
Abstract
Background
Clostridium difficile infection (CDI) is an increasingly common cause of inpatient mortality. Vitamin D deficiency is associated with more aggressive CDI. We aimed to determine if average annual ultraviolet light (UV) exposure was associated with mortality in patients with CDI.
Methods
We used the US National Inpatient Sample (NIS) from 2004–2011 to assess the mortality risk in patients with a diagnosis of CDI (as per ICD-9CM 008.45). Annual average state UV exposure was assigned to each hospitalization. Logistic regression was used to determine the effects of UV exposure on mortality, controlling for age, gender, race and other comorbidities.
Results
During the study period, there were 2.61 million hospitalizations with a diagnosis of CDI. The mortality rate was 9.0%. In univariate analysis, the odds ratio (OR) of inpatient mortality for the UV index was 0.97 (95% CI 0.95–0.99; p = 0.008) per unit of UV exposure. In a multivariable model adjusting for age, gender, race, Charlson-Deyo index, season and coexisting inflammatory bowel disease, the UV index remained a protective predictor, with an OR of 0.94 (95% CI 0.92–0.96; p < 0.001). In the multivariate model, a seasonal effect was also present, with the highest risk of inpatient mortality in the period from January to March (OR 1.11; 95% CI 1.08–1.14) and the lowest risk, from July to September (OR 0.95; 95% CI 0.92–0.98).
Conclusions
An increase in UV exposure index is associated with a reduced risk of inpatient mortality in patients with CDI. A seasonal effect is also present, with the highest risk of death during winter months. Further studies exploring the role of UV light in CDI are necessary.
Background
Clostridium difficile infection (CDI) is the most common cause of infectious colitis in the USA, with a fatality rate that increased from 1.2% in 2000 to 2.2% in 2004. 1 Risk factors for CDI include age, prior hospitalizations, prior antibiotic use, proton pump inhibitor use, 2 inflammatory bowel diseases (IBD) 3 ; and more recently, there is also data to suggest that patients with lower vitamin D levels have a more aggressive CDI course. 4
The importance of vitamin D in diseases beyond calcium homeostasis and bone health is becoming more apparent. Vitamin D has been found to have an antimicrobial effect, aiding the macrophage suppression of mycobacterial growth, in in vitro experiments. 5 This inhibition is believed to be mediated through the induction of cathelicidin, an antimicrobial peptide.6,7 Recent in vitro and in vivo experiments in mice demonstrate that exogenous administration of cathelicidin could suppress intestinal damage due to CDI. 8 In epidemiological studies of patients who are critically ill, vitamin D deficiency is found to be a risk factor for mortality. 9 Additionally, studies of vitamin D and CDI suggest that patients with vitamin D deficiency have longer hospitalizations and increased healthcare-associated costs. 4
Sunlight, in the form of ultraviolet (UV) radiation, provides a major source of vitamin D; UV-B radiation converts 7-dehydrocholesterol into pre-vitamin D, which is later converted to vitamin D3. 10 The broad importance of vitamin D in gut immunity is highlighted by the finding of an inverse relationship between vitamin D levels and the risk of diverticulitis. 11 We aimed to study whether UV light exposure is related to CDI inpatient mortality, using the US National Inpatient Sample (NIS) data from 2004 to 2011. We hypothesized that patients in areas with more UV light exposure will have lower mortality, adjusting for age, gender and other comorbidities.
Methods
The NIS is a de-identified dataset of a 20% stratified sample of inpatient hospitalizations. For this analysis, the 2004–2011 NIS datasets were used for analysis. Each hospitalization is characterized as a single record, with discharge diagnoses, procedure codes and socioeconomic data. The data abstraction process to obtain UV exposure is described in detail, in a prior publication. 12 Briefly, annual UV light exposure was obtained from published maps by the US Environmental Protection Agency (EPA). 13 These maps showed the average UV index for each month, from 2006–2010; the map was divided into 144 cells, which were then matched to the corresponding 3-digit zip code (the first three digits of the 5-digit zip code, designating one area within a state). We calculated the average annual values per 3-digit zip code. These values were then validated, by comparing the results to the 12-year average for 500 cities around the country. The level of UV exposure was characterized by measurement of the UV index. The UV index is a linear-scale prediction of the ground level UV radiation, factoring in elevation, cloud cover, ozone levels developed by the US EPA and the US National Oceanic and Atmospheric Association (NOAA). 14 This value ranges from 0 to greater than 11. As the zip-code level data is only available for the hospital location, and not for the patient’s home; and that data is missing from 31.4% of hospitalizations, we elected to calculate a state UV index average to apply to each hospitalization. We calculated a Charlson-Deyo comorbidity score for each hospitalization, in order to factor in the effects of comorbidities on the risk of mortality. 15 We analyzed all hospitalizations where CDI was a primary or a secondary diagnosis (based on ICD9-CM code 008.45), as studies show that primary ICD-9CM codes are valid and reliable in large administrative datasets.16,17 In order to compare hospitalization numbers across the country, the UV index was categorized into approximately equal population tertiles. We used US Census data from 2010 to determine state populations. Ulcerative colitis (UC) was classified as a diagnosis of ICD-9CM code 556.X and Crohn’s disease was classified as a diagnosis of ICD-9CM code 555.X. The ICD9-CM diagnosis codes used for infection are located in Supplementary Table 1.
Statistical analysis
We performed the statistical analysis using SAS 9.3 (Cary, NC, USA). The appropriate PROC SURVEY commands were used, in order to generate national estimates. The baseline characteristics of the population were compared with the Rao-Scott chi-square test for categorical variables or the student’s t-test for numerical variables. We performed both univariate and multivariate logistic regression analysis, using PROC SURVEYLOGISTIC, to determine individual effects as odds ratios (ORs). All major clinical characteristics and demographic characteristics were combined in the multivariable model.
Results
Baseline characteristics
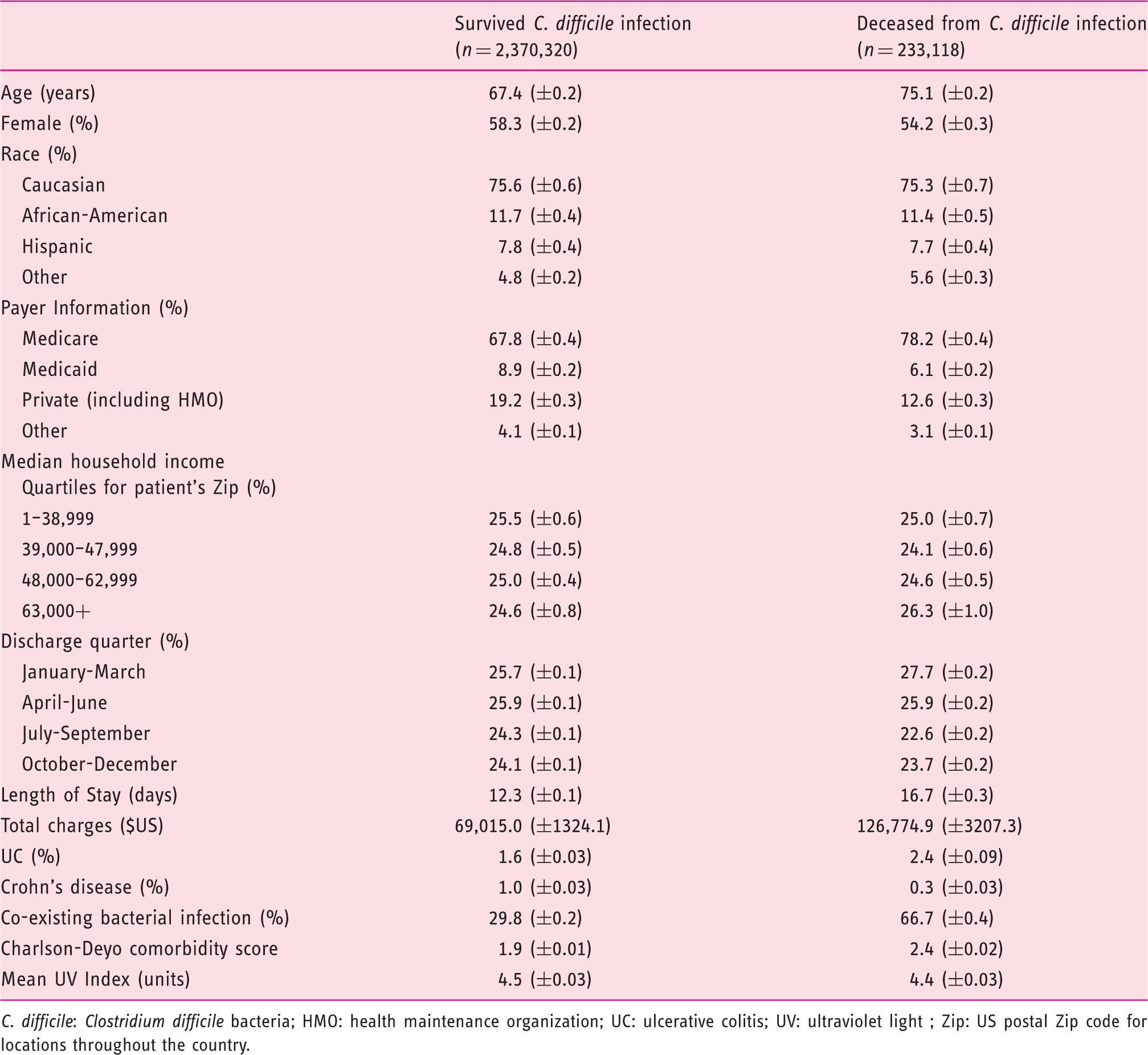
C. difficile: Clostridium difficile bacteria; HMO: health maintenance organization; UC: ulcerative colitis; UV: ultraviolet light ; Zip: US postal Zip code for locations throughout the country.
The average national population-adjusted UV Index was 4.59 (2010 US Census data). On the state level, the average yearly UV Index ranged from 0.66 units in AK, to 9.3 units in HI (Figure 1(a)). The average UV exposure among hospitalizations that led to mortality was lower (4.4 UV Index units versus 4.5, p = 0.009).
Color-coded geographic map of the USA demonstrates the average UV Index exposure per state, categorized by approximately equal population tertiles. (a) The highest area of UV light exposure in the continental US is centered in the Southwest.
18
(b) The percentage breakdown of primary or secondary CDI diagnoses over the UV Index tertiles was statistically different from the breakdown of hospitalizations without a CDI diagnosis. Source: Govani SM, Higgins PDR, Stidham RW, et al. Increased Ultraviolet Light Exposure is Associated with Reduced Risk of Inpatient Surgery Among Patients with Crohn’s Disease. J Crohn’s Colitis. 2015; 9: 77–81.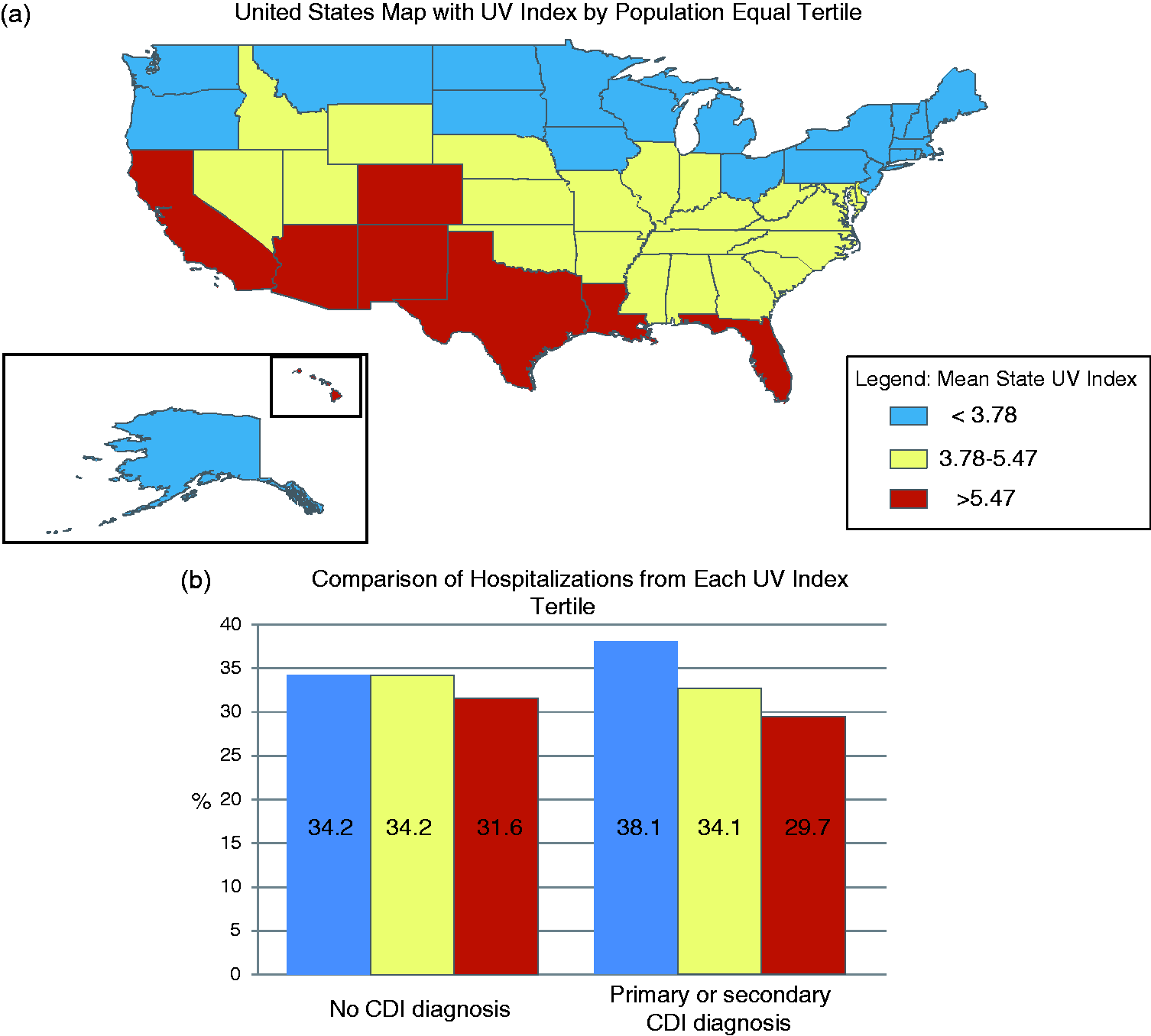
Comparing the proportions of hospitalizations, we found there was a significant difference in the percentage of hospitalizations across UV Index tertiles for CDI, as compared to all hospitalizations (p < 0.001). The largest proportion of hospitalizations was in the lowest tertile of UV exposure (Figure 1(b)).
Univariate ORs of inpatient mortality in patients with CDI
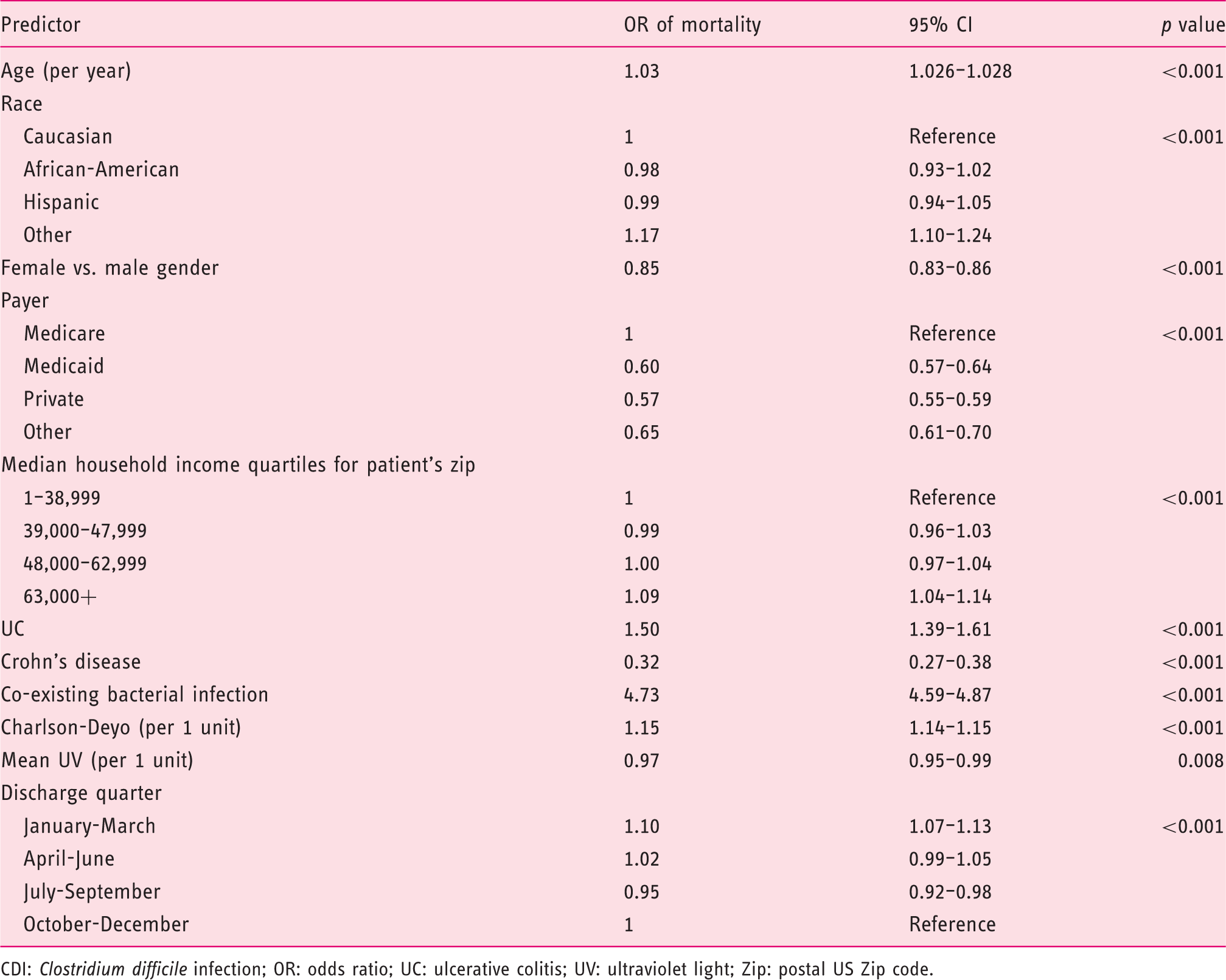
CDI: Clostridium difficile infection; OR: odds ratio; UC: ulcerative colitis; UV: ultraviolet light; Zip: postal US Zip code.
Multivariate ORs of inpatient mortality among patients with CDI
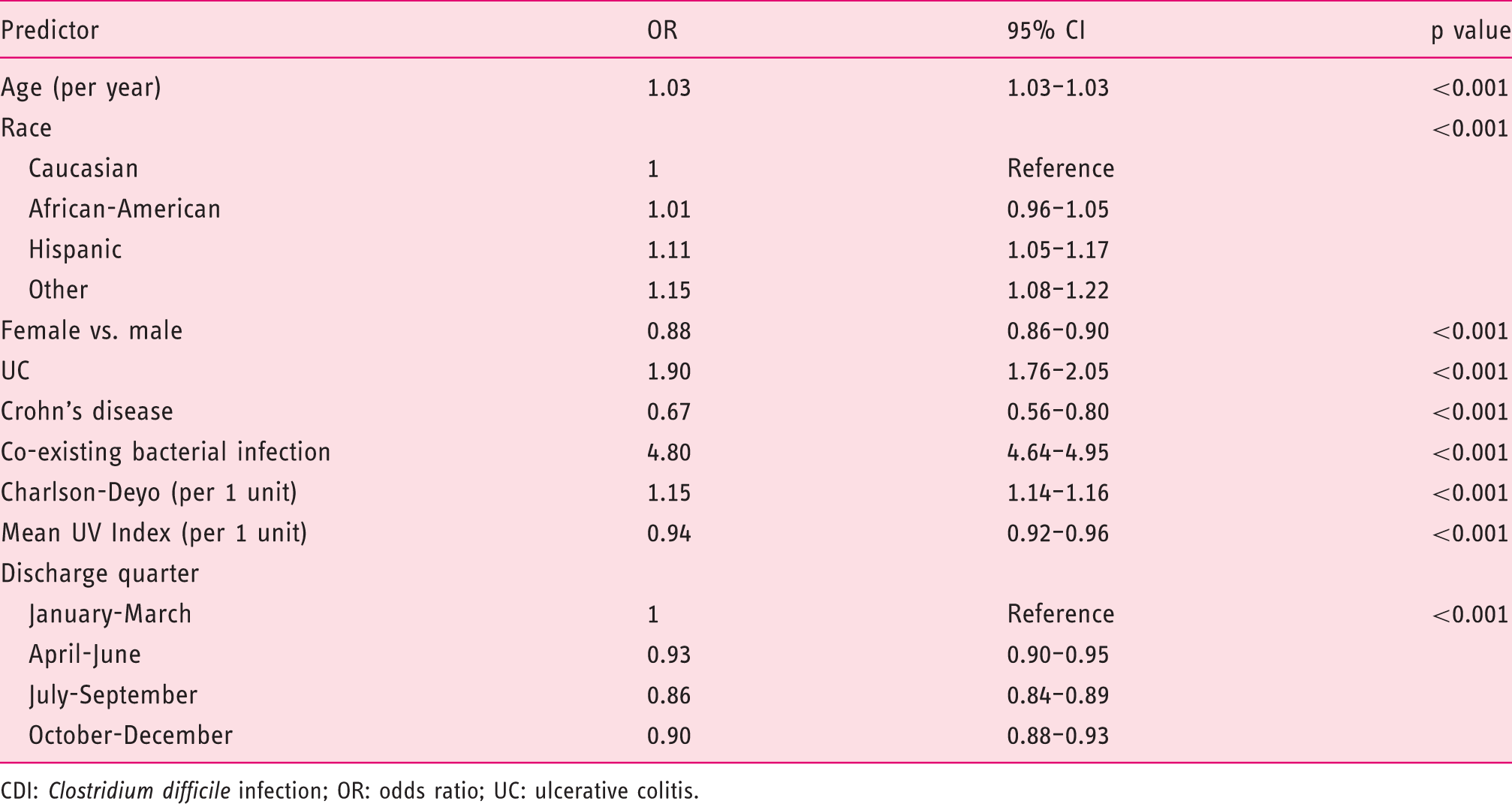
CDI: Clostridium difficile infection; OR: odds ratio; UC: ulcerative colitis.
Sensitivity analysis: Multivariate Modela of Mortality due to CDI, with various UV exposure variables
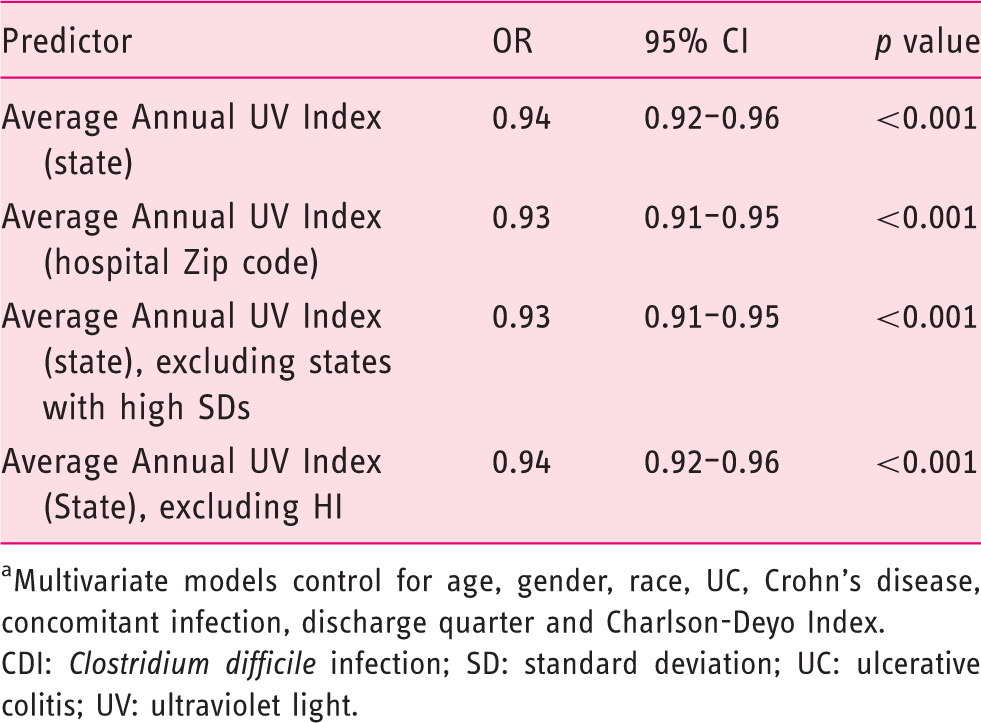
aMultivariate models control for age, gender, race, UC, Crohn’s disease, concomitant infection, discharge quarter and Charlson-Deyo Index.
CDI: Clostridium difficile infection; SD: standard deviation; UC: ulcerative colitis; UV: ultraviolet light.
Finally, we repeated our analysis excluding the state of HI, due to the fact that the average annual UV Index is much higher and the number of CDI-related deaths in HI was quite low. This analysis again showed a protective effect in a multivariate analysis (OR = 0.94; 95% CI 0.92–0.96). When only hospitalizations with a primary diagnosis of CDI were considered in our analysis, UV Index again demonstrated a protective association with inpatient mortality (OR = 0.92; 95% CI 0.88–0.96; p < 0.001). In contrast to the association between UV exposure and CDI mortality, an examination of all hospitalizations during the 8-year period found that UV Index was not protective of all-cause inpatient mortality (OR = 1.00; 95% CI 0.98–1.02; p = 1.00).
Discussion
In this ecological study of NIS data from 2004–2011, we found an inverse relationship between inpatient mortality and the average yearly UV Index exposure in patients with a diagnosis of CDI. Based on the estimates from our logistic model, a patient from AZ is 16% less likely to die in the hospital from CDI than a patient of the same age, gender and other comorbidities in MI.
While there are a number of studies showing an association between latitude and the incidence of inflammatory bowel diseases,19,20 this is the first study that we know of that has examined the association between UV exposure and hospitalizations for CDI. The strengths of this study include the size of the database, which represents more than 200 million hospitalizations in the US over an 8-year period and includes extensive discharge diagnosis data, demographics and comorbidity data. The significance of discharge quarter in the multivariable model is further evidence that the protective effect of UV light may be mediated through vitamin D. A recent study of the season variation of vitamin D revealed a peak serum vitamin D in August and a nadir in February. 21 Our study found that the last quarter of the year had lower inpatient mortality, which could be due to the delayed response of vitamin D levels to summer UV exposure.
The study’s major limitations included the fact that it was based on administrative data, which may have imperfect discharge coding, and that the associations seen here could possibly be due to another unknown factor. We focused our analysis on hospitalizations with primary or secondary diagnoses of CDI, in order to capture patients in whom CDI was the major diagnosis (and therefore, a main contributor to mortality). We note that the mortality rate among patients with a primary diagnosis of CDI is 3.5%, which is lower than the mortality rate among those with a secondary diagnosis (11.3%). While we studied the association between UV and mortality among patients with CDI, we do not have a method to determine whether the cause of death was due to CDI; however, the association between UV exposure and inpatient mortality was stronger for patients with only a primary diagnosis of CDI. Our data cannot account for migratory patterns of Americans or other confounding exposures that may be more likely to occur in the US South/Southwest and could be protective against CDI mortality. Additionally, the dataset did not allow for adjustment for other important predictors of CDI, such as serum albumin, proton pump inhibitor use or white blood cell count.
While we hypothesize that the protective effect of UV light on CDI mortality is mediated through increased levels of vitamin D, it is possible that sunlight and/or warmth itself may have some protective effect. It is also possible that an indirectly associated factor, i.e. use of sunscreen, could be protective rather than UV light or vitamin D. In animal models of multiple sclerosis, an autoimmune disease with similar geographic associations as CD, it was shown that UV light has a beneficial effect, independent of vitamin D levels.22,23
Future studies will need to be done in other large datasets, to see if the relationship between CDI mortality and UV light persists. With the increasing incidence of CDI and the high prevalence of vitamin D deficiency in the elderly population, further research is needed to confirm this association and to determine whether interventions such as vitamin D supplementation can change CDI outcomes.
Footnotes
Funding statement
This work was supported by the Inflammatory Bowel Disease Working Group through an unrestricted educational grant by UCB Inc (GI Fellows Research Award to SMG) and the US Veterans’ Administration (VA HSR&D CDA-2 Career Development Award number 1IK2HX000775, to AKS).
Conflict of interest
The authors declare that there are no conflicts of interest.
Acknowledgements
We would like to acknowledge Scott Montain, from the US Army Research Institute of Environmental Medicine, for sharing his UV data with us.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.