
Abstract
Background
We sought to examine nascent trends surrounding the impacts of police drug seizures in the period after a substantial public policy shift surrounding the personal possession of drugs in British Columbia (BC), Canada. We explored the intersection of drug testing and police opioid seizures in Vancouver, BC.
Methods
Our descriptive analysis draws on internal police drug seizure data and public drug checking data, using simple linear regression and correlates to measure associations between the quantity of police-reported opioid seizures and the percentage of drug samples that contained both fentanyl and benzodiazepines during the first 6 months of BC's decriminalization framework. A one-month lag was applied to drug-checking data to account for the time delay between seizures and their impact on the drug supply.
Results
In the 6 month period between 1 February and 31 July 2023, police recorded 1805 drug seizures, of which ∼42.7% were opioids (n = 771). The drug sample database recorded 9085 drug samples that were tested for fentanyl and/or benzodiazepines. An early potential relationship (p-value = 0.03) was observed between drug samples that tested positive for both benzodiazepines and fentanyl with the raw number of monthly opioid seizures by the Vancouver Police Department.
Conclusions
Our descriptive analysis shows a potential link between drug samples testing positive for both benzodiazepines and fentanyl, and the quantity of opioid seizures by Vancouver Police Department officers, and highlights considerations of removing police from managing drug use and possession.
Introduction
In the backdrop of an international drug toxicity overdose crisis, and after North America's crisis has worsened over the past decades, some jurisdictions (Arredondo et al., 2018; Davis et al., 2023; Drug Policy Alliance, 2015) have either implemented or are considering significant public policy shifts in relation to the consumption, use, and possession of drugs. The World Health Organization (2023) estimates that 600,000 people died in 2019 from drug overdose across the world, and researchers have estimated that 5.5% of the global adult population uses illegal/criminalized drugs each year, which means the toxic supply has contributed to conditions of a major public health crisis (Das and Horton, 2019). In Canada, more than 47,000 people died from the unregulated drug supply between January 2016 and March 2024 (Public Health Agency of Canada, 2024). British Columbia (BC), Canada's province hit hardest by the crisis, declared a formal public health emergency in April 2016 (Government of BC, 2016). From April 2016 until January 2024, more than 14,000 people lost their lives from drug toxicity (Auditor General of BC, 2024). In the year 2023, the death rate from drug poisonings/overdoses was 45.7 per 100,000 people in the province (Public Safety and Solicitor General, 2024). BC is the jurisdiction relative to other Canadian provinces where fentanyl and fentanyl analog concentration has been the highest during the period of the public health emergency, according to national law enforcement seizure statistics (Kleinman, 2024).
BC implemented a three-year policy pilot on 31 January 2023, under an exemption to the national Controlled Drugs and Substances Act (CDSA) granted by the federal government (Government of BC, 2021). With this exemption, BC became the first province in Canada to shift away from personal possession charges in relation to small amounts of opioids, crack and powder cocaine, methamphetamine, and MDMA (i.e. ecstasy). Under BC's decriminalization framework, people aged 18 and older were able to legally possess a cumulative 2.5 g of these substances combined, while the sharing and/or sale of illegal substances remains a criminal offense (Government of BC, 2021). The exemption did not include other commonly found drugs in BC's unregulated drug supply, such as benzodiazepines despite a marked rise in benzodiazepines in the supply since the onset of COVID-19 (Ali et al., 2023; Gonzalez-Nieto et al., 2025; Russell et al., 2023). Moreover, the production, procurement, selling, exchanging, and retail of these drugs remained unchanged (Government of BC, 2021).
Broadly, decriminalization is not a clearly defined policy framework; rather, there are meaningful differences in policies and options between possible frameworks (Greer et al., 2022; Hughes et al., 2019). The framework adopted can vary widely depending on jurisdiction and policy decisions (e.g. in terms of how personal possession is defined, whether police can seize drugs, alternatives utilized in place of criminal penalties, etc.) and thus, its impact is shaped at the community level (Greer et al., 2022; McAdam et al., 2023). BC's framework in particular is made-up of various legal and policy intersections and comes with significant exemptions. Other published research and commentary have provided in-depth analysis of these limits (Ali et al., 2023; Chin, 2022; McAdam et al., 2023; Speed et al., 2025a, 2025b), and media reports have outlined (Singh Kelsall and Michaud, 2024) how the model's limits may be a hindrance to positive impacts for people who use drugs, particularly in regard to expansion in law enforcement tools and discretion. Relevant concerns include the potential for increased interactions with police due to the continued participation of police within many components of the framework, including being tasked with judging the weight and composition of various drugs by eyesight (Gamage, 2024; Singh Kelsall and Michaud, 2023). Moreover, community reports have raised concerns that police may be seizing drug prescriptions from the public, including during routine displacements of people living outdoors (Mannoe, 2022; Singh Kelsall et al., 2025). This phenomenon has been captured in research from other jurisdictions, such as California (Qi et al., 2022). Notably, however, there have been few published findings and trends regarding these limitations as of this writing. While the BC government has released a minor snapshot of aggregated data (BC Ministry of Mental Health and Addictions, 2024), little other research currently exists on this phenonema (Shaw, 2023; Woo, 2022), and BC police do not proactively permit access to raw data, which restricts analysis of policing behaviors and practices within the decriminalization framework (Singh Kelsall and Michaud, 2024). The federal government did provide funding for independent evaluation of the decriminalization framework; however, the government branch distributing the funds, Health Canada, excluded BC-based researchers from applying altogether (Woo, 2022). As of March 2025, one study using data collected after the implementation of the framework has been published (as well as one pre-implementation), which primarily explores drug user understandings of the decriminalization framework (Ali et al., 2024).
As of March 2025, approximately two-thirds of BC's decriminalization pilot's lifespan had passed. Importantly, multiple levels and branches of government are involved in upholding the framework, during a declared public health emergency (Government of BC, 2021); therefore outcome-based research is urgently needed to inform the continued evolution and/or extension of the pilot. One claim by the government in favor of their chosen framework was that it would shift the type of drug seizures that occur from personal to “trafficking” level (Government of BC, 2021). However, policy research on BC's decriminalization pilot indicates that a cumulative 2.5-gram threshold is an inadequate proxy for delineating possession for personal use from possession for “trafficking” (Ali et al., 2023; McAdam et al., 2023). Research has regularly demonstrated that, in Vancouver and elsewhere, the distinction between “drug trafficker” and “drug user” is nebulous, with the latter often taking on the role of the former (Semple et al., 2011; Small et al., 2013). This is made more complicated by the inconsistent evidence around pre-decriminalization rates of drug seizures. While seizures related to personal possession were purportedly relatively low, historically many people have reported having their drugs seized without arrest or related paper-trail (Hayashi et al., 2023), which creates difficulties in accurately determining pre-and-post decriminalization seizure rates. Furthermore, recent work has demonstrated that the targeting of “traffickers,” a catch-all term for people who work at various levels of the unregulated drug market, disrupts trusted networks of drug purchase and can undermine drug users’ safety (Xavier et al., 2022). Ultimately, drug-related charges also drive incarceration rates in many areas of the world (Mauer, 1995). However, our descriptive exploration focuses narrowly on drug seizures that continue to occur post-implementation of the BC decriminalization framework.
Given the lack of information around drug seizure trends and outcomes post-decriminalization in BC, this article explores preliminary research findings related to ongoing police drug seizures of opioids in the 6 month period immediately following the implementation of the decriminalization framework. Focusing specifically on relationships between opioid drug seizures and subsequent changes in the unregulated drug supply, our descriptive exploration utilizes internal police seizure data, drug checking data, and publicly released fatality statistics and is further informed by our experiential knowledge, as two of the co-authors are frontline outreach-based workers in Vancouver, BC. Importantly, the drug supply has continued to change rapidly in BC while this study was in production (Gonzalez-Nieto et al., 2025), which is to be expected under continued prohibitionist drug policy frameworks (Beletsky and Davis, 2017; Boyd, 2021; United Nations, 2024). Notably, our study examines traceable benzodiazepines in the drug supply. Sedatives, including, but not limited to xylazine (Gonzalez-Nieto et al., 2025) and nitazenes, a benzimidazole-opioid not captured in fentanyl strips (Wallace et al., 2025), became more commonplace in BC's drug supply to varying degrees between 2020 (Tobias et al., 2020) and 2025 (Canadian Community Epidemiology Network, 2023; Gonzalez-Nieto et al., 2025), but are not captured here.
Methods
Data collection
For our statistical analysis, two sets of data were primarily utilized. Opioid seizure data was drawn from the Vancouver Police Department (VPD) internal reporting on drug seizures. While the VPD continued to confiscate many substances that fell under the umbrella of decriminalization, our analysis focuses on opioid seizures because opioids are a clearer driver of an overdose in BC and tend to be routinely identified within the VPD's available drug seizure data (in comparison, other drugs were often labeled in a way i.e. indistinguishable such as “blue substance” or “caffeine”). This internal reporting on drug seizures was obtained by the first author via BC's Freedom of Information and Protection of Privacy Act. Drug testing results were pulled from the BC Centre on Substance Use's (BCCSU) open-access drug testing and sampling data dashboard. BCCSU captures this data via Fourier-transform Infrared Spectroscopy, as well as fentanyl and benzodiazepines test strips (BC Centre on Substance Use, n.d.), located in distributed community-based sites across the city and province. Raw descriptive statistics and sources are presented in Table 1 and Figure 1.
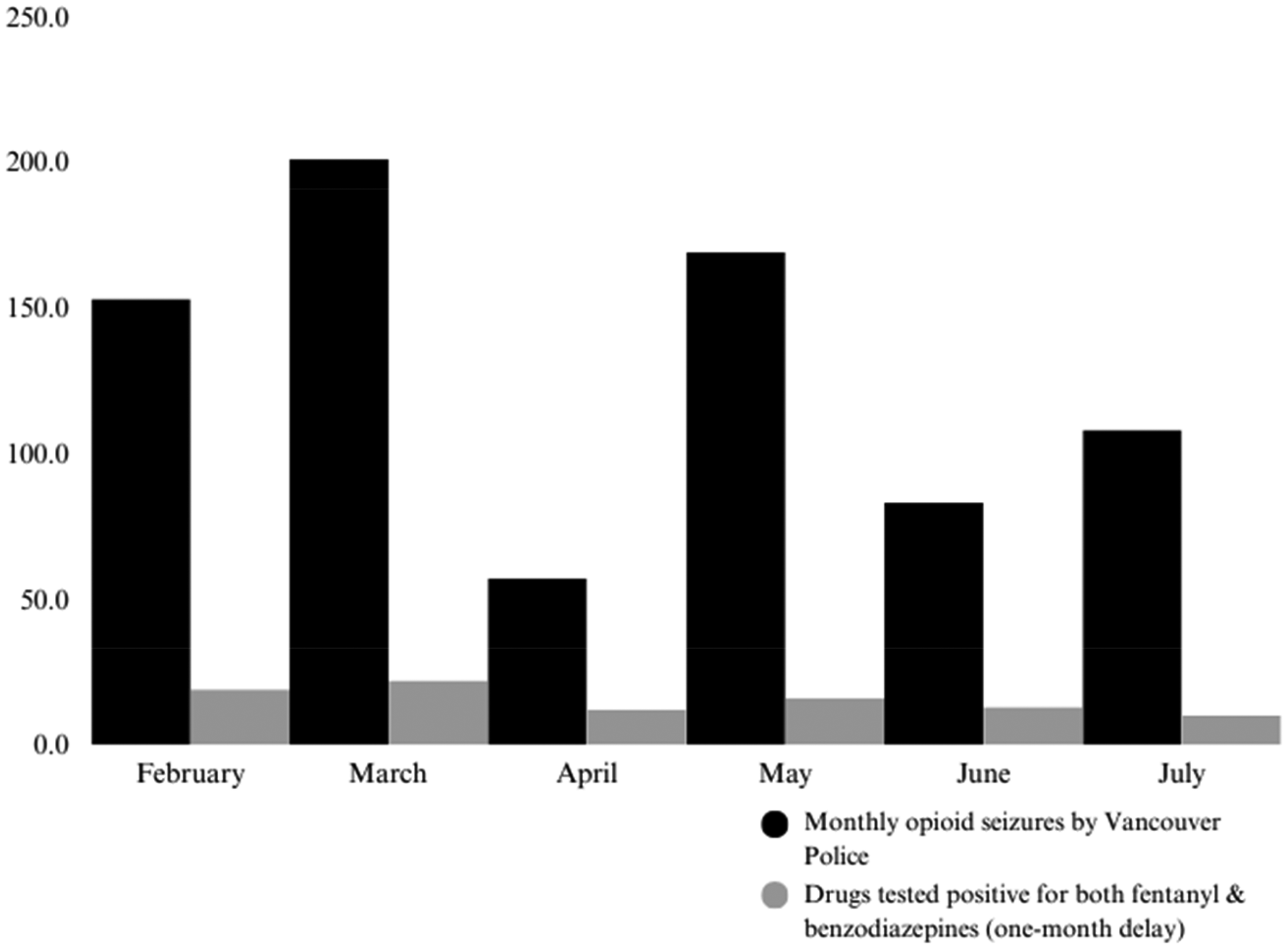
% of drugs with both adulterants and Vancouver Police Department (VPD) opioid seizure monthly totals.
Descriptive statistics.

BC: British Columbia; VPD: Vancouver Police Department; BCCSU: BC Centre on Substance Use's.
Data retrieved via VPD Freedom of Information.
Samples drawn from BCCSU open access dashboard.
Death rates from BC Coroner's Service.
Statistical analysis
VPD drug seizure observations were provided with a monthly breakdown, and individual seizures were categorized by type of drug. To isolate opioids, we included all drugs coded as “fent*,” “heroin*,” “oxy*,” “code*,” “morphine*,” “dila*” (Dilaudid), and “hydro*” (for hydromorphone, the generic title for Dilaudid). As BC's decriminalization model is purported to shift the target of seizures away from the street-level to the mid- and higher-level aspects of the unregulated drug market (BC Ministry of Mental Health and Addictions, 2021; Michaud et al., 2024), we opted not to create a baseline from previous years. This was in part due to the limitation of the VPD data, which does not clearly present when multiple seizures are linked to one event. Instead, we focused on trends within the decriminalization framework to explore the potential impacts of this new direction embedded in the decriminalization model. We noted April 2023 appeared to be an outlier, so we ran the analysis twice. The first time with the raw counts of seizures provided by the VPD. Subsequently, we attempted the same test employing median imputation to further examine the emerging trends. The composition of benzodiazepines and fentanyl adulterants was similarly disaggregated on a monthly basis by the BCCSU. To capture monthly percentages accurately and adjust for variations in the total number of samples submitted, the total number of samples containing both benzodiazepines and fentanyl was divided by the overall number of samples included for each month. The initial drug type being tested is based on self-report, and some monthly totals of the expected drug are lower than what is labeled as a tested opioid, which necessitated the inclusion of all drug samples in this analysis. Furthermore, this reflects that self-reporting can be impacted by social desirability bias, especially considering the stigma around opioid use relative to certain other drugs. For this reason, all drug samples were included. A one-month time-lag was implemented between seizures and sample testing to address the deferred, systemic impacts resulting from the seizures. In the sub-analysis regarding prescription drug seizures, death rates were drawn from the province's coroner's service (BC Coroner Service, n.d.).
Results
In the six-month period between 1 February 2023 (one day after “decrim” was implemented) until 31 July 2023, the VPD documented 1805 drug seizures. Approximately 42.7% of these seizures were categorized as opioids (n = 771). Concurrently, BCCSU recorded 9085 drug samples that were subject to fentanyl and/or benzodiazepine testing. Among these samples, 15% (n = 1374/9085) tested positive for both benzodiazepines and fentanyl. Both the seizure and sample data were disaggregated on a monthly basis. The ratio of positive samples to total monthly samples was calculated to adjust for fluctuations in monthly testing volumes. We employed a linear regression model while applying a one-month lag between seizure and sample to account for the time between seizure and samples being tested. An early significant association (p-value = 0.03, r2 = 0.71) was observed between drug samples that tested positive for both benzodiazepines and fentanyl with the number of monthly opioid seizures by the VPD. The trends are presented in Figure 2. The coefficient's strength was 0.07, indicating that for every opioid seizure, there was a corresponding increase of 0.07% in the proportion of drugs exhibiting multiple adulterants.
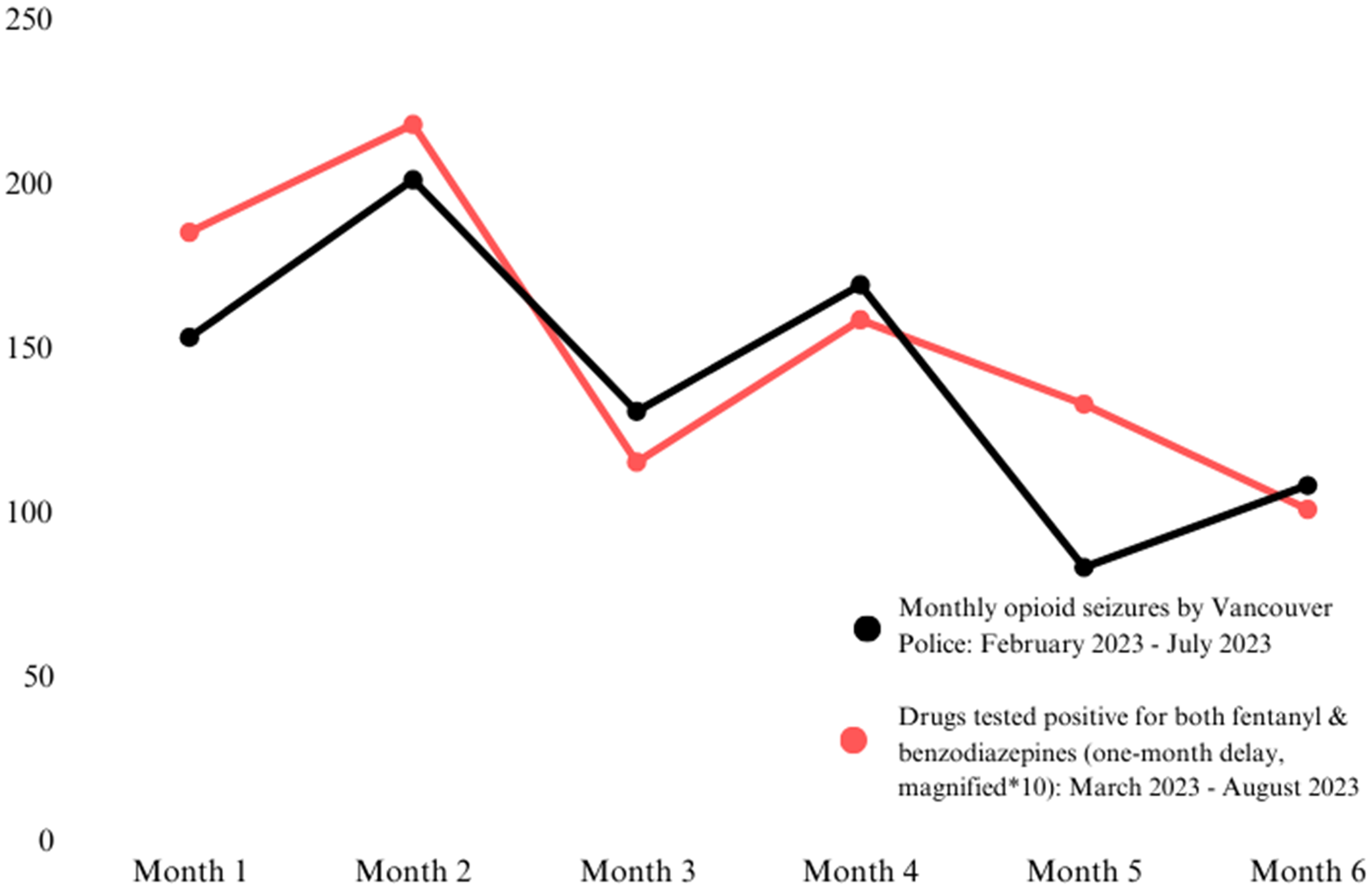
Change to % of drugs with both adulterants and Vancouver Police (VP) opioid seizures.
In a secondary analysis to increase reliability, we employed median imputation as a potential correction in the case that the month of April was an outlier (skewing seizures lower). We replaced the observed opioid seizures with the median seizure amount across the 6 months (n = 130.5). This likewise resulted in a potential relationship between variables (p-value = 0.047, r2 = 0.67). Notably, the coefficient was of a greater magnitude (0.089).
Finally, in a sub-analysis, we explored statistics of drugs seized that police coded as prescriptions in the first 6 months of decriminalization. Our model did not show a relationship between observed prescription seizures and drug supply complexity (p-value = 0.83). However, when applying the same regression and time-lag analysis, we found there was an potential relationship emerging between prescription seizures and drug toxicity deaths in the health region governed by the Vancouver Coastal Health Authority (p-value = 0.047); an area that extends moderately beyond the city boundaries. There was no clear information provided about what defines the category “prescription” (rather than what the police label “illicit”) with the VPD data. This could be a consideration for future research. Figure 3 shows a current link between the two variables.

Vancouver Police Department (VPD) number of prescription seizures and overdose deaths in the Vancouver Coastal Health region (p-value = 0.047).
Discussion
During the 6 months immediately following the implementation of BC's approach to decriminalization, our exploratory analysis demonstrates that opioid seizures remain common practice within Vancouver. Decriminalization is purported to shift the target of seizures away from the street level. If true, and seizures have continued, mid- and higher-level aspects of the unregulated market have been susceptible to police intervention. Our descriptive exploration highlight that law enforcement opioid seizures may lead to further destabilization within the already unpredictable, unregulated drug supply in Vancouver, resulting in more complex compositions, and potential disruptions to drug use routines. This is significant as unintentional benzodiazepine use, when mixed with opioids, can increase the risk of complex overdose and other harms, such as anterograde amnesia (Russell et al., 2023) and/or prolonged sedation, which has been linked to experiences of interpersonal violence (Speed et al., 2025b). This likewise highlights the potential for increases in other forms of criminalization, which can be more severe (such as being charged with possession for the purpose of tracking, rather than personal possession) or more routine (such as bylaw infractions), in the name of “decriminalization,” while these workers in the unregulated drug market are still not the beneficiaries of prohibition. Furthermore, interpersonal trust between sellers and purchasing of unregulated drugs has been measured as a protective factor against opioid overdoses in some regions (Bardwell et al., 2019; Carroll et al., 2020).
Trends in our early and limited descriptive exploration are congruent with recent findings conducted on the impacts of police drug seizures on the composition of the unregulated drug supply, particularly with data collected in the context of the unregulated global drug supply becoming incredibly toxic and unpredictable. One significant example by Ray (2023), linked opioid seizures to both nonfatal and fatal overdoses in Indiana, including with up to 21 days between seizure and overdose event. Other researchers found similar patterns using when employing 2014–2017 data from Ohio (Zibbell et al., 2019). A previous study conducted in Vancouver suggested that from 2009 to 2012, 61% of people who experienced seizures immediately prioritized purchasing replacements (Hayashi et al., 2023). Hayashi et al. (2023) employed data collected prior to the emergence of the unregulated fentanyl supply being mixed with benzodiazepines and other sedatives, and so understanding the acuity of this pattern in this newer and shifting drug supply context should be vital for those trying to improve public health outcomes. The trends presented in our Vancouver study reflect this same temporal order of overdoses following seizures that is present in other studies. Furthermore, a comprehensive scoping review of research on drug seizure and overdose associations in the US from 2013 to 2023 found that 86% of included studies reported at least one significant association between law enforcement seizures and overdose (Cano et al., 2024). Collectively these prior analyses validate what has been theorized broadly as the “Iron Law of Prohibition,” which suggests that by imposing stringent measures (e.g. via increased criminalization and policing) around the unregulated supply chain, the predictability/consistency of prohibited drugs will inevitably decrease (or, conversely, the toxicity of prohibited drugs will inevitably increase) (Beletsky and Davis, 2017).
Our analysis explored a potential mediating variable between police behavior and substance-use-related harms with the extremely limited data available. The increasingly complex drug supply, including the influx of benzodiazepines, in Vancouver and other areas of the world, are linked to individual and community-level harms, such as fatal and nonfatal overdose. The unregulated and unpredictable supply likewise generates other harms, including impacts on wounds (Quijano et al., 2023), potentially risky and physically difficult detox (Hernandez, 2023; Russell et al., 2023; Ti and Tobias, 2021), reduced effectiveness of prescribed alternatives (Silverstein et al., 2019), and gender-based violence (Boyd et al., 2018; Martins, 2022; Speed et al., 2025b; St Denis, 2021; Ti and Tobias, 2021). In Vancouver, overdose response work has also contributed to strain among harm reduction staff (Mamdani et al., 2021; Mental Health Commission of Canada, 2021; Olding et al., 2021), firefighters (Howell, 2023) and the ambulance service (BC Emergency Services, 2024).
Policy and evaluation considerations
These potential emerging trends highlight limitations of BC's decriminalization model as a policy approach and suggest an urgent need to implement interventions that meaningfully address unregulated drug supply to reduce the continuation of fatal and non-fatal overdoses (Death Review Panel, 2023; Irvine et al., 2019). For example, emerging research on increased access to a regulated and predictable drug supply shows substantial impacts on reducing overdoses and other harms (Gagnon et al., 2023; Giang et al., 2023; Gomes et al., 2022; Haines et al., 2023; Ivsins et al., 2020; Slaunwhite et al., 2024), and quality of life factors. This includes an evaluation of a novel “unsanctioned’’ non-medicalized compassion club model in Vancouver, where community members buy illegal/criminalized substances, and test, label, and pack them before they are distributed (Bowles et al., 2024; Kalicum et al., 2024, 2025; Nyx and Kalicum, 2024). In November 2023, the BC government stated it would not consider expanding access to a regulated drug supply outside of the medical system, shortly after the province's Chief Coroner led Death Review Panel (2023) of experts made it their primary recommendation to end the overdose crisis. The potential, emerging trend connecting prescriptions seizures and increased chances of people dying, however, aligns with both the medical logic of safe supply studies, and research showing that access to diverted prescriptions reduces the use of more potent and unpredictable drugs (Bardwell et al., 2021; Death Review Panel, 2023; Kalicum et al., 2024; Kolla and Strike, 2020; Nyx and Kalicum, 2024). The BC government reiterated their rejection as recently as July 2024 when they rejected a similar recommendation by the Office of the Provincial Health Officer (Provincial Health Services Authority, 2024). In the immediate term, the reality that prescribed/regulated drugs are being seized by police officers should preclude the need for further protocol; such as the provision of an on-call prescriber who can replace regulated drugs confiscated by police during a life-and-death emergency. It is doubtful that this seizure of all prescriptions is being taken during street sweeps, as community-based concerns include the speed at which sweeps take place and the difficulty in discerning what is confiscated (Mannoe, 2022: 27).
Limitations
This analysis has several limitations. First, seizure data observed on a daily basis, rather than monthly, would allow for a more granular examination and offer more toward theorizing causality. Second, because of numerous non-standardized measurements (“pills,” “bag,” etc.), our analysis was limited to the number of seizures; further total weights of seizures could provide more insight. Third, our data is limited to police-led reporting, which may not capture all seizures, and to community drug-checking services, which may provide only a minor snapshot of what the composition of the supply is overall (Singh Kelsall and Michaud, 2024). Finally, it should be noted that this policy model is a province-wide initiative (Government of BC, 2021) and this data is only based on one jurisdiction with a city-level police force, which limits the generalizability of this study to other parts of the province.
Conclusion
Our early, descriptive exploration is congruent with previous research findings that suggests collective police opioid seizures, including those primarily targeting fentanyl, are associated with the drug supply becoming more complex. While additives are utilized both for their psychoactive properties, to evade criminalization, and/or sometimes to cheapen production, the unpredictable drug supply is driving fatal and nonfatal overdose, as well as other toxic supply-related and drug market harms. In BC, this is occurring during a formal public health emergency model. If law enforcement practices continue to negatively impact the drug supply in BC under the recently implemented decriminalization model, this suggests a greater and urgent need to remove police from managing the drug supply to reduce the amount of people dying in BC, particularly in the absence of a legal, accessible expansion to the regulated drug supply.
Footnotes
Acknowledgements
Thank you to Liam Michaud for collaborating on previous work with one of the datasets.
Authors’ contributions
TSK, DG, and JM wrote the main manuscript text. TSK acquired and interpreted the data. TSK conceptualized the study design. TSK, DG, and JM conceptualized the discussion and validated, reviewed, and edited the findings and final draft. All authors read and approved the final version.
Availability of data and materials
The VPD dataset can be accessed via Singh Kelsall and Michaud (2024). The BCCSU drug sampling statistics are publicly via ![]() .
.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Not applicable. Not a human or animal study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Tyson Singh Kelsall is currently funded through a Canadian Graduate Scholarship – Doctorate. No other funding is associated with this study.