
Abstract
Background
Management of Crohn’s disease (CD) is a clinical challenge. In terms of an evidence-based approach, clinical guidelines help to deal with this challenge. However, little is known about guideline adherence concerning the management of CD in Germany.
Objective
To survey German gastroenterologists with regards to their guideline adherence in daily clinical care.
Method
A web-based national survey was conducted among German gastroenterologists.
Results
A total of 175 inflammatory bowel disease (IBD) practitioners responded to the survey. Overall, in the different clinical situations covered in the questionnaire guideline adherence is good. However, the 5-aminosalicylic acid (5-ASA) prescribing habits represent a striking exception. About 10–36% use 5-ASA as mono-therapy in CD, depending on the clinical scenario. Predominantly it is used in mild CD and in colonic involvement. To maintain a surgically achieved remission, therapeutic decisions broadly rely on individual approaches with azathioprine and 5-ASA being used by about 30% of the respondents. Cessation of smoking as a “therapeutic” strategy of maintenance therapy is used by only half of the surveyed physicians.
Conclusion
Amongst German IBD practitioners, the guideline adherence is good overall. Reflecting ongoing uncertainty about the efficacy of mesalazine, its use in Crohn’s disease is still heterogeneous.
Keywords
Introduction
Inflammatory bowel diseases (IBD), i.e. Crohn’s disease (CD) and ulcerative colitis (UC), affect between 320,000 and 470,000 patients in Germany.1,2 Many aspects of IBD are a clinical challenge, even for experienced gastroenterologists. Numerous therapeutic decisions are required to avoid CD complications and to manage every patient’s individual disease. Additionally, there is a tremendous economic significance of therapy costs, especially for biologicals and work time lost due to disease activity.1,2 Therefore clinical decision making should be based on the best available scientific and clinical data.
As a limiting problem, clinical studies do not necessarily represent the average patient population in IBD. 3 In daily clinical care, both over-treatment and also potentially hazardous under-treatment are common problems. A US study from 2005 revealed that about 11% of IBD patients receive a potentially harmful treatment that is not in line with clinical guidelines.4,5 However, decision making in general is influenced by subjective beliefs and personal experiences which may bias medical decisions.6–8
Therefore, there may be a considerable gap between scientific (study-based) knowledge and its implementation in daily patient care. Lack of time or knowledge and negative attitudes towards evidence based medicine are accounted for this phenomenon. 9 Based on medical and socio-economic data it has been estimated that about 20% of German IBD patients may not be treated according to the clinical guidelines provided by the German Society of Gastroenterology (DGVS) or the European Crohn’s and Colitis Organisation (ECCO). 10 We therefore conducted a nationwide survey among German gastroenterologists dealing with CD patients, to address their views on the management of CD. With a second focus we assessed aspects of the use of 5-aminosalicylic acid (5-ASA) in CD, which is still controversial. 11
Materials and methods
A standardized questionnaire consisting of 21 multiple-choice questions (in parts with possibility to note individual answers) and two open questions was developed (see Supplemental Material 1). On the one hand, questions were designed to analyze therapeutic decisions of IBD practitioners in general and on the other hand with special attention on the use of 5-ASA in different clinical settings of CD. The questionnaire was presented at the professional survey website www.surveymonkey.com (anonymized replies). Statistical analysis was performed with the graphical and analytical features of www.surveymonkey.com, Microsoft Office, and GraphPad Prism (GraphPad Software, La Jolla, CA, version 5.04). Proportions were expressed as percentages of respondents.
Between July and December 2013, invitations to participate were sent by email to several organizations of German gastroenterologists: “Arbeitsgemeinschaft leitender gastroenterologischer Krankenhausärzte (ALGK),” “Berufsverband Niedergelassener Gastroenterologen Deutschlands (bng),” “Kompetenznetz chronisch entzündliche Darmerkrankungen e.V.,” and “Deutsche Arbeitsgemeinschaft chronisch entzündliche Darmerkrankungen (DACED).” Furthermore, a survey web-link was integrated in the July 2013 online newsletter of the “Deutsche Gesellschaft für Verdauungs- und Stoffwechselerkrankungen (DGVS).”
The aim of this approach was to motivate every IBD-interested gastroenterologist in Germany with an exposed position to deal with IBD patients. No reminder emails were sent to any of the above-mentioned groups.
Results
Response rate and characteristics of respondents
175 physicians responded to the survey. With our survey approach it is not possible to give an exact response rate, as invitations to participate were sent by email to several organizations of German gastroenterologists (see above) and we are not aware of the exact number of the emails sent. As about 2850 gastroenterologist are registered in Germany, 12 the response rate is <10%. Therefore, the results must be interpreted as a survey of IBD-experienced and interested physicians (see explanation below), rather than being representative for all German gastroenterologists.
144 (out of 175 respondents) answered every question, whereas 29 skipped between 1–3 questions. Two respondents skipped 5–7 questions. Therefore, the detailed response rate for every single question will be depicted separately in the following figures. The vast majority of the respondents were gastroenterologists in private practice (123/175; 70.3%) or in a hospital (43/175 (24.6%)) (Figure 1(b)). The remaining participants were general practitioners (1%) or gastroenterology resident physicians (4%). Ninety-one percent (160/175) of the respondents were 41 years or older. 49.7% (86/173) treat >31 CD patients per quarter and 24.6% (43/173) treat between 16–30 patients (Figure 1(a)). Physicians treating more than 20 IBD patients per quarter (notably UC and CD) are accepted as IBD experienced.1,2 They represent at least 50–75% of this study. Therefore, most participants seem to have a considerable experience in treating IBD patients.
Characteristics of respondents.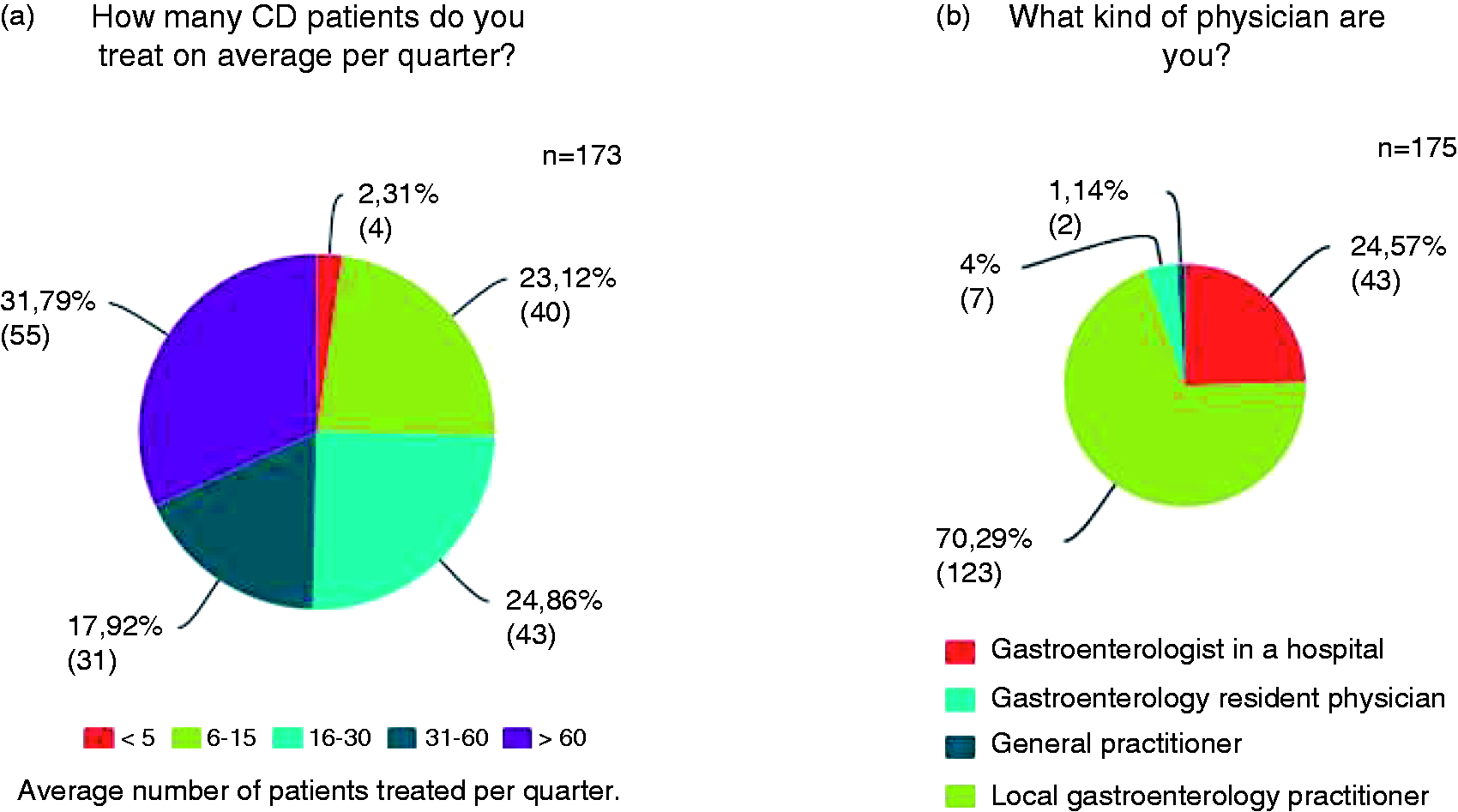
Management of Crohn’s disease in different clinical situations
Management of CD – induction therapy
One aim of this survey was to get an overview about the therapeutic decisions of the respondents regarding defined phenotypes of CD (mild to moderate ileal, colonic, or ileo-colonic disease). For this reason we designed three questions concerning the induction therapy for initially diagnosed CD.
For isolated ileal CD, 82.9% (145/175) of the physicians consider budesonide as the best treatment option (Figure 2(a)), 9.7% (17/175) use 5-ASA in this clinical situation, combined with systemic steroids (n = 6) or without steroids (n = 11), whereas 5.7% (10/175; defined as “others” in Figure 2(a)) propose either a combination of 5-ASA and budesonide or would start a 5-ASA-mono-therapy with the option to escalate therapy (e.g. additional budesonide or systemic steroids) if needed. Only 1.7% (3/175) would use a systemic steroid therapy with or without azathioprine in this clinical setting.
Management of induction therapy in CD.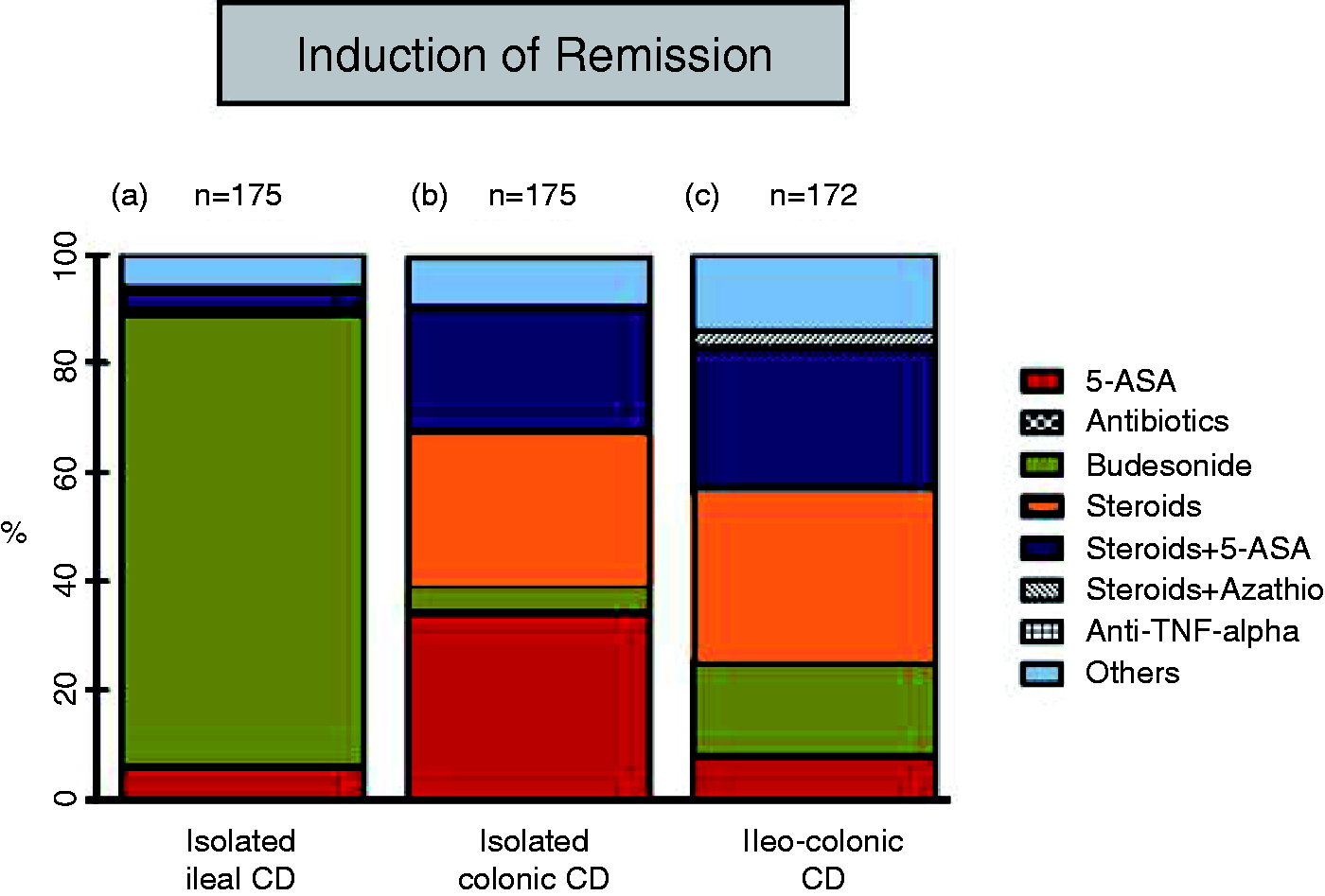
Asking for the induction therapy of an isolated colonic disease, 34.3% (60/175) preferred a mono-therapy with 5-ASA and 23.4% (41/175) use 5-ASA in combination with systemic steroids (Figure 2(b)). Therefore, about 57.7% of the physicians use a 5-ASA containing regimen in colonic CD. The second highest rated therapy are systemic steroids (about 27.4% (48/175)), whereas only 5.1% (9/175) use budesonide in this context. Less than 1% (1/175) would initiate azathioprine combined with steroids in the first line. Nine percent (16/175; defined as “others” in Figure 2(b)) consider different drug combinations as best choice, most prominently the combination of 5-ASA and budesonide. These respondents stressed that sulfasalazine might be effective. They also stated that topical-applied 5-ASA or topical steroids should be considered as potential drugs in colonic CD, combined with any other therapy.
In the setting of ileo-colonic CD, 32% (55/172) use systemic steroids, about 25.6% (44/172) recommend systemic steroids combined with 5-ASA, and 8.1% (14/172) would prescribe 5-ASA alone (Figure 2(c)). Therefore, about 34% of the respondents use 5-ASA combined or alone in this setting. About 16.9% (29/172) use budesonide alone and 3.5% (6/172) prescribe systemic steroids in combination with azathioprine. Fourteen percent (24/172) propose other therapeutic combinations, most of them (19/172) would treat their patients with 5-ASA and budesonide.
Without signs of infection none of the respondents would use antibiotics as mono-therapy for newly diagnosed CD in the clinical subgroups mentioned above. Also, none of the respondents would use anti-TNF-antibodies in the first line (Figure 2).
Management of CD – maintenance therapy
We further assessed which type of therapy is chosen to maintain a medically achieved remission in CD. At this type of questions it was allowed to pick more than one answer. We therefore present the percentages in terms of how often one alternative was mentioned by all respondents, although some respondents stated more than one answer.
In the case of isolated ileal disease, 41.9% (72/172) recommend a “watch and wait” strategy and 50.6% (87/172) underlined advising patients to stop smoking, in addition to “watch and wait” (Figure 3(a)). 5-ASA or budesonide would be administered by about 13% of the respondents (each drug), whereas 7.6% (13/172) directly initiate azathioprine/6-mercaptopurine as maintenance therapy.
Management of maintenance therapy in CD. For these questions it was allowed to pick more than one answer. We therefore present the percentages in terms of how often one alternative was picked by all respondents, albeit some respondents stated more than one answer.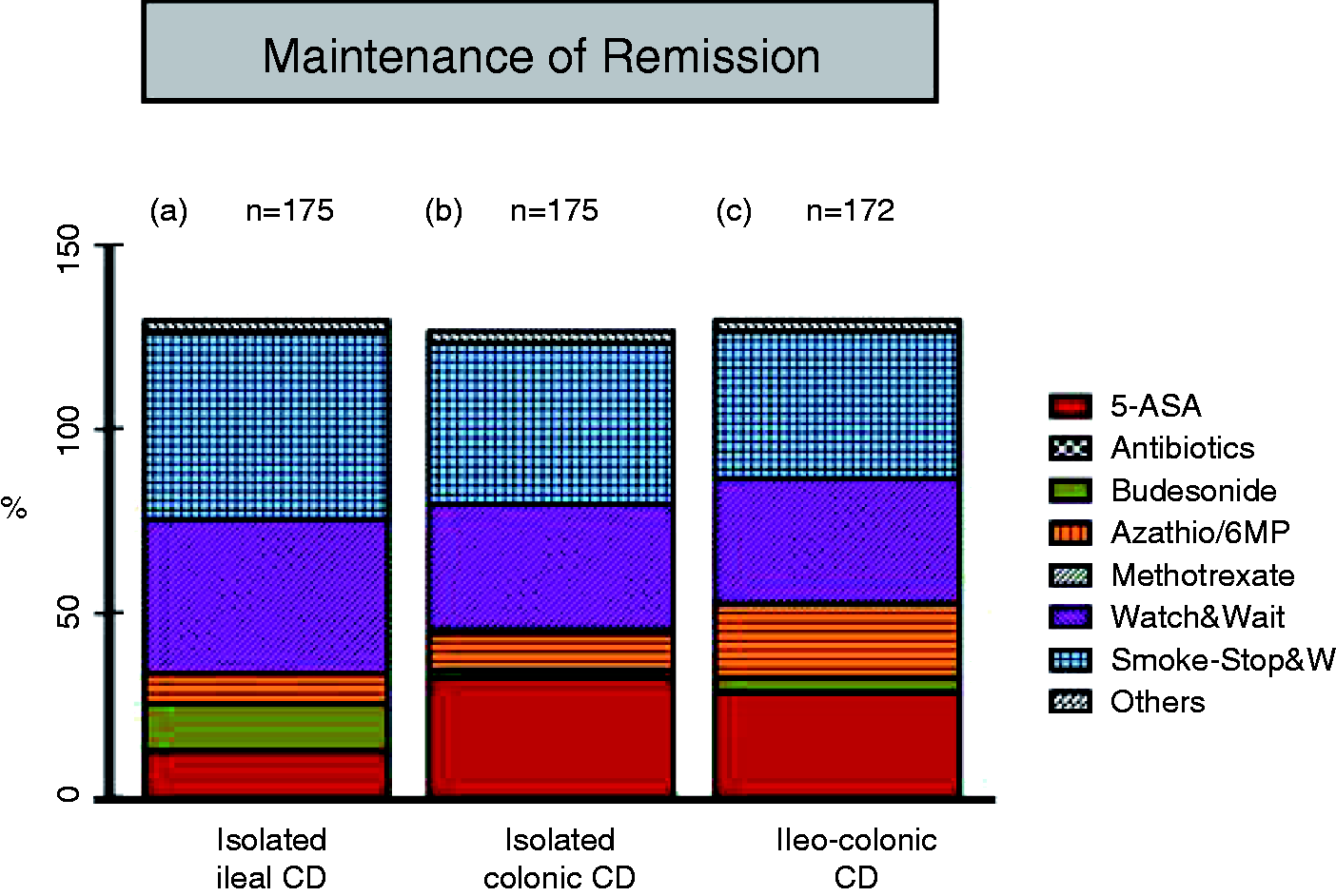
In colonic CD, 33.9% (59/174) voted for “watch and wait” and 44.2% (77/174) underlined the need to stop smoking. However, 32.8% (57/174) advise their patients to take 5-ASA as maintenance therapy and about 9.8% (17/174) would already start a therapy with azathioprine/6-mercaptopurine (Figure 3(b)). To maintain remission in ileo-colonic CD, 33.9% (58/171) choose a “watch and wait” strategy and 39.8% (68/171) additionally underline the need to stop smoking (Figure 3(c)). About 28.7% (49/171) recommend 5-ASA and 19.9% (34/171) would administer azathioprine/6-mercaptopurine.
In the post-surgical setting, most of the respondents try to maintain surgically achieved remission by administration of azathioprine (36.5%; 61/167). In second position (25.1% (42/167)) 5-ASA was mentioned (Figure 4) whereas 20.3% (34/167) recommend a “watch and wait” strategy without any therapeutic intervention. About 4% (in each case) would prescribe metronidazole (7/167) or budesonide (6/167). About 9.6% (16/167) proposed that this decision depends on prior therapies and disease history and only 3.6% (6/167) would perform an endoscopic examination 3–6 months after resection to assess the necessity of further therapeutic interventions.
Practices to maintain surgically achieved remission in CD.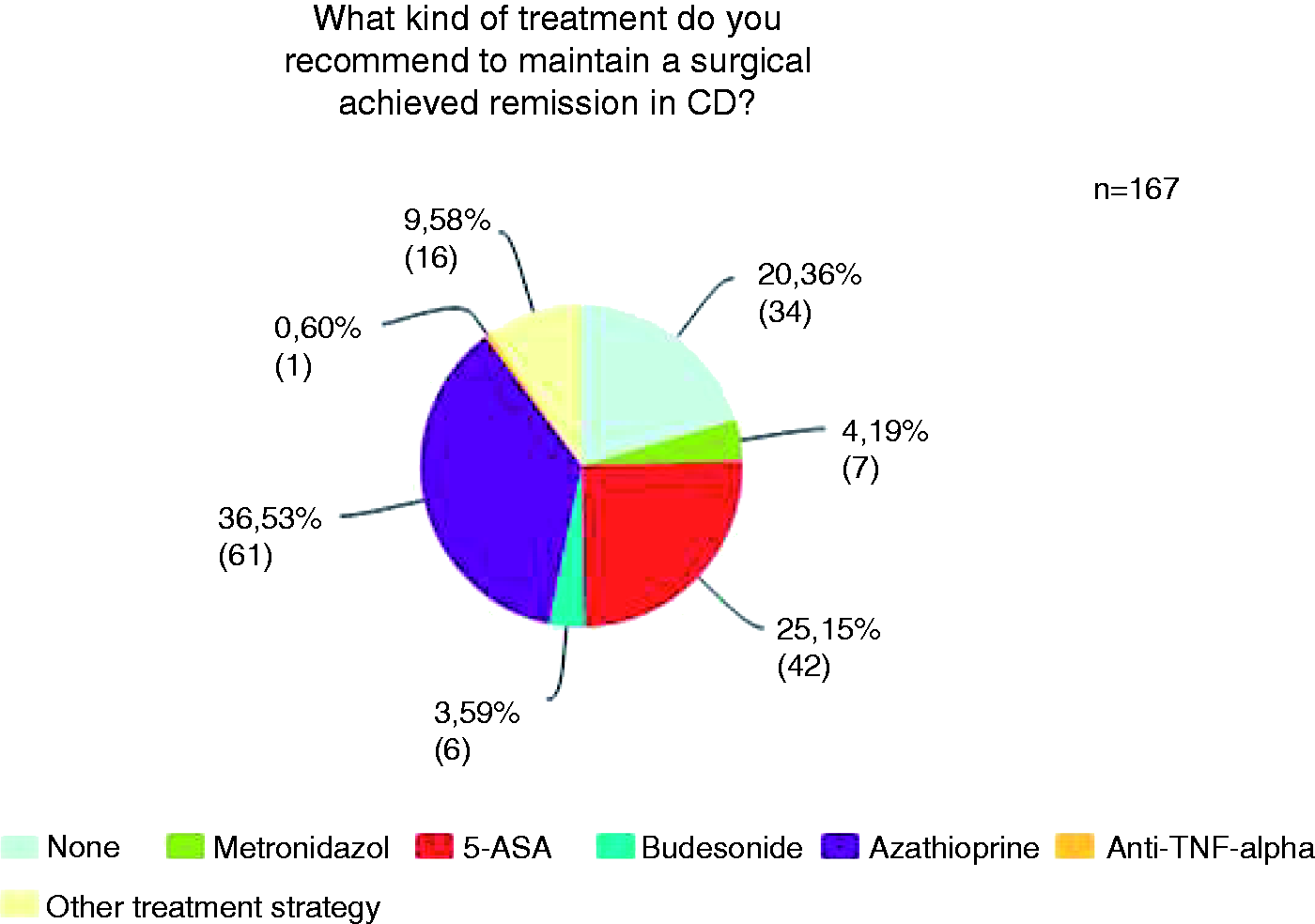
Different clinical scenarios and use of 5-ASA in CD
The further questions of this survey were especially designed to enlighten aspects of 5-ASA in CD. Since the clinical context is one of the main factors influencing therapeutic decisions, we asked which scenario allows the rational use of 5-ASA. At this question it was allowed to pick more than one answer. With 73.1% the highest rated statement was to use 5-ASA in mild CD (20.5% in moderate disease; 6.4% in severe disease) and only 8.2% would never use 5-ASA in CD (Figure 5). About 28.1–38.6% see a potential of 5-ASA in the combination with other therapeutics or as mono-therapy for the induction of remission and/or maintenance therapy (Figure 5).
Different clinical scenarios – therapeutic implications for the use of 5-ASA.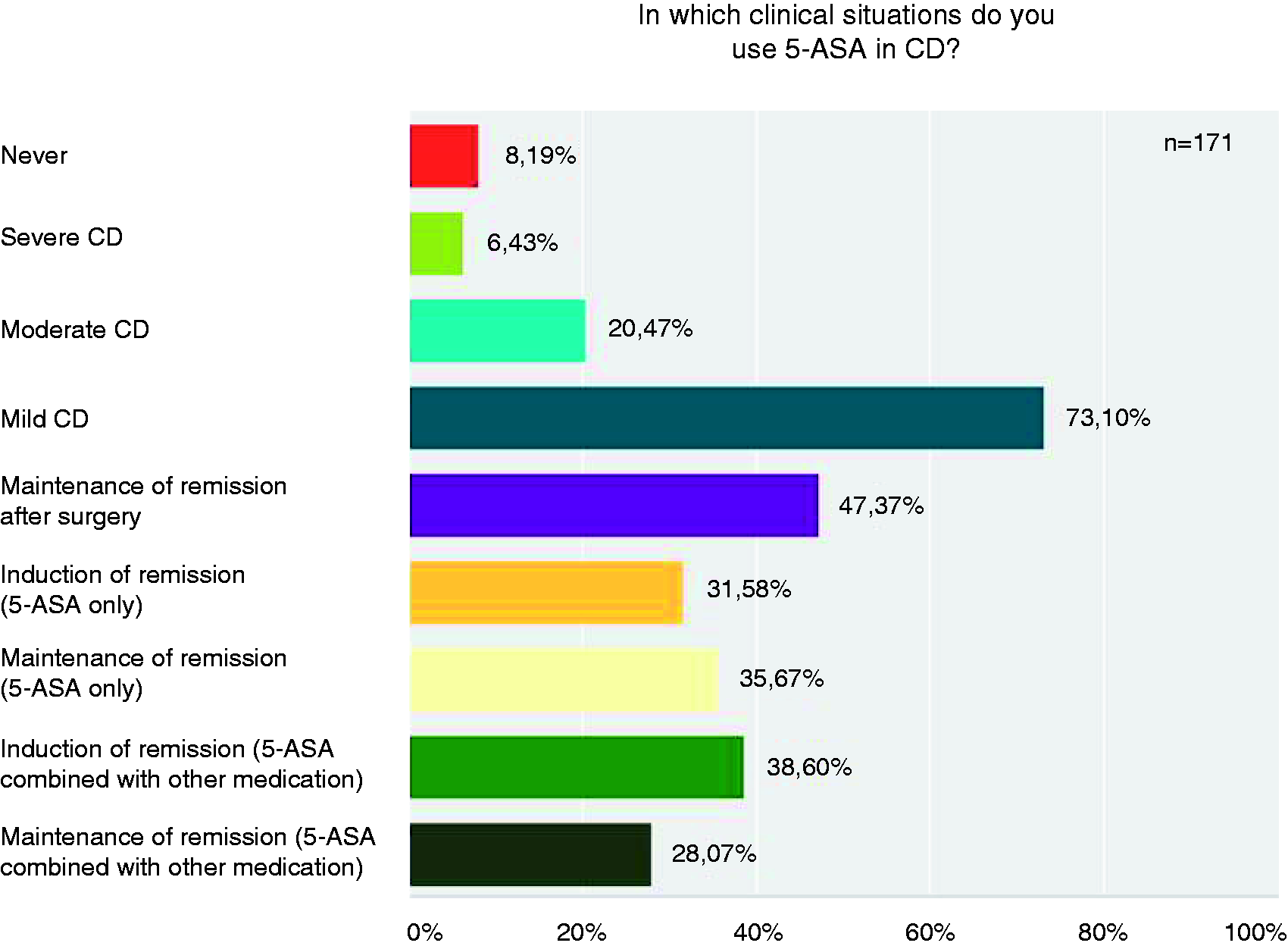
The use of 5-ASA in cases of unclassified colitis was also assessed and 56.5% (95/168) stated that they usually use 5-ASA in this setting and 10.1% (17/168) use it at all times. 32.7% (55/168) use it sometimes (data not shown).
Eighty-three percent (139/168) of the respondents report <5% of 5-ASA-related side effects in their daily clinical practice (Figure 6(a)), the main ones being nausea, unspecific gastrointestinal symptoms, and headache (Figure 6(b)). With the aim of inducing remission in CD, 91.8% (146/159) prescribe 2.6–4.5 g 5-ASA daily, 62.7% (96/153) perform a dose reduction to 1.0–2.5 g daily during maintenance therapy, whereas 36% continue high doses (2.6–4.5 g). Ninety-four percent (158/168) of the respondents favor mesalazine as 5-ASA derivative in their clinical practice, 5.9% (10/168) use sulfasalazine.
5-ASA-related side effects.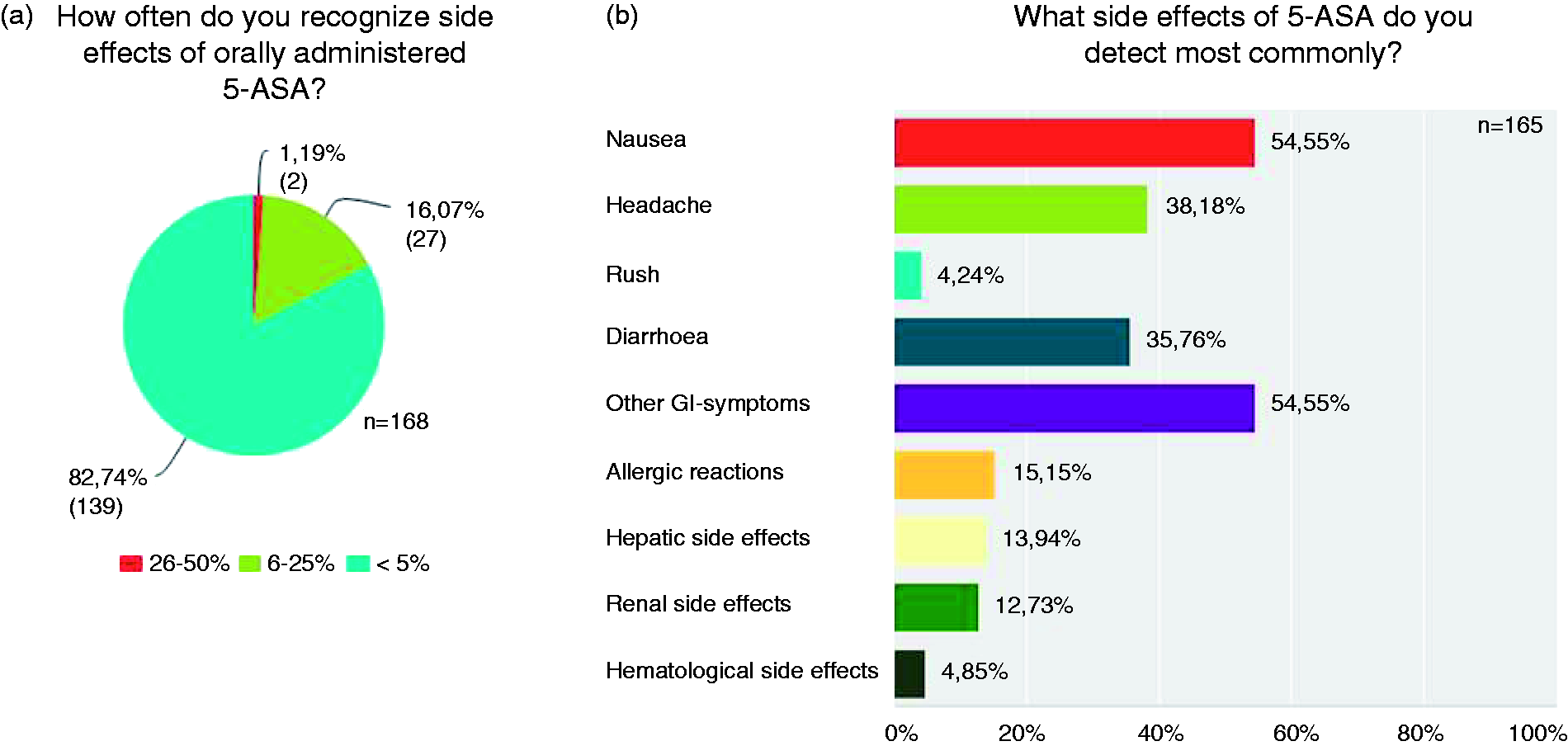
Respondents’ individual comments on the “Pros” and “Cons” of 5-ASA in CD
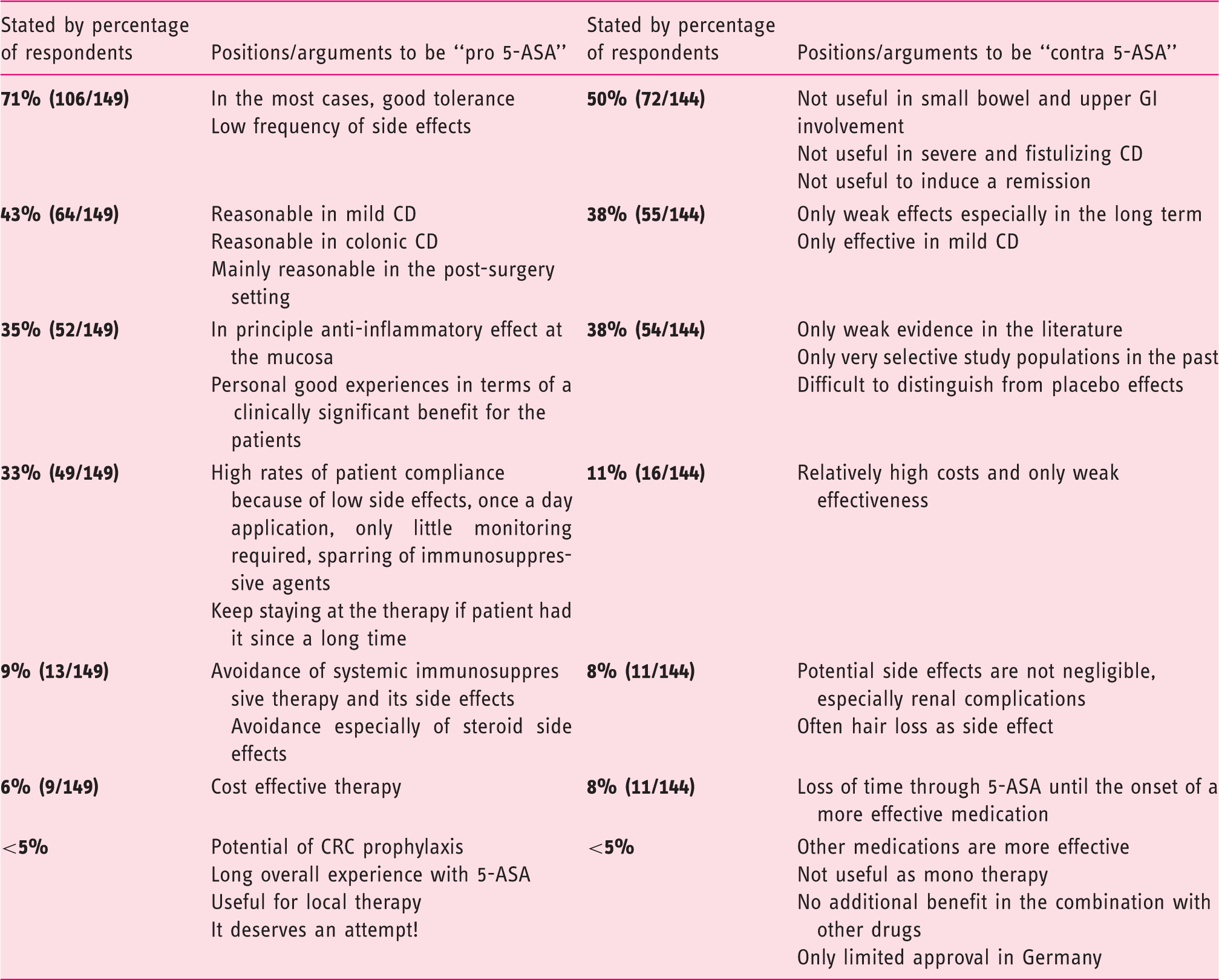
With 50% (72/144), the main “Con” 5-ASA statement was that it is not useful in clinical situations like small bowel or upper GI involvement of CD, fistulizing CD, and in terms of induction of remission in acute CD. The second highest rated “Con” statement (38.2%; 55/144) was that 5-ASA might only be useful in mild CD and that it might have only weak beneficial effects, especially as long term treatment. Thirty-eight percent (54/144) stated that there is only weak empirical evidence concerning the effectiveness of 5-ASA, in only very selected patient collectives. For further statements see Table 1.
Discussion
In this study we found that guideline adherence in Germany concerning the available therapeutic options for induction and maintenance therapy of CD is generally quite good. However, some particular clinical scenarios and therapeutic approaches diverge from the guidelines, use of 5-ASA in particular.
At first the most comprehensive guideline adherence can be noted for induction therapy of (mild to moderate) ileal CD. About 82.9% recommend budesonide as first line therapy as recommended in the German guidelines (Figure 2(a)). 13 For induction of remission in colonic CD, about one third of the respondents prefer a 5-ASA-mono-therapy, one third systemic steroids, and 23.4% the combination of both (Figure 2(b)). The German guidelines recommend systemic steroids or sulfasalazine in colonic CD, but not the combination of both. 13 Thus, guideline adherence regarding the induction of remission in colonic CD is more variable. These inconsistencies might be due to different treatment strategies adjusted to different disease activities, which were not fully detailed in our survey. Therefore it is conceivable that in daily clinical care the choice of systemic steroids versus 5-ASA or the combination is individualized to the respective disease activity. However, it should be noted, that in our study only 5.9% of the respondents use sulfasalazine as 5-ASA derivative. Therefore the chosen 5-ASA-derivative is not in line with guideline recommendations. 13
Regarding the induction therapy for combined small and large bowel disease about one third recommend systemic steroids and 25.6% the combination of 5-ASA and systemic steroids. In this setting, only 8.1% of the respondents use 5-ASA alone (Figure 2(c)). Therefore, again, guideline adherence seems to be good, as systemic steroids are recommended. 13 Nevertheless, about 16.9% use budesonide alone and nearly 14% budesonide combined with 5-ASA in this setting, possibly in patients with predominantly right-sided ileo-colitis. In line with the German guideline and independent of disease location, no-one recommended an anti-TNF-therapy in the first line and <4% prescribe azathioprine for inducing a remission in CD (Figure 2).
Furthermore, we asked for the management of maintenance therapy after an achieved remission (after first flare) in CD. In this setting, the German guidelines discuss “watch & wait” as justifiable. 13 This was recommended by ca. 34–42% of our respondents (largely regardless of disease localization). However, the German guidelines furthermore underline the necessity to stop smoking, an option recommended by only 50% of our respondents (Figure 3). This is in line with other observations in Germany, showing that about 41% of CD patients are smokers. 14 Hence there is a need for guideline implementation strategies regarding cessation of smoking in CD. In the German guidelines the use of azathioprine/6-mercaptopurine during maintenance is suggested for complex disease courses (e.g. fistulas) and not in mild CD, 13 accordingly only about 8–20% recommend this therapy.
One of the major controversies in the field is reflected in the questionnaire’s results on 5-ASA use in CD. Overall, there is weak and controversial evidence of its effectiveness. A 2011 published meta-analysis of 22 randomized controlled trials reassessed the efficacy of 5-ASA in CD. This analysis suggests that 5-ASA might be more effective than placebo in inducing remission in active CD. A subgroup analysis revealed positive effects of 5-ASA in preventing disease relapse. Albeit this benefit is described as modest, it might have a desirable risk-benefit profile for CD patients. 15 In any case, even this cautious conclusion is not shared by all IBD experts and had been criticized because of the meta-analysis design. 16 Regarding the induction of remission the available studies showed conflicting results, were underpowered or un-interpretable. 17 However, recent studies on 5-ASA induction were positive, particularly in patients with mild to moderate disease.18,19 It is quite possible that these reports impact on the IBD-practitioners views, supporting their rather extensive use of this drug in active disease.
Maintenance of a medically or surgically achieved remission with 5-ASA is also grounded on a weak evidence base for the maintenance of surgically induced remission and is not significant after medically induced remission.17,20–22 Therefore, a further guideline deviation can be recognized in our survey, regarding the use of 5-ASA as maintenance therapy in colonic and ileo-colonic CD. About one third of our respondents prescribe 5-ASA in this setting, without recommendation and scientific background (Figure 3(b) and (c)). 13
Answers regarding the frequency and kind of side effects of 5-ASA are widely in line with the available empirical data. 23 About 83% of the respondents see side effects in less than 5% of their patients (Figure 6(a)). The dosage of 5-ASA for maintenance therapy seems to be chosen to high by about 36% of our respondents. They prescribe 2.6–4.5 g/d in this clinical setting. Recommendations of the pharmaceutical companies producing Mezavant and Salofalk Granustix for example state doses of 1.5–2.4 g/d for maintenance therapy of UC, whereas the dosage for CD is even not mentioned.24,25 However, in the ECCO guidelines for CD 11 studies investigating 5-ASA for the maintenance of a medically achieved remission are listed. Only four out of these 11 studies used doses>2.4 g/d, without showing an average benefit of the higher dosage regimen. 23
In our study, diverse therapeutic strategies were chosen to maintain a surgically remission in CD. Most prominently about 36% of the IBD-practitioners initiate a therapy with azathioprine and on second position 5-ASA is recommended (Figure 4). However, 5-ASA seems to be of limited value and no concluding evidence is available for its role in maintaining a surgical achieved remission in CD. 26 Regarding azathioprine/6-mercaptopurine, the available data in the post-surgical management of CD seem to confer a slight benefit compared to placebo or 5-ASA. Therefore this strategy can be considered as feasible, especially in patients with a moderate risk of recurrence, 26 although overall 5-ASA was equivalent in some patient cohorts. 27
A surprising result was that only 4% of the respondents recommend an endoscopic evaluation after 3-6 months, although endoscopy reveals early lesions predictive of symptomatic disease recurrence. 28 It is also unclear why antibiotics like metronidazol or ornidazol are used so infrequently in the post-operative setting, despite good controlled trial evidence for their effectiveness.29–31 Possibly, their side effect profile is perceived as prohibitive.
As a caveat, the results of this survey have to be interpreted with caution, because of some weaknesses. First, the number of respondents (n = 175, out of about 2850 German gastroenterologists) may not be representative for all German gastroenterologists dealing with IBD patients, 12 even though our respondents are considered to be IBD specialists. Generalization regarding the reality of IBD patient care in Germany is therefore not possible. On that account it should be kept in mind, that a large proportion of IBD patients are treated by general practitioners rather than gastroenterologists. 10 Possibly, therefore guideline-conform treatment of IBD patients might be less common than observed in our survey. However, the views of IBD-practitioners should not be underrated compared to guideline recommendations, as their experiences and opinions reflect the daily situation of IBD patients. In addition, this survey only addresses the physicians rather than the patient’s concepts about the management of CD and increasingly patient input may direct the physician’s decision away from guideline recommendations.
Footnotes
Acknowledgements
We are grateful to all physicians who participated in this survey. The authors’ share of the workload was as follows: study concept and design (all); acquisition of data (TK); analysis and interpretation of data (all); drafting of the manuscript (all); critical revision of the manuscript for important intellectual content (all); statistical analysis (TK); obtained funding (JW); technical or material support (JW); study supervision (EFS and JW).
Funding
This work was supported by the Robert Bosch Foundation (TK), Stuttgart, Germany, and by the European Research Council.
JW is a European Starting grantee. Funded by the German Research Foundation (DFG).
Conflict of interest
EF Stange has received honoraria from Falk Pharma, AbbVie, Ferring, and Ardeypharm, and consultancy from Merck and Takeda. J Wehkamp has received honoraria from Falk Pharma, AbbVie, Ferring, Ardeypharm, MSD, Novartis, Takeda, Roche, and Boehringer-Ingelheim. T Klag has received honoraria from MSD.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.