
Abstract
Objective
The objective of this article is to assess the prevalence of somatic symptoms and of gastrointestinal (GI) syndromes in abused “non-patient” women and the association with the time of perpetration, type, and severity of abuse.
Methods
Sixty-seven women, 18–58 years, receiving shelter in anti-violence associations were invited to fill out an anonymous questionnaire with a medical and an abuse section. The severity of abuse was expressed as the 0–6 Abuse Severity Measure (ASM). The association between abuse characteristics and the number of symptoms, and GI syndromes was assessed by Poisson regression model.
Results
Most women suffered from childhood and adulthood sexual and physical abuse. They reported a mean of 5.1 GI symptoms (range 0–13; median 5; IQR 6) and of 1.3 extra-GI symptoms (range 0–6; median 1; IQR 2); 30% of women matched the Rome II Criteria for one, 36% for two, and 4.4% for three or more syndromes, respectively. Women with an ASM of 5–6, having suffered from both sexual and physical abuse, reported significantly (p = 0.02) more GI symptoms, but not extra-GI ones (p = 0.07), and met criteria for more GI syndromes than women with an ASM ≤4 and those reporting only one type of abuse. No association was found between the time of perpetration of the abuse and the number of GI and extra-GI symptoms.
Conclusions
Symptoms in abused “non-patient” women mainly concern the abdomen and the GI tract. A history of severe, combined physical and sexual abuse is associated with a higher number of GI symptoms.
Keywords
Introduction
There is growing evidence suggesting an association between sexual and physical victimization and long-term health disturbances. The prevalence of violence in the general population ranges from 5% to 60% worldwide. 1 Reports from different countries indicate that 14%–55% of patients in primary care2,3 and 17%–56% of those in tertiary care4–6 have a history of sexual and/or physical violence. The wide variability of abuse prevalence rates across studies may reflect social and cultural differences in the examined populations, variations in the size and characteristics of the study sample, and discrepancies in the definition and methods used to assess the abuse history. 7 Overall, a higher prevalence of violence was found in patients vs. the general population and in tertiary vs. primary care patients.
Several studies8–10 have reported an association of lifetime sexual and/or physical abuse and their severity with multiple medical complaints, chronic pain, poor daily functioning, limited response to medical treatment, unnecessary surgery, and psychopathological correlates, such as somatization. In 1996, the World Health Organization Assembly declared violence as a major global public health issue and called for increasing action. In 2002 the World Health Organization released the first World Report on Violence and Health.
To date, several studies have investigated the prevalence of chronic medical complaints in abused patients,4–6,8–10 but only a few have focused on abused “non-patient” individuals,11–14 i.e. people not referring to a doctor. The prevalence of chronic symptoms in severely abused “non-patient” women forced to apply for housing in anti-violence centers is currently unknown.
This study aims to assess in “non-patient” women subjected to severe sexual and/or physical victimization and being offered shelter and aid by anti-violence associations:
the prevalence of reported gastrointestinal (GI) and extra-GI symptoms, and GI syndromes; the association, if any, between the time of perpetration of abuse, its type and severity, and the number of reported symptoms, and GI syndromes.
Participants and methods
Five Italian anti-violence associations were contacted, three of which agreed to participate in this study: “Artemisia” (Florence), “Differenza Donna” (Rome) and “UDI Casa delle Moire” (Palermo). In the anti-violence centers, victimized women receive shelter, legal advice, and psychosocial support from female operators.
After providing free, informed consent, women were asked to fill out an anonymous standardized questionnaire. To preserve privacy, the questionnaire was mailed to the centers and handled exclusively by specifically trained operators. The questionnaire was submitted to women who had already received counseling by the in-house operators.
The questionnaire consists of two separate sections, a medical and an abuse one, with the same identification code. The medical section includes five items on past and chronic diseases, past surgery, health care use in the past year, chronic drug use, seven socio-demographic items, and 46 items for GI symptoms (32 items), divided into six categories (i.e. esophageal, gastroduodenal, intestinal, anorectal, biliary symptoms, and abdominal pain), and of extra-GI symptoms (14 items), in particular urinary and gynecological symptoms (i.e. dysuria, strangury, nycturia, urinary urgency and incontinence, dyspareunia, dysmenorrhea, and pelvic pain). GI symptoms were asked about and analyzed by means of the validated Italian version of the Rome II Modular Questionnaire 15 (www.theromefoundation.org). GI symptoms were taken into account both individually and when constituting a clinical syndrome that matched the Rome II Criteria (dyspepsia, irritable bowel syndrome (IBS), chronic abdominal pain, functional diarrhea, functional constipation) or criteria for gastroesophageal reflux disease.15,16 Self-perceived severity of abdominal pain was evaluated by means of a visual analog scale (VAS), ranging from 0 (“no pain at all”) to 10 (“very severe pain”).
The abuse section consists of the Italian version of the Sexual and Physical Abuse History Questionnaire. 17 Proper understanding of the questions was previously verified by a gastroenterologist (NP) who matched 10 control individuals’ interviews and questionnaire responses. Test-retest reliability 18 was verified by re-submitting the questionnaire to the same control participants three weeks later. Based on the abuse questionnaire items, an Abuse Severity Measure (ASM) was derived. 19 The ASM quantifies the severity of sexual and physical abuse, on a scale from 0 to 6, assessing history of sexual abuse (score of 0 = none, l = touch, 2 = rape), serious injury during sexual abuse (score of 0 = no injury or minor injury, 2 = serious physical injury), and number of life-threats deriving from physical attack (score of 0 = none, 1 = from one to three life threats, 2 = four or more life threats). The ASM has been shown to correlate with health status within each of the above dimensions. 19
Informed consent was obtained from each participant and the study protocol was approved by the local ethics committee of our university hospital.
Statistical analysis
Continuous variables were summarized as median, interquartile range (IQR) or mean (M) and standard deviation (SD); categorical variables were summarized as absolute and percentage values. Differences in baseline characteristics were determined by Pearson’s chi-square test and Fisher’s exact test.
A Poisson regression model was used to assess the association between number of reported GI and extra-GI symptoms, and GI syndromes and variables as time of perpetration of the abuse (childhood, i.e. ≤13 years, vs. adulthood, i.e. >13 years, vs. childhood and adulthood), its type (sexual vs. physical vs. sexual and physical) and severity (defined according to the ASM: as ordinal, i.e. 0–6 (results not shown), or dichotomous, i.e. ASM ≤4 vs. ASM 5–6), and socio-demographic characteristics (i.e. age, level of education, economic self-sufficiency, body mass index (BMI), smoking habit, alcohol consumption). In the model, if only one variable is taken into account, univariate results are obtained; if more variables are taken into account, in order to evaluate their independent effect having simultaneously adjusted for the effects of the other variables, multivariate results are obtained.
Significance was set at p < 0.05. All p values were two tailed. The R statistical software release 2.15.3 (Foundation for Statistical Computing, Vienna, Austria) 20 was used to perform analyses.
Results
Study sample
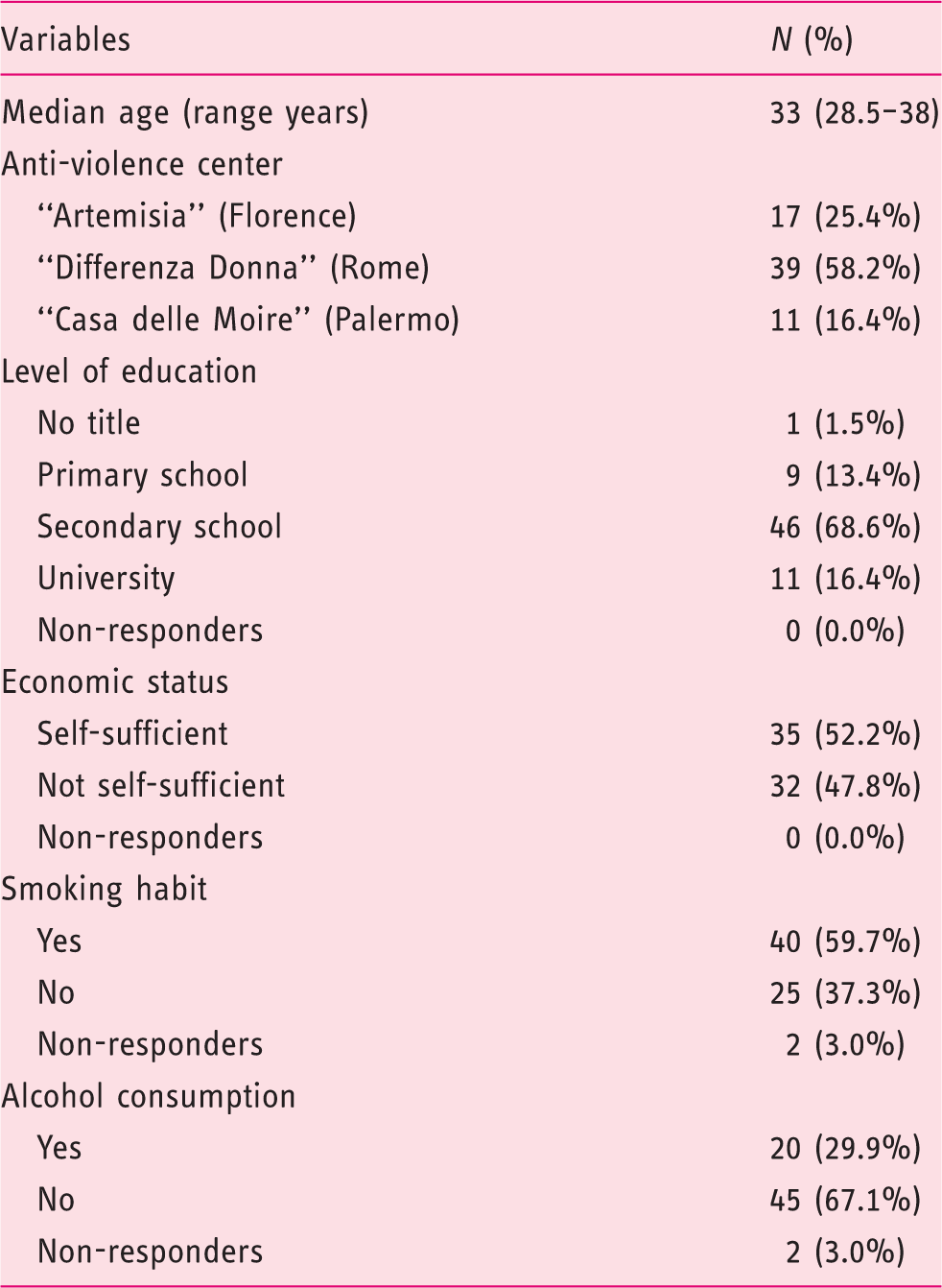
Socio-demographic characteristics of the study sample
Abuse history
Distribution of the women according to the type and the time of perpetration of abuse

Taking into account the severity of abuse, 18% (12/67) of the women scored 1 on the ASM, 18% (12/67) scored 2, 10% (seven of 67) scored 3, 13% (nine of 67) scored 4, 5% (three of 67) scored 5, and 36% (24/67) scored 6. Mean ASM was 3.76 ± 1.98 (M ± SD), median was 4 (IQR = 3).
Distribution of the women according to Abuse Severity Measure (ASM) and type of abuse

The perpetrator of the abuse was indicated to be the current or former partner or a relative by 58 (86.6%) women. More specifically, childhood abuse was perpetrated by a relative in 90.8% of cases and adulthood abuse by a partner in 82.5% of cases.
Prevalence of GI and extra-GI symptoms, and GI syndromes
Women reported a mean of 5.1 GI symptoms (range = 0–13; median = 5; IQR = 6) and of 1.3 extra-GI symptoms (range = 0–6; median = 1; IQR = 2). Four (6%) women did not report any GI symptom, 29 (43%) reported one to four GI symptoms, 14 (21%) five to seven symptoms, 17 (25%) eight to 12 symptoms and three (6%) ≥13 symptoms. Twenty-eight (42%) women did not report any extra-GI (urinary and/or gynecological) symptom, 27 (40%) reported one to two extra-GI symptoms, 11 (16%) three to five symptoms and one ≥6 symptoms.
Twenty (29.8%) women did not match criteria for any GI syndrome, 20 (29.8%) matched criteria for one syndrome, 24 (36%) for two syndromes, and three (4.4%) for ≥3 syndromes.
Number and proportion of women reporting gastrointestinal symptoms

Number and proportion of women reporting extra-gastrointestinal symptoms

Prevalence of gastrointestinal (GI) syndromes
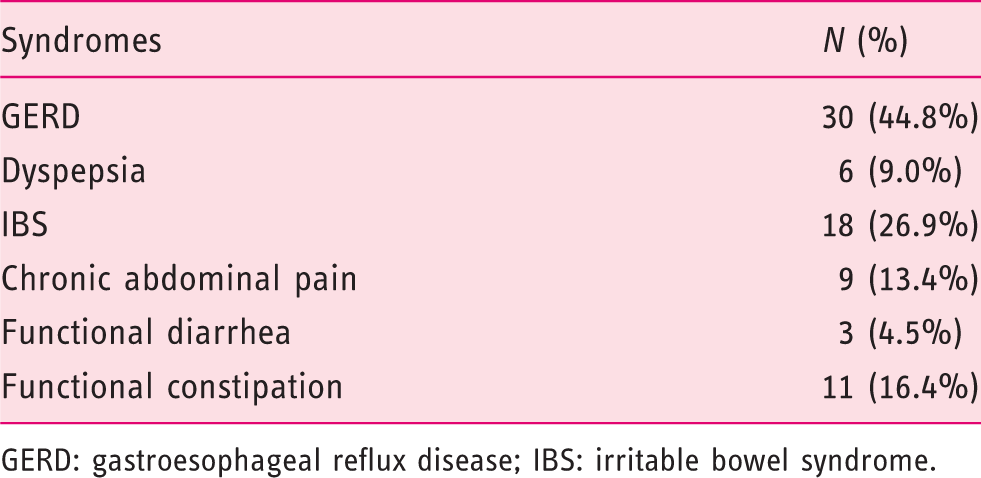
GERD: gastroesophageal reflux disease; IBS: irritable bowel syndrome.
Mean self-perceived abdominal pain, as assessed with the VAS, was 3.36 ± 3.62 (M ± DS), corresponding to “mild-to-moderate pain.”
Association between abuse and symptoms/syndromes
Women scoring 5–6 on the ASM reported significantly more GI symptoms and met criteria for significantly more GI syndromes than women scoring ≤4 (p < 0.05), whereas the two ASM groups did not differ for the number of extra-GI symptoms (Figure 1(a) and (b)).
(a) Box-and-whiskers plots of number of gastrointestinal (GI) symptom according to Abuse Severity Measure (ASM). The boxes at each score extend from the 25th percentile (x[25]) to the 75th percentile (x[75]) (i.e. the interquartile range (IQ)); the lines inside the boxes represent the median values. The line emerging from the boxes (i.e. the “whiskers”) extend to the upper and lower adjacent values. The upper adjacent value is defined as the largest data point ≤x[75] + 1.5 × IQ, and the lower adjacent value is defined as the smallest data point ≥x[25] – 1.5 × IQ. Observed values more extreme than the adjacent values, if any, are individually plotted (circles). * p < 0.05 for all comparisons. 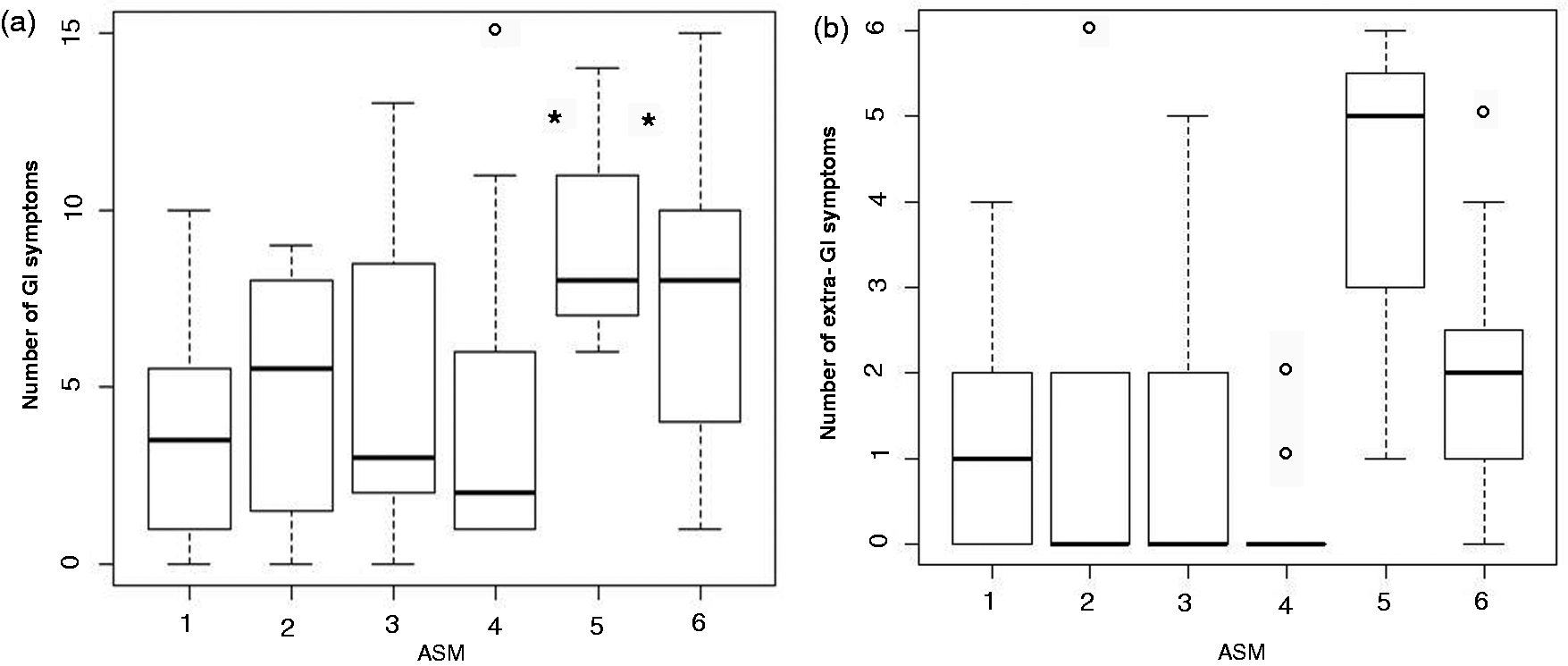
Association between socio-demographic characteristics, abuse history and the total number of reported gastrointestinal (GI) and extra-gastrointestinal (extra-GI) symptoms and GI syndromes
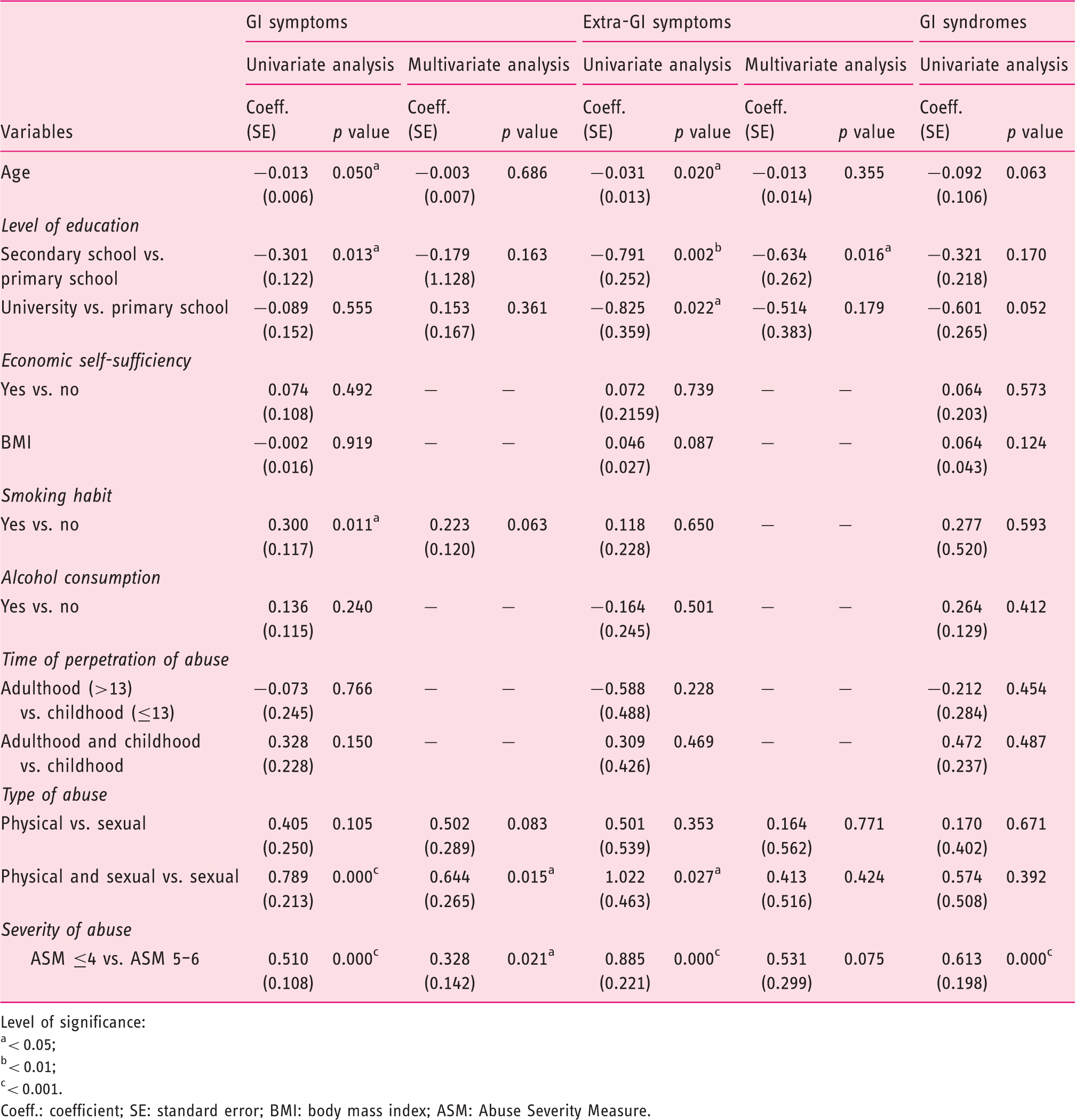
Level of significance:
< 0.05;
< 0.01;
< 0.001.
Coeff.: coefficient; SE: standard error; BMI: body mass index; ASM: Abuse Severity Measure.
At univariate analysis women scoring 5–6 on the ASM reported a statistically significant higher number of GI syndromes than those scoring ≤4 (p = 0.000) (Table 5). The association between abuse history, socio-demographic characteristics, and the number of GI syndromes was not tested at multivariate analysis since no significant association was found between these variables at univariate analysis.
Discussion
A large body of literature highlights that violence has long-term negative health consequences, even after it has ended. An abuse history can lead to poorer physical and psychological status, lower quality of life, higher levels of disability in all areas of functioning, and higher utilization of public health services.8,9,21
The lifetime prevalence of physical and sexual victimization and its relationship with medical complaints vary widely according to the population involved and to the evaluation methods employed. Several studies performed in patient populations have investigated abuse history through self-report questionnaires, others through interviews. Although interviews may be considered the gold standard, it has been shown that the prevalence of abuse was under-reported in medical charts compared to self-reported questionnaires in a population-based cross-sectional study, 11 and in abuse questionnaires where identity was not sufficiently concealed compared to anonymous ones in a GI outpatient study. 6
A strength of the present study is that all the evaluated women were victims of such severe and repeated violence that they had to leave their homes and abusers, thus reducing the risk of possible biased reporting on violence experience.
A minority of women reported childhood-only and one-fourth adulthood-only sexual and/or physical abuse. In more than half of the women, the sexual and/or physical abuse began in childhood and persisted during adulthood. In about 90% of cases, the perpetrator of the abuse was a current/former partner or a relative of women subjected to childhood abuse.
Drossman et al. 5 detected a strong association between functional bowel disorders and sexual or physical abuse in outpatient women, whereas Baccini et al. 6 found an association in all patients with chronic GI diseases, irrespective of functional or organic diagnosis.
To our knowledge, this is the first study to provide in “non-patient” severely abused women requiring shelter in dedicated centers the prevalence of chronic symptoms, as well as the association between their number and the different characteristics of abuse.
More than half of the sample reported at least four GI symptoms and about one-fifth at least three uro-gynecological symptoms. Two women out of three met criteria for at least one GI syndrome. Although these analyses were not replicated in a sample of healthy controls in order to perform comparisons, the rates of GI symptoms and syndromes were found to be much higher than those expected in the general population 22 and are in line with the high prevalence of dyspepsia (67%) and IBS (47%) in 70 women reporting intimate partner violence (IPV) to the police. 13 Whether the association between abuse experience and physical disturbances reflects a cause-effect relationship or just an excessive reporting behavior is unclear. Yet the women of our sample, who did not require medical assistance or treatments, may be less likely than patients to over-report disturbances and to link life negative experience to their medical conditions. 23
It is noteworthy that most symptoms concern the GI tract, and, in particular, the abdomen. It has been suggested that abuse via high levels of neuroticism, (i.e. a long-term tendency to be in a negative emotional state), may determine anxiety and mood disorders in GI patients. These disorders increase abdominal pain reporting, which, in a “vicious circle,” increases GI symptoms over time. 23 The association between abuse and GI symptoms could also reflect the relationship between abuse history and somatization.9,23 Alternatively abuse may determine biological alterations in addition to, or instead of, psychological ones. Abdominal pain could be explained by the stress-mediated release of substances through the brain-gut axis/neuroendocrine activation, such as catecholamines, corticotrophin-releasing factor, and prostaglandins that modify the sensory-motor function of the GI tract. 24 Indeed, compared to non-abused GI patients, abused ones show significantly lower peripheral pain threshold levels, 25 and in those with unexplained abdominal pain and subjected to physical abuse gut distension is associated with increased pain and changes in central pain processing. 26 Lastly, abdominal injury caused by physical abuse may induce long-lasting changes in nociception. 27
The present study shows that combined sexual and physical abuse is associated with more GI symptoms than either one alone. These results are in line with those of preceding studies showing a direct relationship between the number of experienced episodes of violence and the number of GI and extra-GI symptoms, 28 and a significant association between multiple types of violence and a poorer individual’s health status. 9
Several studies10,19,21 found that the difference in terms of health status between abused and non-abused female patients was particularly striking in those with severe forms of violence (i.e. rape and life-threatening events). In our study, 40% of women scored 5–6 on the ASM and there appears to be a link between the severity and type of abuse. The observation that a combination of sexual and physical violence, as well as a greater severity of violence as measured by the ASM, are significantly and independently associated at the multivariate analysis with a higher number of GI and extra-GI symptoms, and at the univariate analysis with a higher number of GI syndromes, is in line with the findings of Leserman et al.10,21 in patient populations. Thus the ASM appears to be a useful and reliable tool to be employed in future studies to rate violence and identify severely abused individuals who are at a higher risk of medical disturbances, regardless of any request for health assistance.
A history of childhood abuse may contribute to multiple chronic complaints in adult women; 29 however, the association between an early age of abuse and the later onset of health problems has been found in cross-sectional studies, 30 but not confirmed by Walker et al., 31 Rimsza et al., 32 and Briere and Runtz, 12 who conducted observational studies. In the present study childhood abuse did not affect the number of symptoms reported in adulthood. Furthermore, differently from a previous report, 9 we did not observe worse health outcomes deriving from combined childhood and adulthood abuse in terms of number of symptoms or GI syndromes. However, the observation that more than half of our sample suffered from violence during both childhood and adulthood is in line with the suggestion that the experience of abuse in childhood increases the risk of abuse in adulthood.
In a population-based study, Bytzer et al. 33 found a pronounced effect of socio-economic status on the prevalence of GI symptoms, with more symptoms reported by socially disadvantaged individuals. At the multivariate analysis, we did not find any relationship between socio-demographic variables (i.e. age, BMI, smoking, alcohol, socio-economic status, and self-perceived stress), and the number of GI and extra-GI symptoms, and GI syndromes.
This study has several limitations because of the particular population investigated. Namely, a complete medical history and the presence of mental health conditions, such as anxiety, post-traumatic stress disorder, mood disorders, or somatoform disorders, were not assessed. Substance abuse was just inquired about in the questionnaire, but we cannot reasonably exclude it. Moreover, we did not evaluate psychological abuse, which is known to affect health status not differently from sexual and physical abuse, as it is often difficult to separate it from them.
Because of the small sample size and the lack of a control group, the findings of the present study cannot be extended to, and compared to, the community or to patient populations. In a previous study performed in Italian abused patients with chronic GI diseases, the number of reported GI symptoms was 8.6 ± 3.3 and the number of extra-GI symptoms was 4.3 ± 2.4. 6 Its cross-sectional design does not allow us to draw any causal or temporal relationship between violence exposure and poor health outcomes. All participants were women, hence, our results do not extend to men, and consequently we could not assess the role of gender in experiencing abuse and symptom occurrence. Finally, our sample is not representative of all the women referring to anti-violence centers, since not all contacted centers agreed to take part in the study and only those women who had already received counseling were included. Thus, we cannot exclude a selection bias that may have affected the results.
Despite these limitations, the present study highlights two relevant aspects. The first one is that abused women mainly report symptoms of the GI tract, in particular of the abdomen; the second one is the correlation of higher abuse scores with greater GI symptomatology. In conclusion, our data underline the importance of inquiring about abuse history in patients with multiple chronic GI complaints.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.
Acknowledgments
The authors acknowledge the Anti-Violence Associations Artemisia, Differenza Donna, and Casa delle Moire for collaborating with us and making possible the realization of this research project.