scores. At least in theory, the assessment of these variables should be independent from the POEM procedure, although all of the involved operators whom were not blinded to the procedure performed. See Appendix 1 and Appendix 3.
Discussion
According to our systematic review, POEM is a highly feasible, effective and safe procedure to treat achalasia. In a pooled population of 551 patients, we showed a technical feasibility of 97%. Moreover, in a subgroup of patients, we showed a 93% success rate, whilst the risk of adverse events requiring medical/surgical treatments was limited to 14% of the cases, resulting in surgery only in 0.2% of the initial population. Our results are relevant for the following reasons:
1. First, despite that any single study may appear underpowered to provide a reliable estimate of POEM efficacy, our pooled synthesis is associated with a limited 95% CI, showing a high degree of certainty on its precise estimate. 2. We did not detect any degree of heterogeneity in the efficacy estimate, showing the generalizability and reproducibility of the procedure. Of note, the included studies came from different continents, yet no particular difference between Asia and Western endoscopy appeared. 3. Despite no direct comparison with LHM being available, the success rate we showed is so high that it is unlikely that any study will be able to detect a statistically significant difference between the two procedures. In particular, the long-term LHM success rate appeared to range between 73% and 92%.14–16 4. We showed that there was quite a high degree of homogeneity in the technical details, such as the length of myotomy and timing of the procedure, so that the technique appears to be already quite standardized. 5. We showed that, on the one hand, POEM operators must be aware of adverse events that are not typical of non-POEM endoscopy, such as hypertensive pneumomedistinum and intra-mediastinum bleeding; but, on the other hand, such adverse events may be easly treated with decompressive actions, resulting at best in a short prolongation of hospital stay; however, surgeons with extensive experience in esophageal surgery should always be promptly available to treat POEM adverse events. 6. Despite that there are no comparative studies, POEM would appear as a more rational approach for achalasia, because it allows a more radical treatment of the hypertensive LES without the need of dilation repetition. 7. In our systematic review, there was 13% of post-POEM esophagitis described. Such a rate would not appear higher than the 21% reported in a large randomized trial with LHM.
3
This favorable rate, despite the lack of an anti-reflux plasty, could be related to the conservative nature of POEM, which does not imply the mobilization of the gastro-esophageal junction structures. Differently from LHM, POEM also allows for a more selective dissection of cardial fibers.
There are limitations in our analyses. First, in most series, a selection bias could not be excluded, so that POEM could be less successful when applied to unselected achalasia patients (i.e. those with a very dilated esophagus). Second, there were different criteria to measure the clinical degree of dysphagia or the adverse events rates. However, on the one hand, there was such a dramatic improvement in any score that it is unlikely that the choice of such scores may have affected the results of our analysis; and on the other hand, the assessment of post-POEM surgery is a very solid surrogate for measuring POEM safety. Third, no long-term follow-up results are yet available, because POEM is a recent novel technique. For instance, the short-term success of LHM was substantially higher than its long-term success rate.17–19 The same dynamic cannot yet be excluded for POEM.
In conclusion, we showed that POEM is a highly effective and safe procedure, when performed in a dedicated setting, and it also appeared to be reproducible and generalizable in different continents; however, when considering the observational type of studies included, we believe further data from randomized studies, as well as on the long-term outcome, are needed.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Conflict of interest
The authors report there are no conflicts of interest.
Appendix 1.
Assessment of risk of individual bias
Potential bias et al.
1. Was the spectrum of patients representative of the patients who will receive the test in practice?
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
2. Were selection criteria clearly described?
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
3. Is the reference standard likely to correctly classify the target condition?
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
4. Is the time period between reference standard and index test short enough to be reasonably sure that the target condition did not change between the two tests?
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
5. Did the whole sample or a random selection of the sample, receive verification using a reference standard of diagnosis?
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
6. Did patients receive the same reference standard regardless of the index test result?
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
7. Was the reference standard independent of the index test i.e. the index test did not form part of the reference standard?
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
8. Was the execution of the index test described in sufficient detail to permit replication of the test?
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
9. Was the execution of the reference standard described in sufficient detail to permit its replication?
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
10. Were the index test results interpreted without knowledge of the results of the reference standard?
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
11. Were the reference standard results interpreted without knowledge of the results of the index test?
N
N
N
N
N
N
N
N
N
N
N
N
N
N
N
N
12. Were the same clinical data available when test results were interpreted as would be available when the test is used in practice?
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
Y
13. Were withdrawals from the study explained?
Y
Y
N
N
Y
Y
Y
N
Y
N
N
N
N
Y
N
Y
Appendix 2.
Articles excluded and main reasons
Familiari
36
≤3 cases
Kurian
37
≤3 cases
Muller
38
Non-pertinent
Saxena
39
≤3 cases
Stavropoulos
40
Survey
Tietelbaum
41
Partial duplication
Tietelbaum
42
No clinical outcome
Zhou
43
Partial duplication
Cai
44
Partial duplication
Ren
45
Partial duplication
Minami
35
Partial duplication
Bhayani
46
Partial duplication
Swanstrom
47
Partial duplication
Swanstrom
48
Partial duplication
Sharata
49
Partial duplication
Onimaru
50
Population non representative
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.