
Abstract
Background
There is considerable variation in the quality of colonoscopy performance. The Norwegian quality assurance programme Gastronet registers outpatient colonoscopies performed in Norwegian endoscopy centres. The aim of Gastronet is long-term improvement of endoscopist and centre performance by annual feedback of performance data.
Objective
The objective of this article is to perform an analysis of trends of quality indicators for colonoscopy in Gastronet.
Methods
This prospective cohort study included 73,522 outpatient colonoscopies from 73 endoscopists at 25 endoscopy centres from 2003 to 2012. We used multivariate logistic regression with adjustment for relevant variables to determine annual trends of three performance indicators: caecum intubation rate, pain during the procedure, and detection rate of polyps ≥5 mm.
Results
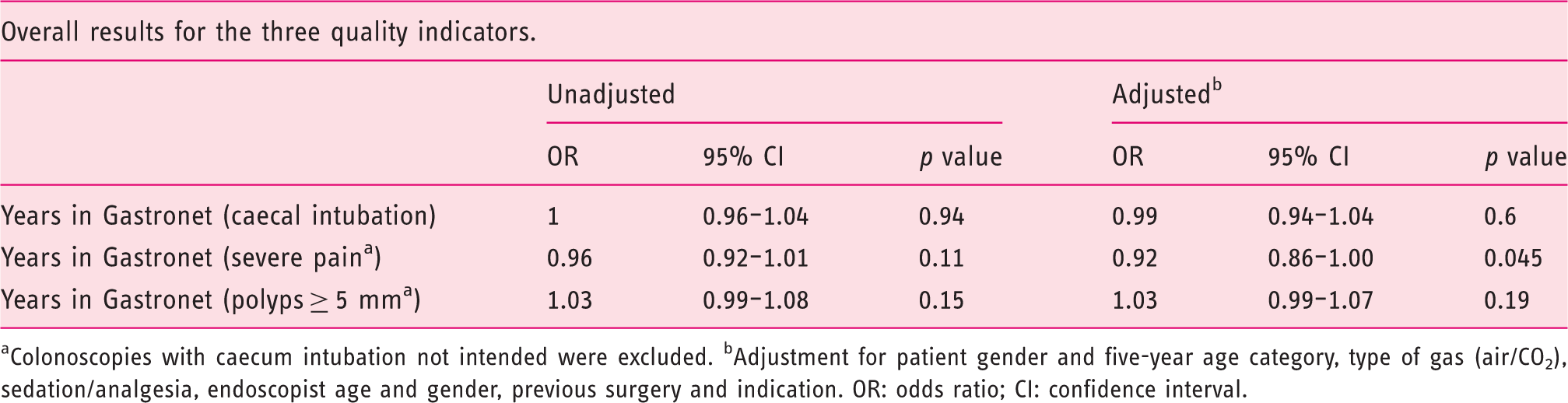
The proportion of severely painful colonoscopies decreased from 14.8% to 9.2% (relative risk reduction of 38%; OR = 0.92 per year in Gastronet; 95% CI 0.86–1.00; p = 0.045). Caecal intubation (OR = 0.99; 95% CI 0.94–1.04; p = 0.6) and polyp detection (OR = 1.03; 95% CI 0.99–1.07; p = 0.15) remained unchanged during the study period.
Conclusions
Pain at colonoscopy showed a significant decrease during years of Gastronet participation while caecal intubation and polyp detection remained unchanged – independent of the use of sedation and/or analgesics and level of endoscopist experience. This may be due to the Gastronet audit, but effects of improved endoscopy technology cannot be excluded.
Keywords
Introduction
There is a continuous need for improving the quality of medical care. Medical quality registers are often used to enable feedback to health care providers. However, there are conflicting results regarding the effectiveness of such feedback.1–5 Quality assurance (QA) of flexible gastrointestinal endoscopy services has been recommended.1,6 In Norway, a national QA programme for colonoscopy was implemented in 2003 – the Gastronet programme.1,7 This programme provides annual feedback of performance indicators to individual endoscopists and endoscopy centres. Improvement of standards remains the responsibility of each centre and the individual endoscopist, but is encouraged through network meetings within the Gastronet programme. The present study analysed whether there are changing trends of three key quality indicators for colonoscopy in Gastronet during a period of nearly 10 years from 2003 until 2012.
Materials and methods
The Gastronet colonoscopy register includes outpatient procedures except for only one tertiary reference hospital with predominantly inpatient colonoscopies (www.kreftregisteret.no/gastronet). Included patients have to be 18 years of age or older. Coverage is estimated by matching against the Norwegian Patient Register.
Only endoscopists who registered at least 300 colonoscopies over a two-year period or longer were included in this study. The inclusion period was from September 2003 to 31 December 2012 (for polyp detection since 2006 only).
The Gastronet programme uses two questionnaires for each performed colonoscopy. One form contains procedural variables to be filled in by the endoscopist and the other contains questions on discomfort and satisfaction to be filled in by the patient at home on the day after the examination. Both forms are sent to the Gastronet secretariat. The endoscopist form includes information about indication, previous abdominal surgery, sedation, type of insufflation gas (carbon dioxide or air), caecal intubation, duration of examination and time to caecum, clinical diagnosis and detected number of polyps with estimated diameter of 5 mm or larger (a surrogate for adenoma detection rate (ADR)).8,9 The patient form includes a four-category-Likert scale for pain (no pain, slight pain, moderate pain and severe pain). 10 The patients mail the completed form directly to the Gastronet secretariat.
Results on performance indicators are provided yearly to all participating endoscopists who have registered at least 30 colonoscopies during the last year and to each participating centre. Each endoscopist knows only his or her identity code in the reports. Results from other endoscopists and centres are anonymised. Measures that may be taken locally to improve quality (retraining programme, individual interviews, etc.) are not routinely reported to Gastronet.
Variation among endoscopists and changes over time were explored for the three quality indicators caecal intubation rate (CIR), detection of polyps ≥5 mm in diameter and proportion of severely painful colonoscopies.
All three quality indicators were analysed in two steps. In step one, a logistic regression was performed comprising all included colonoscopies (procedure level). In step two, we calculated individual quality indicators for each endoscopist for each year in Gastronet (endoscopist level). These individual results were then analysed by applying scatterplots and trend tests. Individual quality indicators were not calculated if the endoscopist had registered fewer than 30 procedures during that particular year. Due to the steadily increasing number of participating centres and endoscopists in Gastronet during the course of this study, the highest number of included colonoscopies and endoscopists was registered in their first year of Gastronet participation (defined as Gastronet year one). Consequently the number of included colonoscopies and endoscopists available for analysis declined steadily toward the last Gastronet year since the more recent entries have not had time to accumulate years of membership (few ‘Gastronet years’). A sensitivity analysis was applied by excluding colonoscopies at centres ending Gastronet participation prematurely in order to see if this might change the results.
According to United States (US) guidelines, 11 a CIR of at least 90% in routine clinical work and 95% in screening colonoscopies is recommended. European guidelines propose a minimum standard of 90% for unadjusted CIR for screening colonoscopies. 12 We chose the 90% cut-off because only 0.6% of colonoscopies were screening examinations (www.kreftregisteret.no/gastronet). American guidelines also recommend an ADR of 20% (25% for men and 15% for women). As 80% of colorectal polyps 5 mm in diameter or larger have been shown to be adenomas,8,9 our target was a polyp detection rate (PDR) for polyps ≥5 mm of 25% or more (20%/0.8). An acceptable threshold for pain perception has not been defined in the aforementioned guidelines. In the present study, the proportion of patients reporting ‘severe pain’ was evaluated. On average, 12% of patients reported severe pain during colonoscopy in 2012. This threshold was arbitrarily chosen as a cut-off for minimum standard performance in the analysis.
For the analysis of detection of polyps ≥5 mm, all endoscopists who started in Gastronet before 2006 were excluded as polyp size was not included in the endoscopist form before 2006.
In a sensitivity analysis we focused on the lowest quartile of individual endoscopist performance for each indicator. In another sensitivity analysis we looked at the results separately for procedures with no sedation or analgesia and procedures with sedation/analgesia, respectively.
Statistical analysis
Logistic regression models were used to estimate the effect of time (years) after each endoscopist initiated reporting to Gastronet on the three dichotomous indices of performance (CIR above or below 90%, PDR above or below 25%, and patient’s report on severe pain). The reported odds ratios (OR) measure the relative change in odds of the specific outcome per year participation in Gastronet. Cluster-robust standard errors were applied to adjust for the inherent clustering by endoscopist. 13 All multiple regression models included adjustments for patients’ sex and five-year age category, previous surgery, sedation/analgesia, gas insufflation, indication, endoscopist gender and age of endoscopist when joining Gastronet. The Cochran-Armitage test for trend was used to assess change in quality indicators per year of participation in Gastronet at the endoscopist level. The statistical analyses were performed with SPSS v.19 and Stata 12 (StataCorp LP, College Station, TX, USA).
Ethics
The Regional Committee for Medical and Healthcare Research Ethics of the South Eastern Norwegian Health Board waived their need to evaluate the study protocol.
According to requests from the Norwegian Data Inspectorate, patient age was registered in five-year age categories instead of exact number of years.
Results
In total, 73,522 colonoscopies performed at 25 centres by 73 endoscopists (61 male and 12 female) were included in the study (Figure 1).
Flowchart showing the inclusion and exclusion criteria for colonoscopies and endoscopists in the total study period 2003–2012 for analysis of the three quality indicators (caecal intubation, severe pain and detection of polyps >5 mm (polyp detection rate (PDR)-5 mm). PDR-5 mm was registered in 2006–2012 only.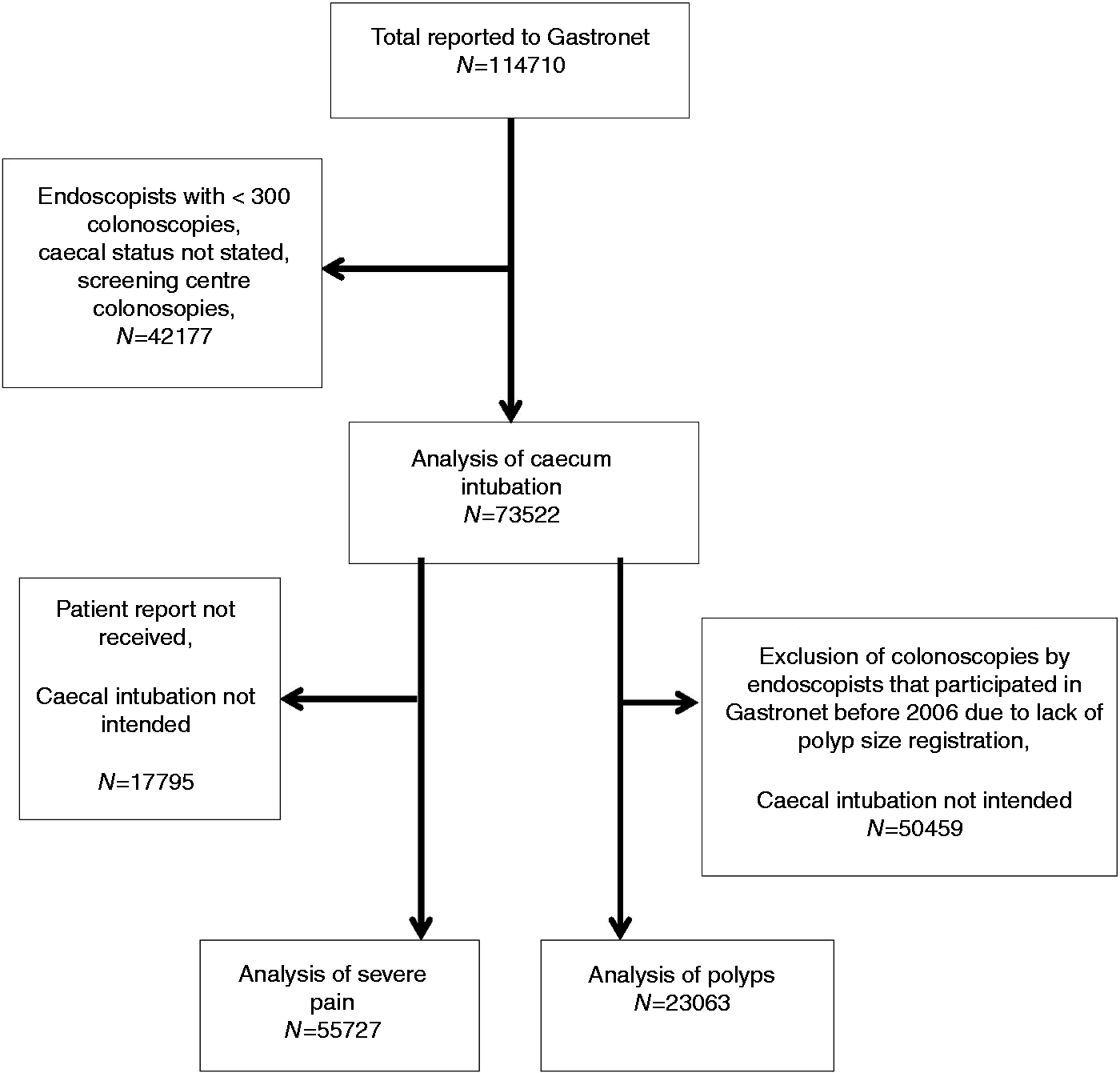
This represents a coverage of 33% of all outpatient colonoscopies performed in Norway during the study period according to the Norwegian Patient Register. In our study, 45% of the patients were male and 55% were female. The median five-year age category of the patients was 55–59 years. The mean age of the endoscopist at Gastronet registration was 47 years. Endoscopy centre participation is shown in Figure 2.
The course of participation for the 25 endoscopy centres in the study period 2003–2012.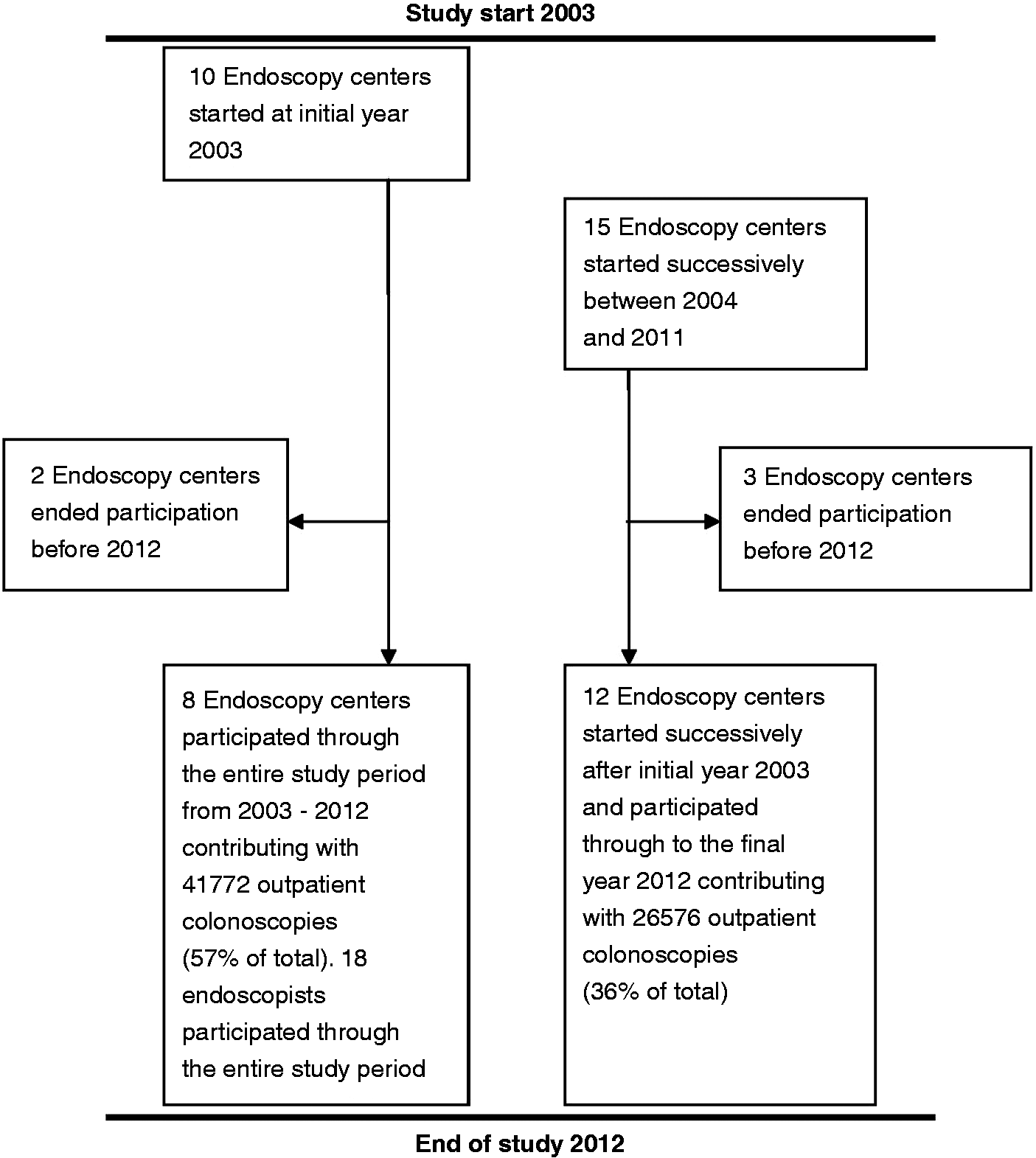
Five centres contributing 5161 colonoscopies ended participation before the final study year 2012, one of them due to closure and four of them due to other reasons which were not explored any further. In a sensitivity analyses, these centres were excluded, but the results did not change materially (data not shown).
CIR
The unadjusted CIR for the entire number of included colonoscopies was 91.8% in the first year of participation, and remained stable during the study period (adjusted OR 0.99, 95% confidence interval (CI) 0.94–1.04, p = 0.60) (Table 1 and Figure 3).
Development of quality indicators (polyp detection rate (PDR) ≥ 5 mm, severe pain, completed colonoscopy) in Gastronet as mean percentage of all participating endoscopists’ colonoscopies per year. Overall results for the annual change of the three quality indicators (caecal intubation, severe pain and polyp detection ≥ 5 mm) with odd ratios, confidence intervals and p value per Gastronet year Colonoscopies with caecum intubation not intended were excluded. bAdjustment for patient gender and five-year age category, type of gas (air/CO2), sedation/analgesia, endoscopist age and gender, previous surgery and indication. OR: odds ratio; CI: confidence interval. 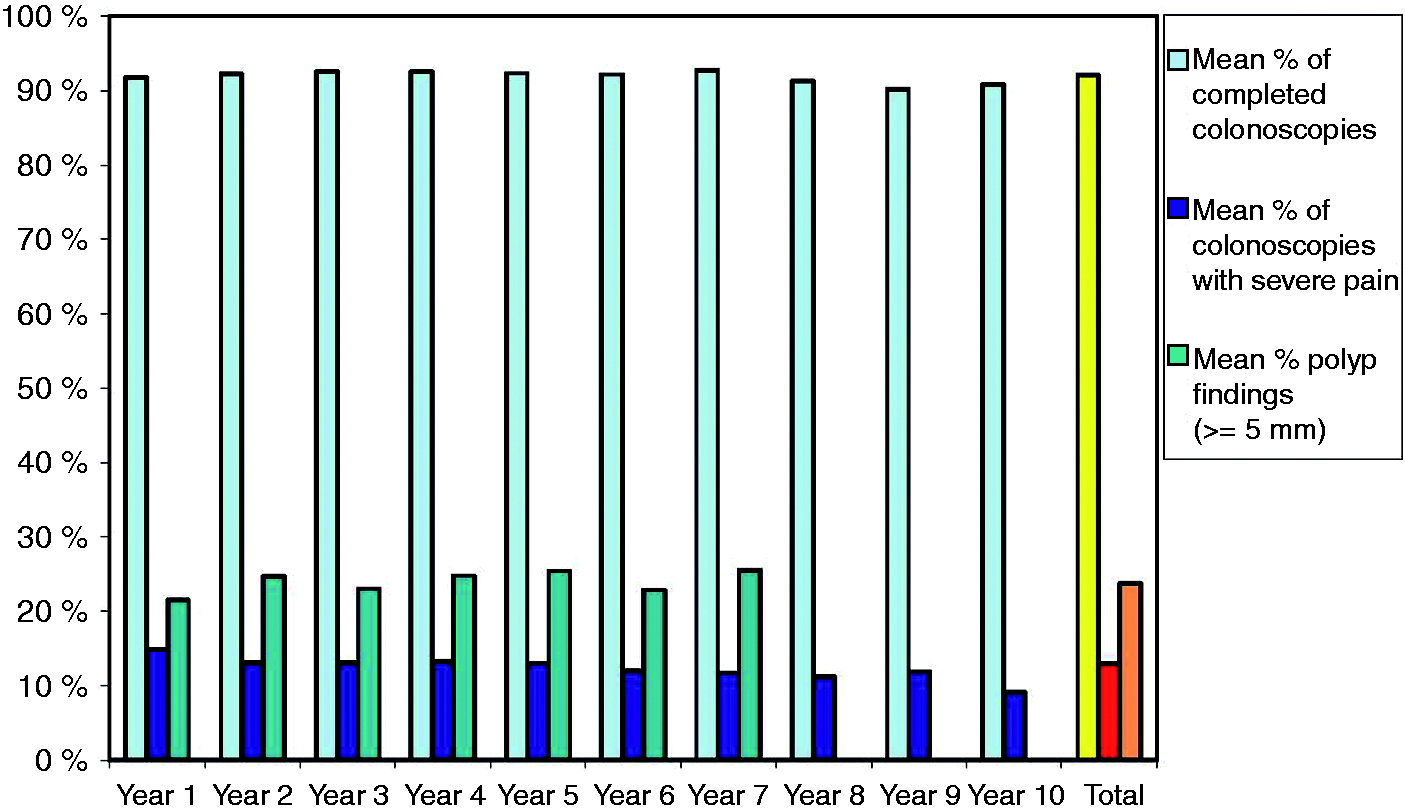
In the first year of registration, 49 out of 71 endoscopists (69%) had an individual CIR of 90% or higher compared to 10 endoscopists out of 13 (77%) in the tenth year of participation (p value for trend = 0.43) (Figure 4(a)).
Three scatterplot diagrams (Figure 4(a)–(c)) depicting the variation of the participating endoscopists’ performance with regard to the three quality indicators (caecal intubation rate (CIR) (a), percentage of colonoscopies with severe pain (b) and polyp detection rate (PDR) (c)) per Gastronet year of participation. One circle represents one endoscopist’s performance result for this particular Gastronet year. The red line indicates the desired level of performance (CIR ≥ 90%, none for severe pain and PDR-5 mm ≥ 25%).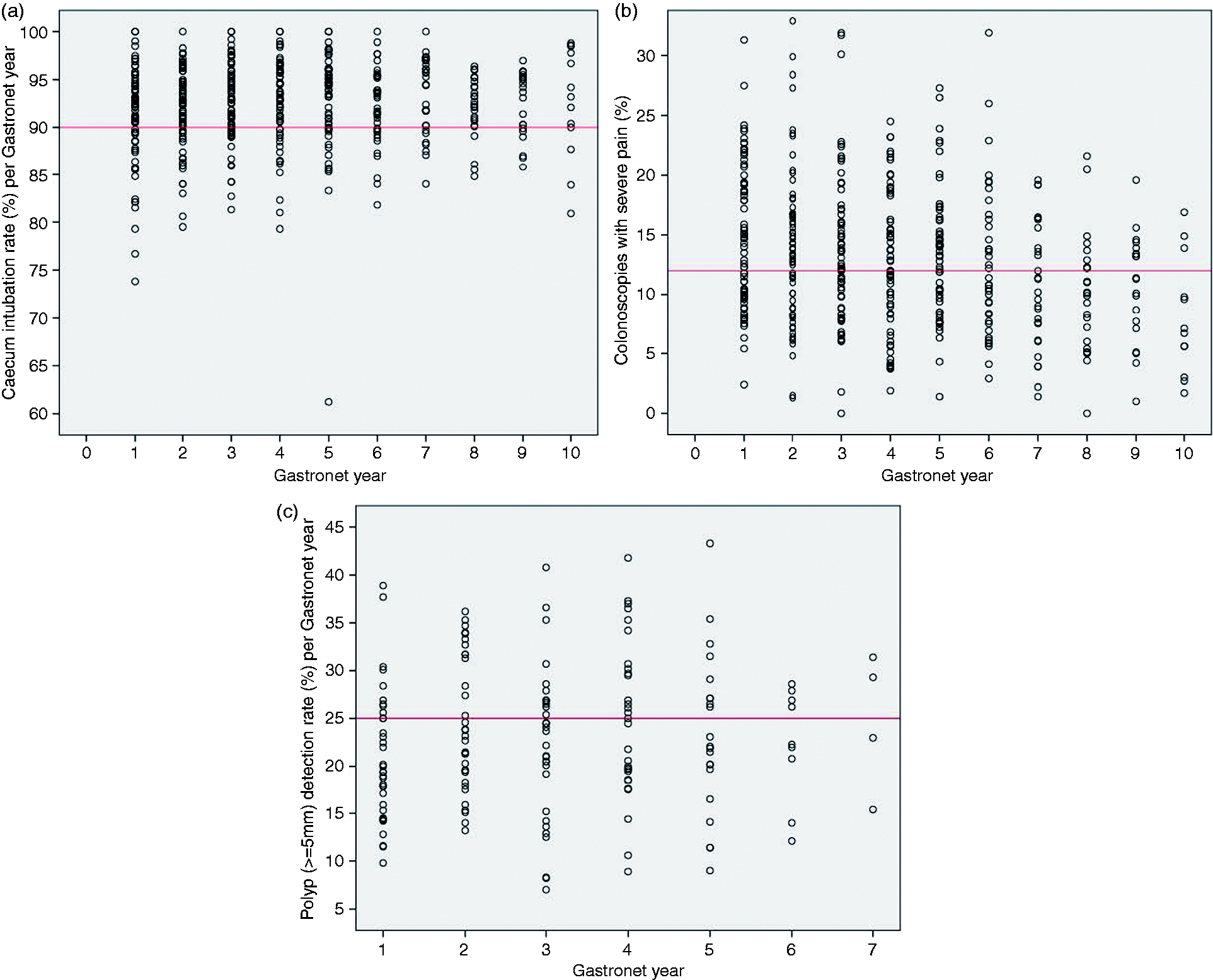
The number of endoscopists who accomplished the desired quality level and the number of those who did not (percentages of endoscopists at this particular year): (a) CIR; (b) percentage of colonoscopies with severe pain; (c) PDR-5 mm
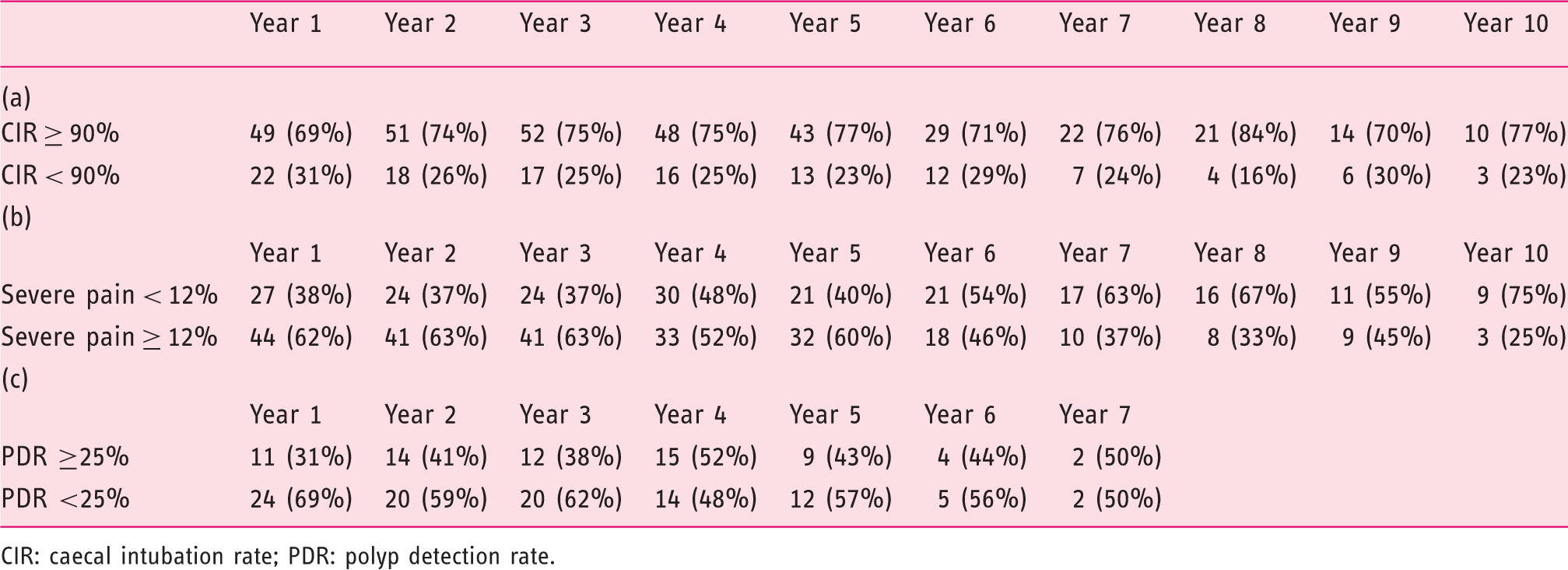
CIR: caecal intubation rate; PDR: polyp detection rate.
Severe pain
A total of 14.8% of the patients examined during the first year reported severe pain. In the tenth year it was reduced to 9.2% (Figure 3).
Crude and adjusted odds ratios (OR) with 95% confidence interval (CI) for patients reporting severe pain during colonoscopy
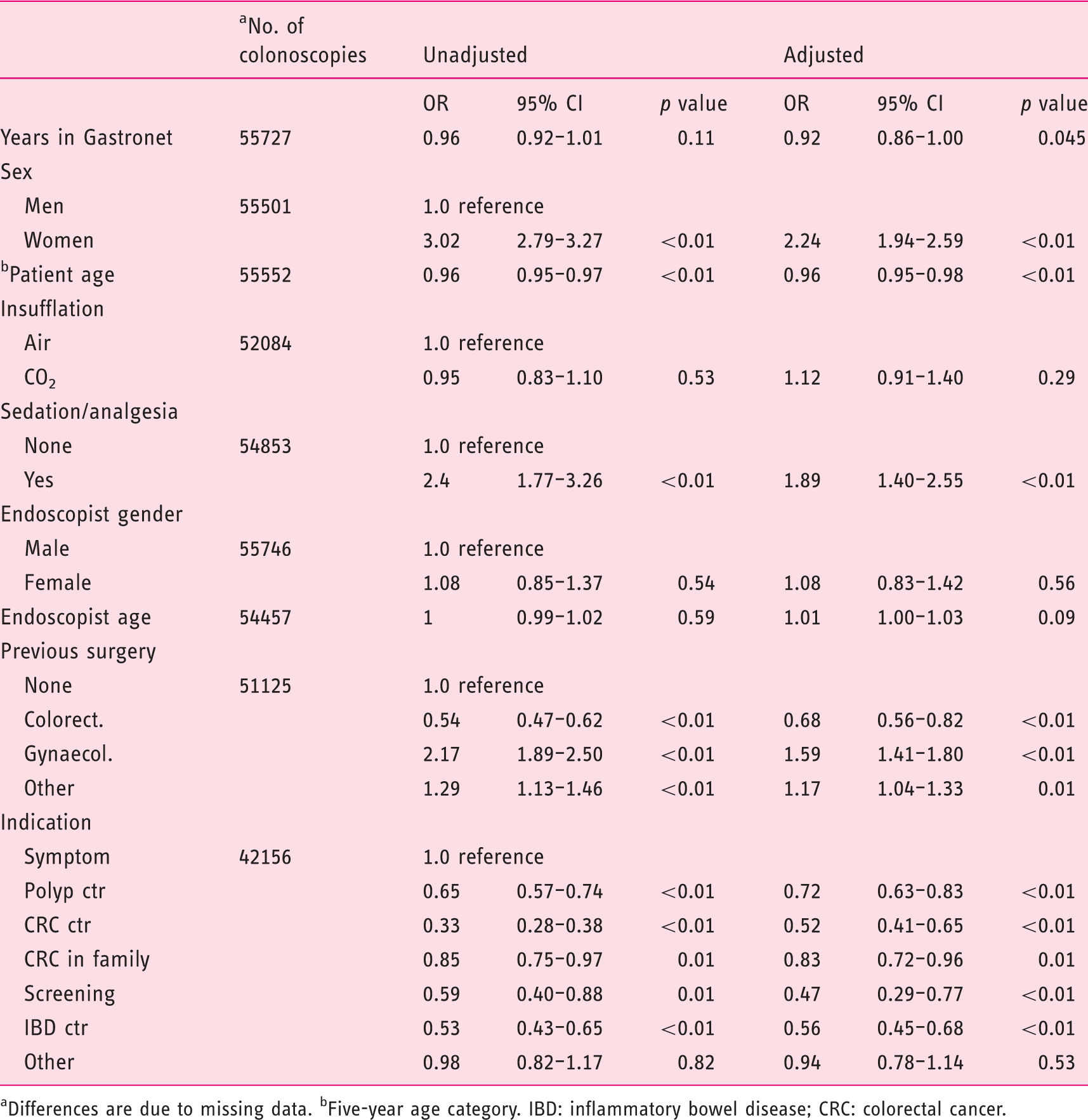
Differences are due to missing data. bFive-year age category. IBD: inflammatory bowel disease; CRC: colorectal cancer.
Twenty-seven out of 71 endoscopists (38%) reached an individual level of less than 12% of procedures with severe pain in the first year, and nine out of 12 endoscopists (75%) reached this level in the tenth year (p value for trend < 0.001) (Figure 4(b)).
Neither the gender nor the age of the endoscopist had any influence on severe pain during the procedure (Table 3). Improvement as shown by Figure 4(b) was evident both for experienced and inexperienced endoscopists (data not shown).
The rate of sedation and/or analgesic medication used before or during the procedure was 32% in the first year and 28% in the tenth year.
PDR
The PDR-5 mm for the entire number of colonoscopies included in the polyp analysis was 21.6% in the first year. The adjusted OR for finding a polyp ≥5 mm was 1.03 (0.99–1.07) per year of participation in Gastronet (p = 0.19) (Table 1 and Figure 3). In the first Gastronet year, 11 out of 35 endoscopists (31%) had an individual PDR-5 mm of 25% or higher. In the sixth year four out of nine endoscopists (44%) and in the seventh year two out of four contributing endoscopists accomplished this goal (p value for trend = 0.21) (Figure 4(c) and Table 2).
Due to low procedure numbers in the last two years of polyp analysis (1031 and 231 colonoscopies) in contrast to more than 3000 procedures in the first five years, we performed another sensitivity analysis excluding the two final years. This analysis did not materially change the results for polyp analysis (OR 1.04, p = 0.16).
Sensitivity analyses
A sensitivity analysis was performed in the group of colonoscopies performed by endoscopists in the lowest quartile of performance for each indicator in their first Gastronet year (18 endoscopists for CIR (CIR <89.4%) and severe pain (severe pain in more than 19.3%) and eight endoscopists for PDR-5 mm (PDR-5 mm <14.6%). Colonoscopies performed by these ‘poor starters’ showed no improvement with regard to severe pain (adjusted OR 0.96, 95% CI 0.91–1.02, p = 0.17; 15,110 colonoscopies included) but they improved with regard to polyp detection (adjusted OR 1.23, 95% CI 1.10–1.38, p < 0.001; 3858 colonoscopies included). Similar to the entire study population, the CIR remained unchanged over time (adjusted OR 1.03, 95% CI 0.97–1.08, p = 0.36).
Another sensitivity analysis on unsedated colonoscopies (n = 38,106) showed no significant reduction in severely painful colonoscopies over time (adjusted OR 0.97; 95% CI 0.89–1.05; p = 0.46). A sensitivity analysis on colonoscopies with sedation/analgesia (n = 10,400) showed that most of the reduction in severe pain over time occurred in exactly this subgroup (adjusted OR 0.86; 95% CI 0.82–0.90; p < 0.001).
Discussion
This is the first long-term report on trends of performance in a QA register for colonoscopy.
The QA variables CIR, PDR and proportion of severely painful procedures were analysed. There was a significant reduction in severe pain. However, it is not satisfactory that this change in performance quality took 10 years to happen.
In contrast, there were no changes in either PDR or in procedure completion.
Gastronet provides performance data to centres and endoscopists, encouraging them and their local leaders to use this information in their local QA work. In a systematic review on how medical registers provide information feedback, van der Veer at al. 1 found limited and varying effects of QA registers and identified a series of barriers to be addressed to improve success, like lack of trust in the data (e.g. the ‘we have sicker patients’ syndrome), lack of motivation and organisational constraints. In Gastronet, the barriers are unknown, but it may be due to high work load, lack of local organisational support or even unawareness of differences between endoscopists at the local centre.
Pain
A total of 14.8% of patients reporting severe pain at colonoscopy in the first year of Gastronet participation is unacceptably high. Different approaches are proposed in the literature to evaluate the degree of discomfort or pain for the patient – either by the patient himself or herself, the endoscopist or the assisting nurse. 14 Although pain is a highly subjective factor with huge inter-individual variation and difficult to measure, Gastronet has chosen the patient’s own opinion as benchmark for pain perception.
During 10 years of Gastronet a continuous decrease of severe pain has been shown. The decrease to 9.2% reporting severely painful colonoscopies in the most recent Gastronet year is equivalent to a 38% reduction, which we regard as clinically relevant. Surprisingly, this improvement was not associated with frequency of using sedatives and/or analgesics (32% in the first year and 28% in the last year of Gastronet participation). The fact that the reduction of painful procedures is seen in the subgroup of colonoscopies with sedation and/or analgesics (adjusted OR 0.86; p < 0.001 in the sensitivity analysis) implies that the endoscopists rather than increasing the frequency of the use of medication, became smarter in applying medication and selecting the right patients who will profit from it in the course of the study. It is, however, an unsolved problem that the reduction of severely painful procedures is not seen for colonoscopies performed by those endoscopists who constitute the lowest quartile of performance with regard to severe pain (adjusted OR 0.96, p = 0.17 in the sensitivity analysis). This suggests that ‘poor starter’ endoscopists are not sufficiently cared for in terms of local training and surveillance.
The trend toward improvement on pain during colonoscopy in the course of the study was not restricted to less-experienced endoscopists. Also, endoscopists who were experienced at study entry (more than 1000 pre-study colonoscopies) showed a clear tendency toward less pain reported during their years in Gastronet.
As our study did not include a control group of endoscopists not receiving performance feedback, we can state only that a significant decrease in pain has been documented in Gastronet. The causality between improvement and Gastronet participation remains unclear. The improvement might be a consequence of the Gastronet feedback, but it might just as well be a result of improved experience, technique and endoscopy technology over time. The use of sedation and analgesics varies among and within countries and cultures ranging from infrequent use of any sedation to routinely offering deep sedation to all with propofol or general anaesthesia administered by anaesthetists. 15 Conscious sedation on demand with the majority of colonoscopies being performed without any sedation or analgesics dominates in Nordic countries.16,17 This imposes high demands for technical skills on the endoscopist. Although a 38% relative reduction of severely painful colonoscopies is a clinically significant achievement, it is hardly acceptable that it took 10 years, nor is it desirable that 9.2% of the patients in the most recent year of registration still experience severe pain. Thus, a change in policy to lower the threshold for giving analgesics and/or sedation should be implemented in Norway. 18 New techniques like small-calibre endoscopes and the use of water instead of gas/air insufflation may also be important in reducing discomfort during colonoscopy.19–21
CIR
The expectancy of improvement for any defined endpoint depends on baseline values. European and American guidelines recommend a CIR of 90% in routine clinical work.6,22 With a baseline CIR of about 92%, we could hardly expect much improvement except for a few individual suboptimal performers. The percentage of endoscopists with CIR≥90% increased from 69% in the first year to 77% in the tenth year.
In England the Global Rating Scale (GRS) programme was initiated in 2003 to improve on a CIR of 77%. 23 By Joint Advisory Group (JAG) visits to centres and accreditation of centres and endoscopists, the CIR improved to 92% in 2012. 24 Others have also succeeded using local resources discussing performance results and intervention, like Imperiali et al. 25 in Northern Italy, where CIR was improved from 85% to 90%. Ball et al. 26 in England achieved an impressive improvement on CIR from 60% to 94% by a combination of organisational measures which included more time per colonoscopy, letting the most successful endoscopists perform more colonoscopies, retraining the less successful and even advising some to give up colonoscopy entirely.
PDR
Guidelines recommend an ADR of 20% based largely on studies on screening populations 22 which translates to a PDR-5 mm of 25%.8,9 In the United Kingdom (UK), a PDR of 10% is recommended for routine clinical work. 27 Although recommended and used for QA of routine clinical colonoscopy, the value of ADR and PDR is regarded as limited in a non-screening setting. 28 In our study, baseline PDR-5 mm was 21.6%. An unadjusted logistic regression analysis revealed that there was no improvement in PDR. The adjusted OR for PDR-5 mm was 1.03 (95% CI 0.99–1.07; p = 0.15) – i.e. a statistically non-significant 3% annual increase in PDR-5 mm. A PDR of 25% or higher was regarded as the desired performance level for an individual endoscopist in Gastronet. Eleven out of 35 endoscopists (31%) reached this level in the first year, four out of nine endoscopists (44%) in the sixth year and two out of four endoscopists (50%) in the final seventh year (Figure 4(c) and Table 2).
As we performed sensitivity analyses excluding colonoscopies by endoscopists/centres that ended participation prematurely, we regard the risk of selection bias by good performers participating longer as being small.
Although the number of endoscopists with a PDR-5 mm ≥25% increased from 31% to 50% during the study, this positive development was confirmed neither in the logistic regression analysis at the procedure level nor in the Cochran-Armitage trend test at the endoscopist level (p = 0.21).
The apparent improvement of PDR-5 mm at the endoscopist level might be a result of relatively low numbers of endoscopists in the last two years of polyp analysis, with nine endoscopists in the second last year and only four endoscopists having achieved 7 years in Gastronet by the final year of follow-up (polyp size registration started first in 2006 and therefore we excluded endoscopist who registered before 2006. See Figure 1. Therefore the longest period for follow-up in polyps is 7 years). By calendar year, however, there has been a steady increase in endoscopist and centre participation (Figure 2).
Similarly, the study by Imperiali et al. 25 referred to previously did not achieve an improvement on their 33% PDR (all sizes) in spite of their comprehensive intervention measures. This may be due to high initial PDR – hitting the ceiling for further improvement. Through the very active GRS/JAG intervention programme in the UK, a PDR improvement from 23% to 32% was achieved. 24 This suggests that a PDR beyond 30%–35% may be very difficult to achieve in routine clinics.
Kahi et al. 29 analysed the impact of performance feedback by a quarterly report card provided to endoscopists listing individual results on CIR and ADR. A significant increase of ADR and CIR was shown. ADR increased from 44.7% to 53.9% after intervention (p = 0.013) and CIR from 95.5% to 98.1% (p = 0.027). Although the performance feedback given in this study was very similar to our study, we could not confirm a significant increment of either PDR or CIR. An important difference between our and Kahi’s study is case-mix differences of non-screening and screening procedures. An explanation for Kahi’s remarkably high ADR might be the combination of screening focusing on polyps, few endoscopists (only six) and few procedures (fewer than 1000) in contrast to our present study and those of Imperiali 25 and Gavin 24 comprising routine colonoscopies focusing on explanations for symptoms and with much higher numbers of procedures and endoscopists. It is, however, encouraging to see that in our sensitivity analysis, ‘poor starter’ endoscopists obtained a significant improvement in PDR-5 mm, increasing from 13.5% in their first year to 30.8% in the seventh year (adjusted OR 1.23, 95% CI 1.10–1.38, p < 0.001) which is comparable to Kahi’s results.
A strength of the present study is that it is multi-centred over a decade including a large number of colonoscopies and endocopists. A weakness of the study is that reporting is not compulsory. We have previously shown that incomplete examinations on sedated patients (i.e. the most difficult examinations) tend to be underreported by the patient and patient-reported outcome replies decreased from 87% of colonoscopies reported to Gastronet in 2004 to 80% in 2006. 30 This suggests that the proportion of painful procedures and incomplete examinations may have been underreported in the present study.
In conclusion, during the course of this study on colonoscopies registered in Gastronet, a 38%, statistically significant relative reduction of severely painful colonoscopies was observed, but CIR and PDR remained unchanged. Improvement on pain was independent of the frequency of administration of sedation and/or analgesics. The effect may be due to participation in the Gastronet QA programme both for initially experienced and inexperienced endoscopists, but independent improvements in experience, technique and endoscopy technology cannot be excluded as explanation for the effects observed.
Footnotes
Funding
The Gastronet QA program is funded by the South-East of Norway Regional Health Board (grant number 08/00085).
Conflict of interest
None declared.
Acknowledgements
We are most grateful for contributions on data collection and valuable comments to the manuscript from the following gastroenterologists (endoscopy centre): Asbjørn Stallemo (Department of Medicine, Sørlandet Hospital, Kristiansand, Norway), Ole Høie (Department of Medicine, Sørlandet Hospital, Arendal, Norway), Borgar Flaaten (Department of Medicine, Telemark Hospital, Notodden, Norway), Sverre Nyhus (Department of Medicine, Vestfold Hospital Trust, Larvik, Norway), Fred Arne Halvorsen (Department of Medicine, Vestre Viken Hospital Trust, Drammen, Norway), Lars Aabakken (Department of Medicine, Oslo University Hospital, Oslo, Norway), Jens Pallenschat (Department of Medicine, Sørlandet Hospital, Flekkefjord, Norway), Arnt Sagosen (Department of Medicine, Vestre Viken Hospital Trust, Kongsberg, Norway), Joachim Friestad, (Department of Medicine, Vestre Viken Hospital Trust, Ringerike Hospital, Hønefoss, Norway), Geir Folvik (Department of Medicine, Division of Gastroenterology, Haukeland University Hospital, Bergen, Norway), Eva H Gunther (Department of Medicine, Østfold Hospital, Moss, Norway), Øystein Kjellevold (Department of Medicine, Telemark Hospital, Kragerø, Norway), Ove Lange (Department of Medicine, Nordmøre og Romsdal Hospital, Molde, Norway), Tom Hamre (Department of Medicine, Volda Hospital, Volda, Norway), Njaal Stray (Department of Medicine, Diakonhjemmet Hospital, Oslo, Norway) and Ingrid Berset (Department of Medicine, Ålesund Hospital, Ålesund, Norway) and Ralph Herter (Department of Medicine, Kristiansund sykehus, Kristiansund, Norway).