
Abstract
Background
Substance use at UK music festivals presents a significant public health challenge, with evolving patterns of drug use, associated risk behaviours, and harm reduction practices among attendees.
Methods
A sample of UK festival attendees (N = 773) completed a lengthy online survey detailing their typical substance use practices and related behaviours within music festival contexts.
Results
This study reports patterns in substance preferences and polysubstance use combinations, where younger individuals report the use of novel substances, while older attendees to use more historically popular drugs. Users of ketamine (z = −10.58, P < .001), or novel psychoactive substances (z = −4.23, P < .001) were significantly younger than non-users. The findings highlight the prevalence of alcohol use (92.8%, N = 718), and polysubstance use (60.7%, N = 476). Alcohol was particularly prevalent within the context of polysubstance use (71.6%, N = 341). Notably, polysubstance use involving the combined use of five substances (alcohol, cocaine, cannabis, ketamine, and MDMA) during the same period was concerningly common among those engaging in polysubstance use (25%, N = 119). The study identified a lack of engagement with critical harm reduction practices and provisions, such as accessing drug checking services (N = 53, 6.7%) or onsite welfare provisions (N = 82, 10.6%).
Conclusions
The low reports of accessing formal onsite services suggests the need for improved educational outreach and the potential to enhance engagement through informal online platforms. This study highlights the importance of context-specific drug use patterns and targeted interventions, aiming to facilitate more effective public health responses. These findings indicate the necessity for adaptive and targeted interventions, particularly those addressing alcohol consumption, polysubstance use, and the promotion of early help-seeking.
Introduction
Substance use at music festivals is a growing public health concern in the UK, where these events have become culturally significant. Festivals involve large gatherings over several days, exposing attendees to social and environmental factors that may encourage substance use. Evidence suggests festivals are high-risk settings for drug and alcohol-related harm, with crowd density, prolonged celebration, and permissive attitudes contributing to risk (Black et al., 2020; Cooney and Measham, 2023). The liminal nature of festivals suspends normal social rules, further increasing substance misuse risk (Martinus et al., 2010; Turner et al., 2017). The transient, escapist atmosphere can lower inhibitions and promote riskier behaviours (Ponnet et al., 2024), while social norms endorsing excess and the availability of substances heighten the likelihood of binge drinking and drug use (Hesse and Tutenges, 2012). These findings align with broader research on substance use in recreational settings (Bellis et al., 2008; Hughes et al., 2008).
A Liverpool-led analysis identified 32 potential drug-related festival deaths in the UK from 2017 to 2023 (18 confirmed), averaging about 5–6 per year (Cooney and Measham, 2023). Official data remain scarce, as no centralised system exists. Published accounts describe individual incidents (e.g. two critical ecstasy overdoses at a 2018 UK festival) but reliable counts depend on media or FOI sources. On-site medical data indicate intoxication is a small fraction of cases. For instance, 164 out of 2828 medical visits at Glastonbury 2022 (5.48%) were intoxication-related (Bennett and Cottrell, 2024), and one European festival (2011–2017) reported only 5% of presentations were due to intoxication (86% of those were alcohol, 14% illicit drug; Maleczek et al., 2022)
Recent US surveys show very high festival drug use. A New York City study (2017–2022) found that by 2022 about 11% of Electric Dance Music partygoers reported past-year ketamine use (vs. 5.9% in 2017), and 24.5% reported past-year use of amyl nitrite (‘poppers’) (vs. 9.8% in 2017; Palamar et al., 2023). In Europe, research in Belgium found 44% of festivalgoers used drugs, mainly MDMA, amphetamines, and cocaine (Van Havere et al., 2011), while in the Netherlands, 38% reported drug use, primarily MDMA and cocaine. These findings underscore the prevalence of festival drug use across Western contexts. Different types of substances are often favoured by different populations, with more traditional substances remaining popular among older individuals and newer more novel substances becoming popular in younger generations (Patrick et al., 2016).
Despite existing research, there is limited evidence on substance use at UK festivals. While international studies offer insights, substance use patterns may differ due to cultural and regulatory factors (Day et al., 2018; Jenkinson et al., 2014; Southey et al., 2020). While there are UK-focused studies available (Martinus et al., 2010; Measham, 2019), some face methodological challenges that may limit their broader applicability. Additionally, there is still limited research on engagement with harm reduction strategies, such as drug checking, peer support, or medical assistance (Measham, 2019; Winstock et al., 2018). Higher frequency and levels of substance use at music festivals, for longer periods, can have serious consequences even resulting in death (Cooney and Measham, 2023).
This study aims to quantify self-reported substance use at UK festivals, focusing on (a) patterns and frequency, (b) substance-related risk behaviours, and (c) personal harm reduction and help-seeking. A clearer understanding of these behaviours will help address public health challenges and inform targeted, evidence-based interventions to improve festival safety.
Method
A single-time-point online survey gathered data on participants’ substance use at UK festivals over the past year, along with their awareness of risks, personal risk behaviours, use of harm reduction services, and onsite support.
Procedure
Ethical approval was obtained from Swansea University (Ref: 2368), following the Ethics Guidelines for Internet-Mediated Research (The British Psychological Society, 2021). The study was promoted via social media, university posters, and at six UK festivals within onsite support services. Participants accessed an information sheet before providing informed consent to complete the survey. Participants were required to provide information at the beginning of the survey about which UK festival they had attended and were reporting their substance use in relation to. A debrief page with research team contacts and harm reduction resources was provided upon completion.
Materials
Participants were required to complete demographic questions (age, gender, education, ethnicity, and relationship status). Additionally, participants completed standardised scales reporting their personality traits and values (Ten Item Personality Index & Ten Item Values Index; Gosling et al., 2003). Participants were then required to complete a questionnaire designed specifically for this study which enquired about their previous drug use at festivals they had attended during the previous year, any experiences of harms (e.g. medical difficulties, assault or mental health crisis) at these festivals, harm reduction strategies and help seeking while at the festivals. Some questions were nested resulting in different participant numbers for some conditional multiple-choice questions. Some text-response questions were also included to capture experiences not listed within multiple choice options. The questionnaire took approximately 30 min to complete.
Data analysis
Raw data was cleaned to remove any responses where the response time was deemed to be too quick to be genuine (less than 5 min); where all multiple-choice elements had been fully endorsed (i.e. ticking every box in the whole survey); and where responses were deemed to be disingenuous (e.g. where text responses included irrelevant or inflammatory text). Binary variables were generated from multiple-choice questions, such as whether a substance was used during a festival in the reporting period (dependent variable). Omission to some questions was allowed, resulting in differing N values. Data distribution assumptions were tested before analysis to guide statistical choices and transformations. Non-parametric tests were generally used due to the distributions found. Exploratory quantitative analysis using Mann–Whitney U, Cochran's Q, and McNemar tests examined differences in substance use (dependent variable) across demographic characteristics (independent variables) and temporal factors (e.g. festival vs. non-festival periods). Regression modelling was employed to determine predictors (independent variables such as age, gender, previous use, social context) of substance use patterns (dependent variables). Qualitative responses were clustered to identify core concepts about substance use and behaviours.
To identify predictors of high-risk polysubstance use (defined as the use of alcohol, cannabis, MDMA, ketamine, and cocaine during the same festival period), we employed a binary logistic regression using a stepwise forward likelihood ratio method. Predictor variables included demographic factors (age, gender), values (hedonism and stimulation), social and behavioural factors (e.g. number of motivations for substance use, type of festival genre attended), and prior substance use behaviour. Model performance was evaluated using Nagelkerke R² and classification accuracy, with multicollinearity diagnostics assessed through variance inflation factors (VIF).
Results
Participants
Of the 1120 participants who started the survey, 773 completed at least 75% of the survey and were included in the analysis. Participants’ ages ranged from 18 to 72 years, with the majority (61.8%) of participants under the age of 30 (M = 30.24, SD = 11.184, Skewness = 1.321, Kurtosis = 2.273). Gender distribution was roughly equal between males (N = 371) and females (N = 390); non-binary and undisclosed genders were recorded (N = 12) but not analysed separately due to small numbers. Participants were generally well-educated, with over half having completed a bachelor's degree (N = 310) or postgraduate qualification (N = 107). The most common relationship status was single (N = 275). The majority reported their ethnicity as White British (N = 643, 83.2%).
Substance use patterns
92.8% of participants reported using alcohol at music festivals in the previous year (N = 718) with almost half having also used MDMA (48.9%, N = 378) and cannabis (46.9%, N = 363) (Table 1). Cocaine was used by over a third of respondents (37.3%, N = 288), and ketamine a little under a third (29.8%, N = 230). Opioids (2.5%, N = 19) and mephedrone (1.4%, N = 11) were the least used drugs. ‘Other drug’ responses included nitrous oxide, spice, and GHB, but these were too few for separate analyses. The mean number of different substances used (including alcohol) was 3.32 (SD = 2.49, N = 776).
Frequency, gender distribution, and average age of self-reported use of substance types at UK music festivals 2018–19.
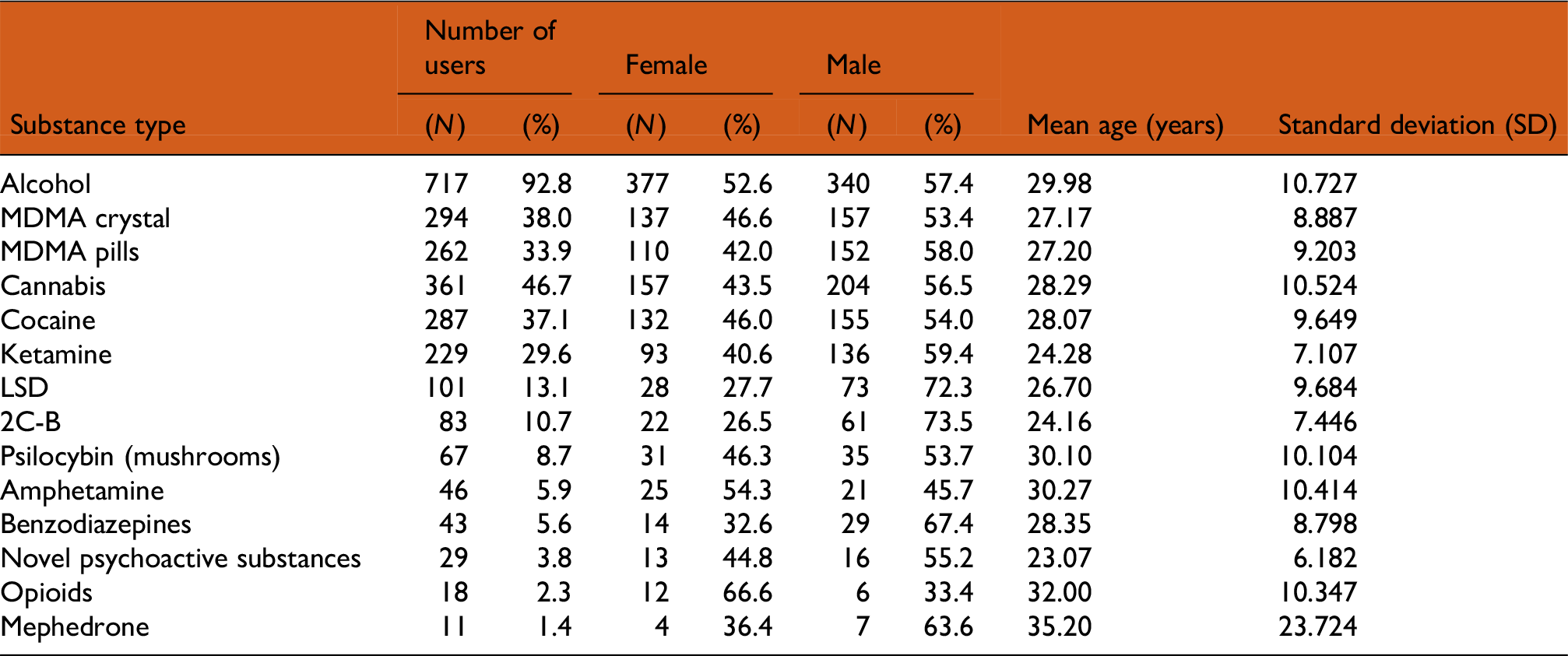
The mean age of participants varied across substance types with mephedrone, opioids, amphetamine and psilocybin having a mean participant age over 30 whilst 2C-B, ketamine, and novel psychoactive substances (NPS) had a mean age under 25. Comparison of the mean age between users and non-users for each substance type showed that users of cannabis (z = −5.23, P < .001), MDMA crystals (z = −5.81, P < .001), MDMA pills (z = 5.54, P < .001), cocaine (z = −3.95, P = <.001), ketamine (z = −10.58, P < .001), LSD (z = −3.97, P < .001), and novel psychoactive substances (z = −4.23, P < .001) were on average significantly younger than those who did not use these substances, and that those who were abstinent or used alcohol only were on average significantly older.
Male participants were more likely to use most substance types, with statistically significant differences between genders for cannabis (χ2(1) = 17.46, P < .001); LSD (χ2(1) = 26.302, P < .001); MDMA pills (χ2(1) = 14.087, P < .001); 2C-B (χ2(1) = 23.220, P < .001); and ketamine (χ2(1) = 14.087, P < .001). Female participants (N = 138) were more likely to use alcohol only (with no other substances) compared to male participants (N = 71; X2 (4) = 34.182, P < .001). A binary logistic regression considering all substance types upon gender was computed with a forward likelihood ratio variable selection method. Results indicated that those who reported using alcohol were 2.41 times more likely to be female, whereas those who reported using 2C-B, Cannabis, and LSD were 3.75, 3.33 and 2.10 times more likely to be male.
Frequency and quantity of substance use
Self-reported drug use at festivals was compared with use at other times to identify increased or decreased frequency of use during festival periods. Most participants reported an increase in frequency during festivals for each of the five drugs analysed (Table 2). To examine this change, a large, medium and small shift category was produced for each participant based on the difference in frequency between reported outside-festival use to reported in-festival use. For alcohol, the most common shift size was medium (some days to most or every day), whilst for the remaining four substances the most frequent shift size was large (never or occasionally to most or every day).
Shifts in frequency of use between festival contexts and non-festival contexts per substance type.
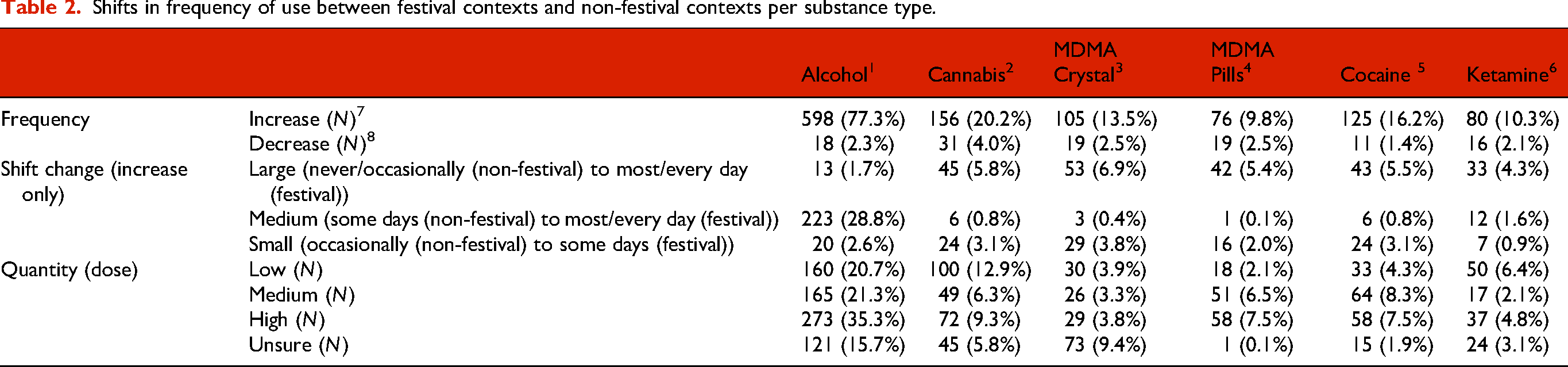
In order to estimate dosage, participants were asked to self-report the average amount of each substance consumed per day during the music festival. Reference values from publicly accessible drug information sources (DrugWise, TripSit, and the NHS: https//www.drugwise.org, https//www.tripsit.me and https//www.nhs.uk) were used to provide guidance for participants. However, it is important to note that a substantial proportion of participants – particularly those using MDMA in crystal form – reported uncertainty about the quantity they had consumed. Among those who used MDMA (N = 286), a quarter (N = 73, 25.52%) of those using the crystal form were unsure of the quantity they had used whilst only one participant using the pill form was unsure of the quantity. This suggests limitations in the reliability of self-reported dose estimates, likely due to the unregulated nature of substances and difficulty in measuring amounts without standard units (e.g. capsules, pills). This limitation is acknowledged in the discussion and reflects the broader challenge of assessing dosage accuracy in retrospective festival drug use research.
Where participants were able to estimate the quantity for a specific substance, between a quarter and a third reported using a high quantity each day at a music festival. For MDMA, the number of participants who reported high quantity use of MDMA pills (N = 58) was almost double that of MDMA crystals (N = 29).
Substance use combinations
Many participants identified as polysubstance users (60.71%) with a much smaller number of participants reporting the use of alcohol and other substances independently of each other (5.62%). A proportion of participants reported using alcohol only (27.12%). While very small numbers of participants reported abstinence from all substance use (3.18%) or using illicit substances while remaining abstinent from alcohol (3.44%). A Kruskal–Wallis H test showed a statistically significant difference in age between the different substance use pattern types, χ2(4) = 45.489, P < .001, with mean rank ages suggesting a significantly older age (or older ages) for alcohol only or abstinence participants, and a younger age (or younger ages) for polysubstance use (Table 3).
The frequency of alcohol only users, illicit substance only users and combined users.

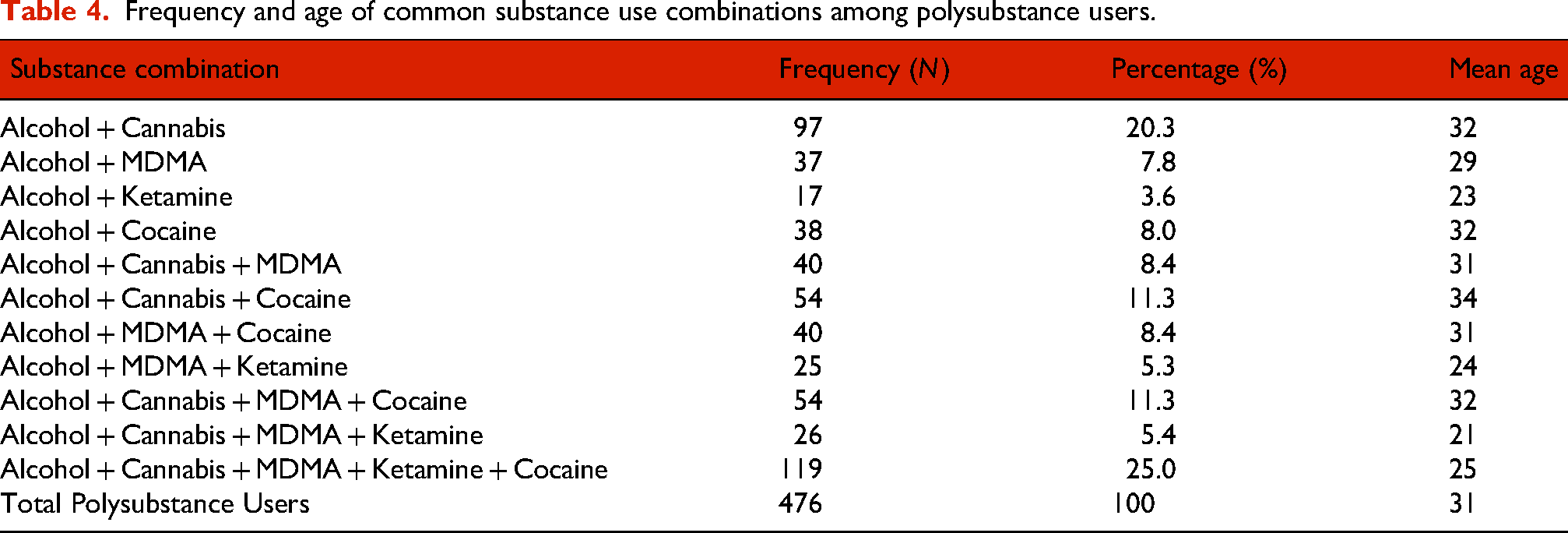
Where participants reported on their polysubstance use, almost all the combinations reported included alcohol as one of the substances (71.6%, N = 341). Further analysis of alcohol use alongside the remaining four most used substances (cannabis, cocaine, MDMA and ketamine) showed a combination of all five substances (25%, N = 119) to be the most common substance use combination (Table 4), followed by the combined use of cannabis and alcohol only (21.4%, N = 97). When examining age, the combined use of alcohol, cannabis, MDMA and ketamine (5.5%, N = 26) showed the lowest mean age (21 years), followed by the combined use of all five substance types (25 years). The highest mean ages observed were 34 years for the combined use of alcohol, cannabis, and cocaine use (11.3%, N = 54). Descriptive analysis found that any combination which included the use of cocaine attracted an older attendee (M = 30.5 years); conversely, combinations including ketamine had a much lower mean age (23.5 years).
Frequency and age of common substance use combinations among polysubstance users.
As the largest subgroup, the combined use of alcohol, cannabis, MDMA, cocaine and ketamine during music festivals was subject to further analysis to identify factors which may predict this polysubstance use pattern. A correlation analysis showed the following variables to have statistically significant relationships with this pattern of polysubstance use: gender (X2 (1, 636) = −8.41, P = .004), employment (X2 (6, 636) = −28.84, P < .001), relationship status (X2 (4, 636) = −21.07, P < .001), age (rs = −0.26, P < .001), number of reported motivations for substance use (rs = 0.27, P < .001); impulsive substance use (X2 (1, 636) = −15.99, P < .001); number of perceived benefits of substance use (rs = 0.24, P < .001); number of risk behaviours in relation to substance use (rs = 0.27, P > .001); number of harm reduction services accessed (rs = 0.22, P > .001); number of music festivals attended (rs = 0.24, P > .001); higher scores for hedonism value (rs = 0.19, P > .001); higher scores for stimulation value (rs = 0.23, P > .001); and attending alternative (X2 (1, 636) = 13.40, P < .001), electronic(X2 (1, 636) = 86.04, P < .001) or grime (X2 (1, 636) = 43.48, P < .001) genre music festivals.
Entering all these variables into a binary logistic regression (computed using a statistical stepwise forward likelihood ratio approach) identified male gender, higher stimulation value, a higher number of reported motivations surrounding substance use, festival genre (electronic and grime) and lower age as the best fitting model (Table 5). The model was statistically significant (χ2(6) = 143.783, P < .001) and explained 35% (Nagelkerke R2) of the variance in the reported use of this combination of substances, correctly classifying 85.1% of cases. The model suggests that males were 2.44 times more likely to report using this five-substance combination than females, with those who attended electronic or grime genre festivals 4.35 and 2.82 times more likely to use this combination of substances respectively.
Model of predictors for festival attendees who report using a combination of alcohol, cannabis, MDMA, cocaine and ketamine.

Substance use related intentions, effects and risks
Nearly all participants reported being aware of the expected effects and risks of each substance type before using them (Table 6). Proportionally, LSD, novel psychoactive substances (NPS) and Benzodiazepines had the largest proportion of participants who reported a lack of awareness of the possible risks associated with these substances. While most users did intend to use each substance type before attending the event, approximately one in five of those using each substance reported doing so impulsively. This proportion was higher (up to 50%) for those substances where the overall reported use was lower (e.g. mephedrone, benzodiazepines, NPS, amphetamine, psylocibin mushrooms, and LSD).
Awareness of expected effects/associated risks and intentions among participants per substance type.

The number of risk behaviours by substance type (i.e. taking more than a safe dose, redosing before feeling initial effects, buying from an untrusted source, taking a substance found discarded or dropped, feeling pressured into taking more of a substance than planned, and polysubstance use) was generally low (Table 7). Alcohol (mean = 1.27) and 2C-B (mean = 2.44) attracted the highest number of different risk behaviours per participant. Overall, polysubstance use was the most reported risk behaviour, with endorsement rates for each of the other risk behaviours broadly similar across substance types. The exception being alcohol where over two-thirds reported taking more than a safe dose in comparison to approximately 10% for the other substances.
Risk behaviours engaged in per substance type.

aThese variables were not collected within this study due to alcohol being a legal substance sold through official vendors. Alcohol is also consumed over a period of time and cannot be reliably considered as individual doses.
Harm reduction strategies and help seeking behaviour
Only 61.7% of participants (N = 383) stated they were aware of the concept of harm reduction in relation to recreational substance use, although within the whole sample participants endorsed an average of 8.13 harm reduction strategies each in relation to their substance use (SD = 7.89, range = 0–44). ‘Drinking soft drinks or water whilst under the influence’; staying with a group of friends’; ‘buying substances from a trusted source’ and ‘eating regular meals’ were the most commonly reported strategies across the different substance types (Table 8). Some harm reduction strategies received very few endorsements across all substance types, namely ‘writing what you have consumed on your hand or mobile phone in case of an emergency’, ‘testing/checking your substance’, and ‘carrying a form of contraception/protection that is, condoms’.
Reported use of named harm reduction strategies among UK festival attendees by substance type used.

Few participants reported having ever accessed specific harm reduction services (Table 9). Results showed that online sources (pill reports / trip reports (N = 127, 16.4%); online substance information (N = 92, 11.9%)) and onsite services (welfare services (N = 82, 10.6%; medical services (N = 57, 7.4%)) were the most popular provision types. DIY reagent testing (N = 57, 7.4%) and substance use information leaflets (N = 52, 6.7%) were also more commonly used than the other provision types named within the survey.
Number of participants who engaged with harm reduction services by type.

The number of people who reported accessing emergency onsite services as the result of the use of a specific substance was very small. For most substances this was less than 1% with the exception of alcohol and MDMA crystals at approximately 2%. It appeared that there was a difference in the rate of access to emergency services between MDMA crystals (1.92%) and MDMA pills (0.78%).
Discussion
This study provides a detailed picture of self-reported substance use, risk behaviours, harm reduction strategies, and help-seeking among UK music festival attendees. Findings suggest age-related differences in substance use, with younger individuals more likely to use NPS or ketamine, while older attendees favour historically popular substances like psilocybin mushrooms or cocaine. These trends align with other reports of increasing NPS use (Mohr et al., 2021; Richeval et al., 2019) and highlight the need for harm reduction strategies to evolve accordingly. Drug checking services and onsite welfare or medical provisions can be informed by the findings reported within this article, adapting to address and mitigate the risks associated with trends in attendee substance use. Numerous festival-specific harm-reduction measures are now in use. Many festivals adopt a ‘welfare-first’ model combining onsite medical tents, chill-out/welfare spaces, and peer support (often called ‘trip-sitting’) for attendees in distress (Janes, 2025). On-site drug checking is increasingly practiced: some countries have front-of-house testing booths, and others run behind-the-scenes testing to detect dangerous substances. Educational outreach (leaflets, apps, on-stage announcements) about safer use is common, and free water, sunscreen, and earplugs are often provided.
Alcohol use, particularly in polysubstance combinations, mirrors international patterns (Fernández-Calderón et al., 2018; Jaensch et al., 2018), reinforcing the need for targeted harm reduction efforts. The widespread pairing of alcohol and cannabis may reflect growing social acceptance of cannabis (McCormack et al., 2021). However, combining multiple substances heightens the risk of harm (Bailey et al., 2019). With most participants engaging in polysubstance use reporting combined use of alcohol cannabis, cocaine, ketamine and MDMA, future interventions should prioritise harm reduction efforts surrounding this increased risk of harm. Participants reporting the use of many substances rarely listed LSD, NPS, or benzodiazepines as primary choices, suggesting moderate use among polysubstance users. Combining MDMA with alcohol markedly amplifies heat and fluid balance problems (van Amsterdam et al., 2021). In one analysis of 1997–2006 deaths, 30% of ecstasy-related fatalities involved MDMA + alcohol vs. 20% MDMA alone (Rogers et al., 2009). Likewise, cocaine used in combination with alcohol produces cocaethylene (a potent cardio-toxic metabolite), stressing the heart. Concurrent use of multiple stimulants (e.g. MDMA + cocaine) can compound cardiovascular and hyperthermia effects, while combining depressants (e.g. alcohol + ketamine) greatly increases sedation and risk of respiratory depression. Even cannabis (though often milder) can impair judgment and add to sedation when mixed with other drugs or alcohol. Festival environments worsen these risks through factors like crowding, heat and dehydration – for example, one NYC EDM festival saw 22 drug-related ER visits (including two deaths) during a very hot weekend with heavy alcohol/drug use (Palamar and Sönmez, 2022). The model reported within this paper which predicted behaviours and traits associated with individuals reporting polysubstance use involving all five substance types is able to inform future intervention design and delivery. For example the model reported indicated these individuals would present with higher scores for hedonism value and higher scores for stimulation value. Understanding that values can impact the type of polysubstance use reported is critical in developing tailored interventions.
Many participants reported increased frequency and quantity of substance use at festivals compared to other contexts. Notably, those using MDMA in crystal form were less able to recall quantity of use compared to those who used pills, suggesting pre-dosed substances may be easier to monitor. However, MDMA pills were used in higher quantities, potentially increasing overdose risk.
Two-thirds of participants recognised the term ‘harm reduction’, and awareness of expected risks and effects of substances was high. This suggests a promising impact of previous education efforts. However further efforts around underutilised harm reduction strategies like drug testing, contraception, and tracking consumption would be beneficial. Risky sexual behaviour has been linked to substance use at festivals (Bows et al., 2024), combined with the reported lack of contraceptive use in this study, suggests stronger messaging on contraception and STD protection should be promoted.
Low engagement with onsite services may suggest either a lack of need or reluctance to seek help. Other UK festival research reports higher medical service use (13%; Bennett and Cottrell, 2024), implying possible underreporting in this study. This may be due to the framing of survey questions around substance-related service use. Further research around prevalence is needed, alongside improved service promotion and integration with online resources. Participants in this study showed greater reliance on online trip reports and DIY reagent testing over formal onsite advice, indicating a preference for informal sources. Strengthening the link between online platforms and onsite services could improve harm reduction efforts (Ivers et al., 2021; Measham, 2019).
Limitations
This survey relied on self-reported data, which may be affected by recall and social desirability biases, leading to inaccuracies in substance use and harm reduction reporting. As it focused on past-year festival experiences, memory degradation or selective recall may have influenced responses. In particular, reported quantities of substances used should be interpreted with caution. Many participants were unsure of dosage, especially for non-standardised forms such as MDMA crystals, reflecting broader issues in accurately measuring and recalling drug quantities consumed in festival environments.
While the sample was large, it was predominantly White British and well-educated, limiting generalisability. Non-binary and undisclosed genders were not analysed separately due to small numbers, potentially overlooking differences. Recruitment via online promotion and festival harm reduction services may have introduced selection bias, and the study's focus on substance use may have influenced rates of abstinence reported. Nested and conditional questions led to variable N values, limiting comparability, while small sample sizes for less common substances reduced statistical power. Finally, the cross-sectional design prevents causal conclusions, highlighting the need for longitudinal research.
Conclusion
This study highlights substance uses patterns at UK music festivals and the need for adaptive harm reduction strategies. The generational associations in substance preferences and high rates of polysubstance use require tailored interventions. Expanding onsite services, particularly around alcohol and drug checking, alongside educational outreach and integration of informal and formal harm reduction resources, is essential to improving festival safety and attendee well-being.
Footnotes
Abbreviations
Ethical approval
Approval for this study was obtained from Swansea University (Ref: 2368) with the study design and delivery informed by Ethics Guidelines for Conducting Internet Mediated Research.
Consent to participate
Obtained by participants via a consent form integrated within the online survey.
Authors’ contributions
All authors were involved in the development of the design of the study. CR led the study, collected and analysed the data. JD, CB, and AJ provided overall methodological and content expertise guidance. CR compiled the initial manuscript; all authors contributed edits and have read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Due to the extensive size of the datasets used and/or analysed during the current study additional analysis and future publications are intended. As such the dataset is not currently publicly available. However, in order to manage data access requests from other researchers, the dataset may be obtained from the corresponding author upon reasonable request.