
Abstract
The prevalence of 3,4-methylenedioxymethamphetamine (MDMA) consumption is relatively high in Aotearoa New Zealand, but MDMA use has not been investigated in detail. We explored consumption behaviours and a range of MDMA-related factors, including motivations, subjective effects, and reflections about personal MDMA use via a cross-sectional survey. A total of 1180 respondents (59.2% female, 15% Māori, aged 18–65, Median = 23.5) partially completed the survey, whilst 915 completed most questions. All included respondents had used MDMA in the past 5 years. Median reported MDMA consumption per session was 151 to 200 mg. The majority (88.9%) reported use in the last year, with house parties being the most common setting of consumption. Fortnightly or more frequent use was reported by 14.1%, and 53% reported 21 or more use occasions. Concomitant use with other drugs was common, and the median number of standard drinks consumed in addition to MDMA was 7 to 9. Enhancement (fun, feeling good) was the primary motivation for consumption, followed by social motivations. Motivations scores for MDMA consumption also differed significantly to motivations for alcohol consumption. Reflections about MDMA use were mainly positive and suggest that many respondents perceived that they had benefitted from their MDMA consumption, although a minority also reported increased memory or concentration problems and paranoia. These findings present a detailed overview of MDMA consumption in Aotearoa and show that most individuals use infrequently and consume within a lower risk dose range. However, some participants reported frequent and high-dose consumption, presenting as targets of harm reduction messaging and education. The concomitant use of MDMA and large amounts of alcohol also presents another avenue for public health messaging and intervention.
Introduction
3,4-Methylenedioxymethamphetamine (MDMA) is an illicit drug often classified as an entactogen, meaning ‘to touch within’. It is relatively distinct in its ability to elicit both stimulant-type effects (e.g. euphoria, alertness and energy), in addition to increased feelings of connection, openness and empathy, whilst lacking many of the typical psychedelic effects of drugs like lysergic acid diethylamide (LSD) or psilocybin (Holland, 2001). MDMA effects result from significant release of monoamines, primarily serotonin, but also dopamine and norepinephrine (de la Torre et al., 2004). Despite recent investigations into the potential of MDMA as an adjunct to PTSD psychotherapy (Mitchell et al., 2023), MDMA has historically been consumed in social settings, with significant links to club, festival, and rave culture that remain to this day, with some indication that MDMA may be becoming more mainstream following changes to production and markets (Mounteney et al., 2018). Global estimates suggest past-year MDMA use sits at 0.4% of the population aged 15 to 64 (United Nations Office of Drugs and Crime, 2022), most commonly consumed in higher income countries and by younger people. Although MDMA can lead to negative subjective experiences (e.g. heightened anxiety), the acute effects generally lead to positive experiences. Increased positive mood, energy, sensory experience, and interpersonal connection have all been found to motivate consumption in prior research (Elsey et al., 2023; Sottile et al., 2023; ter Bogt and Engels, 2005), although consumption motivated by coping or conformity has also been identified (Elsey et al., 2023; Sottile et al., 2023).
Multiple drug harms ranking studies report MDMA's harm to be relatively low (Bonomo et al., 2019; Crossin et al., 2023; Nutt et al., 2010; van Amsterdam et al., 2015). However, MDMA use is not risk free, and negative effects such as dehydration and jaw tightness can occur acutely, in addition to a subacute phase of low mood and fatigue in the days following use, colloquially known as a ‘comedown’. As with other drugs, oral consumption is the route of administration that carries the least risk, whilst nasal administration or injection carry additional risks associated with tissue damage or infection. Positive and adverse effects are also somewhat dose-dependent, with negative effects more likely to occur at higher doses (Brunt et al., 2012). Although rare, death can result following MDMA consumption (Rigg and Sharp, 2018; Roxburgh et al., 2021), and the emergence of high-dose MDMA pills and associated complications following their consumption are of significant concern across the globe (Coroners Court of Victoria, 2023; Couchman et al., 2019). Furthermore, MDMA is often substituted or adulterated with other substances (e.g. cathinones (KnowYourStuffNZ, n.d.; Pascoe et al., 2022)) and thus harm can arise from unintentional consumption. This is of particular concern given the current state of the illicit market which continues to include potent opioids, some of which have also been detected in pressed pills sold as MDMA (NSW Health, 2024). Negative effects may also be exacerbated by concomitant use of other drugs with MDMA. Co-consumption of MDMA with alcohol also increases risk of adverse consequences such as dehydration and hyperthermia (van Amsterdam et al., 2021), whilst intoxication may reduce the ability to engage in harm reduction behaviours such as managing timing and total MDMA intake, or avoiding consumption of unidentified substances. This is particularly relevant in Aotearoa New Zealand (hereafter Aotearoa), where hazardous drinking is common in younger people, including binge drinking (Ministry of Health, 2023).
Investigations of long-term effects of MDMA have historically focused on long-term negative impacts such as deficits in neurocognitive functioning and mental health (Parrott, 2013), although findings are complicated by various limitations and confounding factors, including polydrug use and potential impact of adulterants. As such, the extent of use that leads to neuroadaptive changes that results in impairment, and the clinical relevance of detected impairments remains relatively unclear (Amoroso, 2019; Montgomery and Roberts, 2022). In contrast, very little research has sought to examine what consumers of MDMA think about the long-term positive impacts of use, although that which does exists suggests lasting positive impact on consumers emotional openness and social functioning, and life perspective (Elsey et al., 2023; Hunt and Evans, 2008). Understanding of the potential negative impacts of use are clearly important from a public health perspective, however investigating the perceived benefits of MDMA consumption is also necessary to understand consumption behaviour more broadly. With a more nuanced understanding of both the costs and benefits of consumption, ongoing MDMA harm reduction messaging and education can be better informed.
MDMA is not manufactured within Aotearoa (Wilkins et al., 2018), and therefore is heavily influenced by global drug production and policing changes. These factors in addition to Aotearoa's geographical isolation impact the MDMA market, leading to a relatively high national price (Wilkins et al., 2020). Despite high costs, recent data from the 2022/23 New Zealand Health Survey showed a past-year MDMA prevalence for those aged ≥15 of 3.6%, which peaked at 4.8% in 2020/2021, up from 1.8% in 2018/2019 (Ministry of Health, 2023). Māori (indigenous people of Aotearoa) were approximately twice as likely to have used MDMA in the past year than New Zealand Europeans/Pākehā in 2021/2022, although no difference was detected in the most recent national survey (Ministry of Health, 2023). Consumption also skews towards youth in Aotearoa, with greater past-year prevalence in 15 to 24 (8.1%), and 25 to 34 (8.7%) year olds (Ministry of Health, 2023). Wastewater analysis has also revealed significant fluctuations in MDMA consumption since early 2019 (New Zealand Police, 2020, 2023).
Although prevalence is relatively high, little research has investigated MDMA consumption behaviours in Aotearoa. Given the apparent increase in use, gaining a more in-depth understanding of current MDMA-related behaviours can allow for the identification of higher-risk consumers and present potential focus areas for ongoing harm reduction efforts. In addition, further detail about use can allow for a more nuanced understanding of why people choose to consume MDMA, and how their use may impact their lives. Therefore, our study broadly aimed to explore MDMA use in Aotearoa, including consumption behaviours and practices, prices and acquisition, other drug use, motivations, effects, and reflections about use.
Method
A preregistration relevant to this study is available on the Open Science Framework (https://osf.io/ryu8n/). This study was approved by the University of Otago Ethics Committee (ET21/147).
Recruitment and participants
Recruitment was advertised online within national drug-related groups and via personal profiles of the primary researcher on Facebook, Twitter and Instagram, as well as relevant national and regional Facebook groups and pages (e.g. buy/sell groups), Bluelight, and Reddit. Posters featuring a QR code to the survey were placed in public locations in Ōtepoti/Dunedin and Pōneke/Wellington. Participants were required to be aged ≥18 years, have lived in Aotearoa for 1 year or more, and used MDMA/ecstasy in Aotearoa at least once. Participants could enter a lottery for 1 of 20 $100 vouchers of their choice after completion. Individuals meeting inclusion criteria and enrolled in an undergraduate psychology paper at the University of Otago could complete the survey for course credit instead of the voucher lottery.
Survey design
The survey was presented via Qualtrics (Qualtrics, Provo, USA). Questions were sectioned, such that MDMA and other drug-related blocks of questions and measures appeared first, followed by secondary measures. Differential display logic was utilised to present additional questions when relevant. Pilot testing indicated survey completion would take 30 to 60 minutes. Participants could return to the survey within a month of their last access if not completed. The survey was available between late December 2021 and July 2022. Participants who failed two or more attention checks, reported use of a fake drug, Mingnectin, or did not complete the MDMA use section, were excluded from the analyses.
Variables and analysis
Variables collected included MDMA use behaviours, effects and consequences, other drug history, harm reduction behaviours and other psychological variables. For this article, MDMA consumption behaviours, MDMA price and sources, motivations for MDMA (and alcohol) use, acute effects (when on MDMA or just after the effects subside), after effects (in the 4 days following consumption), and long-term effects and thoughts regarding MDMA are reported (for MDMA harm and harm reduction findings, see Whelan et al., 2024).
Questions about perceived ‘single’ dose, average dose per session, last consumption, frequency, time since stoppage of use, total use occasions, and frequency of use were all measured via ordinal scales (see Results section for detail). Further variable details can be found in the Supplemental material.
Alcohol use disorder was assessed via the Alcohol Use Disorder Identification Test (AUDIT; Barbor et al., 2001) and drug use disorder (excluding alcohol) measured via the Drug Use Disorder Identification Test (DUDIT; Berman et al., 2003). For the AUDIT, a cut-off score of ≥8 is indicative of hazardous drinking, whilst a cut-off score of ≥6 for men and ≥2 for females is indicative of drug-related problems as measured by the DUDIT. The eight-factor substance use motives measure (SUMM) was used to evaluate motivations for the use of MDMA and alcohol (Biolcati and Passini, 2019), where each item was scored on a five-point scale, and a mean calculated for each factor, with a higher score indicating greater endorsement of that factor.
SPSS Statistics (Version 28, IBM) was used for all analyses. Alpha was set at 0.05. Where assumptions of parametric testing were violated, non-parametric equivalents were utilised. Mann-Whitney U tests were used to compare group differences for several measures, and Spearman's rank correlations were calculated for ordinal data (Likert items were not treated as interval data). A Wilcoxon signed-rank test was used to compare motivation scores. Further, as shared method variance artificially inflates correlations to an unknown degree, only correlations of ≥0.3 were interpreted as meaningful. Data analyses were primarily exploratory, although findings related to hypotheses logged in preregistration are reported (see Supplemental material). All analyses between females and males were based on self-reported gender identity. Only respondents who reported use of MDMA in the past 5 years were included in the analyses.
Results
Sample characteristics
Participants completing the main MDMA section of the survey totalled 1180 individuals aged 18 to 65 (M = 25.45, median = 23.5). Females comprised 59.2% of the sample, the remainder consisting of 38.6% males and 2.2% non-binary, gender fluid or gender non-conforming. Most participants were ethnically NZ European/Pākehā (88.2%), whilst 15% identified as Māori and 2.3% as Pasifika (see Supplemental Table S1 for more detail). University of Otago research participants accounted for 19.2% (n = 226) of the sample. Due to participant drop off at different sections of the survey the lowest number of participants included in the analyses presented, excluding follow-up questions, is 915 (except when reporting use of MDMA to treat mental health).
MDMA use
Median age of first MDMA consumption was 19 years. Past-year MDMA consumption was reported by 88.9% of the sample, 96.8% when including use in the past 2 years. The median frequency of MDMA use was every 2 to 3 months, which was reported by 28.5% of participants. Frequency of MDMA use was significantly higher for males than females, U = 147765.5, z = 2.08, p = 0.037. Consumption once a year or less was reported by 14.9% of the sample, and fortnightly or more frequent use was reported by 14.1% (Figure 1).

Frequency of MDMA consumption (n = 1180). MDMA: 3,4-methylenedioxymethamphetamine.
Lifetime consumption of MDMA powder/crystal alone was reported by 87.3% of the sample, while 82.9% had consumed MDMA powder/crystal in a capsule or paper, and 60.3% had consumed an MDMA pill/tablet. The most consumed form of MDMA was powder/crystal alone (54.6%), followed by powder/crystal in a capsule or paper (36.9%) and pills/tablets (8.1%). The most common route of administration was oral (swallowing; 48.4%), followed by nasal (44.7%) and sublingual/buccal (finger dipping/gumming; 6.2%). Most males reported oral consumption as their most common route of administration (53.4%) followed by nasal (41.3%) and sublingual/buccal (4.6%), whilst females primarily reported nasal use (47.4%), followed by oral (44.8%) and sublingual/buccal (7.3%).
The average dose of a typical MDMA pill consumed was most commonly reported as 100 to 150 mg (45.7%), with 30.9% reported doses of 100 mg or less, and 23.4% reported doses of greater than 150 mg. Most participants reported consuming pills all at once (44.3%), followed by halves (28.4%), crushing and snorting the pill (16.1%), consuming in quarters (7.3%), or other (3.9%). For participants who reported pill doses of greater than 150 mg, 42.3% reported consuming all at once, followed by halves (38.7%), crushing and snorting the pill (10.8%), consuming in quarters (4.5%), or other (3.6%).
When participants were asked to report what amount of MDMA they considered a single dose, 18.2% selected ‘I don’t know’. The most selected option was 100 mg (37.6%), whilst 21.5% selected options below 100 mg, and 4.7% selected options including 200 mg or above (Figure 2). Figure 3 highlights the average dose of MDMA consumption per session, which had a median 151 to 200 mg. Average consumption per session was unknown for 15.6% of the sample. The median for males-only remained the same but fell to 126 to 150 mg for females-only, and this difference was significant (U = 95347, z = 4.81, p < 0.001). Different distribution patterns were also apparent when comparing median dose per session for oral (101–125 mg) and nasal (126–15 mg) routes of administration (Figure 3; U = 92578, z = 3.45, p < 0.001).

Amount of MDMA considered to be a single dose (n = 1180). MDMA: 3,4-methylenedioxymethamphetamine.
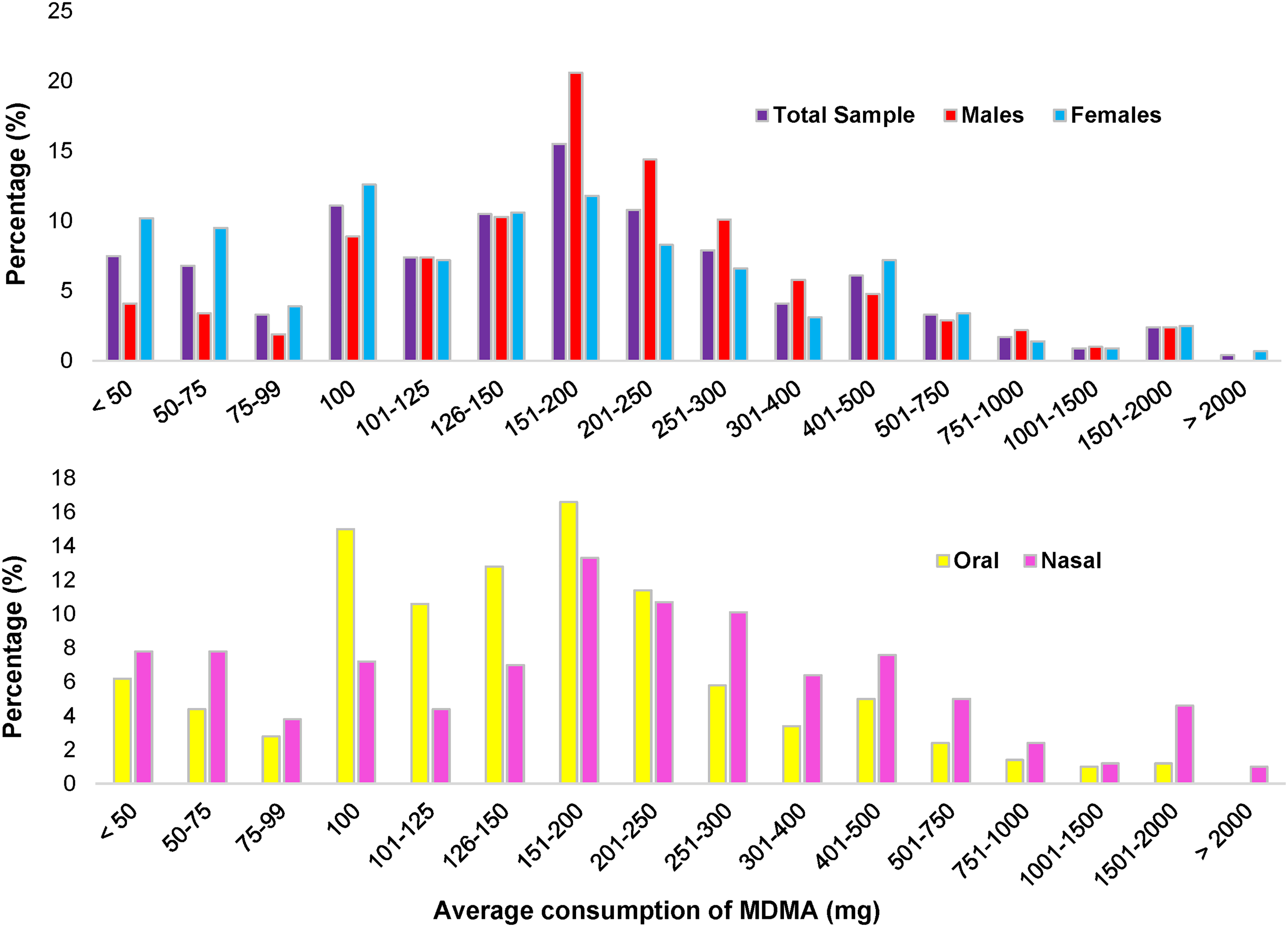
Average consumption of MDMA per session by gender and route of administration. Note. Sample sizes differ between figures. Total sample, n = 997; males, n = 417; females, n = 557; oral, n = 500; nasal, n = 503. MDMA: 3,4-methylenedioxymethamphetamine.
The median lifetime number of MDMA use occasions was 21 to 30, 32.5% had used on 10 or less occasions (4.8% one occasion), and 25.9% reported more than 50 occasions. The maximum dose consumed within 1 hour (reported by 81.9%), did not exceed 50 mg in 9.4%, but exceeded 500 mg in 5.0% of the sample. Almost a fifth of the sample (18.1%) was unable to comment on their maximum dose. Average MDMA consumption per session was negatively correlated with use frequency (lower values indicating greater frequency), r = −0.381, p < 0.001.
Lifetime use of MDMA when also taking antidepressant medication was reported by 21.9% (n = 258). Further details, along with MDMA re-dosing (Figure S1), price (Figure S2), source (Table S2), and physical and social context of use (Table S3) can be found in the Supplemental material.
Alcohol use
Lifetime alcohol use was reported by 98.4% of the sample, 92.5% also reported past 3-month use. The mean number of standard drinks (Aotearoa) in the largest drinking session in the past month was 10.92 (n = 915, SD = 7.71). Lifetime co-use of MDMA and alcohol was reported by 90.1% of the sample. When using both drugs in the same session, the median number of standard drinks was 7 to 9, with 43.9% consuming 6 or less, and 31.5% 10 or more. When co-using with MDMA, alcohol consumption was higher in males than females (n = 1043, U = 107825, z = 4.682, p < 0.001). Of those who completed the alcohol subsection of the survey (n = 915), the mean number of standard drinks in the largest drinking session in the past month was 10.9 (SD = 7.71). Mean AUDIT score (n = 885) was 11.22, with 69.6% scoring ≥8, indicating hazardous drinking. Males and females did not differ significantly in AUDIT score (U = 84229, z = 1.020, p = 0.308). See Supplemental material and Table S4 for additional drug use information.
Stoppage of MDMA use
Almost one-fifth of the sample reported ceasing MDMA use (n = 216, 18.3%), with the majority making this decision within the last year (65.7%). The primary reasons were mental health concerns (43.5%), no longer finding it enjoyable (36.6%), and bad past experiences (27.3%; see Supplemental Figure S3). Nonetheless, reporting this decision did not indicate that individuals had outright ‘quit’, as at least 32 (14.8%) reported using MDMA after their decision to stop. A chi-square test of independence showed that females were more likely than males to have made the decision to stop using MDMA, X2 (1, n = 1154) = 20.19, p < 0.001.
Motivations
The SUMM was completed by 1155 participants regarding their MDMA use motivation. The primary factors endorsed were enhancement (M = 4.16, SD = 0.79) and social (M = 3.48, SD = 0.88) (see Table 1). The SUMM was completed again regarding alcohol use motivations by 915 participants, with primary motivations being social (M = 3.99, SD = 0.85), enhancement (M = 3.21, SD = 0.96) and anxiety-coping (M = 2.88, SD = 1.09).
SUMM factor scores for MDMA and alcohol (n = 915).

Note. Means are inclusive only of those participants that completed the SUMM for both MDMA and alcohol.
Bold indicates a significant difference.
MDMA: 3,4-methylenedioxymethamphetamine; SUMM: substance use motives measure.
Wilcoxon sign-ranked tests indicated a significant difference between MDMA and alcohol motivation scores across all factors, with significantly greater MDMA scores for enhancement, self-expansion and performance, and lower MDMA scores for social, conformity, anxiety-coping, depression-coping, and boredom-coping motivations (see Table 1).
Acute and after effects
A total of 1137 participants responded to items about the frequency of acute MDMA effects (Supplemental Table S5). Typical positive acute effects of MDMA were reported commonly reported as occurring always or most of the time, including greater energy (90.6%), intense positive emotion (87.6%), euphoria (81.6%), greater appreciation of music (86.4%), heightened empathy/social connectedness (80.9%) and heightened appreciation of touch (70.6%). Some negative effects were also commonly reported as occurring most of the time or always, including tight/sore jaw (55.4%), difficulty sleeping (43.8%) and dehydration (39%).
Questions about after effects were answered by 1100 participants. Experience of a ‘come down’ (low mood, increased irritability, etc.) following MDMA use was reported by 83.0% (n = 939). The frequency of reported ‘come down’ experiences occurred sometimes (25.7%), about half the time (30.5%), most of the time (31.2%) or always (12.7%). The time in which the ‘come down’ experience was reported to be experienced the most was the day after (49.9%), followed by 2 days after (34.9%), and the day of use after the MDMA wears off (9.4%).
Experience of an ‘afterglow' (feeling peaceful, happy, etc.) was also reported by 60.9% of the sample (n = 689). This occurred sometimes (41.2%), about half the time (29.2%), most of the time (24.3%), or always (5.3%). The time when the ‘afterglow’ experience was reported to be felt the most was the day after (78.3%), followed by 2 days after (13.9%), and 3 days after (3.4%).
After effects (occurring up to 4 days post-consumption) were reported on by 1100 participants. Both ‘depressed or low mood’ and ‘happiness’ were reported as occurring sometimes or more frequently by over half the sample. ‘Physical tiredness’ (87.1%) and ‘sore jaw’ (70.5%) were also reported as occurring sometimes or more frequently. ‘Brain zaps’ (internal electric shock-like experience), were reported as occurring sometimes or more often by 35.4% (Supplemental Table S6). No correlations between after-effects and average MDMA use per session were stronger than 0.3.
Reflections on MDMA use
Long-term effects and thoughts about MDMA use were reported on by 1039 participants. In general, higher levels of agreement were found for items with positive sentiment, whilst the opposite was true for the negative sentiment items (Table 2). Items that the majority of participants agreed with included ‘I am happy that I tried it’ (91%), ‘gave me amazing memories’ (85.3%), ‘among the most pleasant experiences of my life’ (68.3%), ‘improved my friendships’ (53.0%), ‘deepened my emotional experiences’ (58.1%) and ‘helped me learn to let go and express myself/be more open’ (58.0%). Of note, 19.0% thought their MDMA consumption had contributed to problems with concentration and memory, and 9.8% agreed that it had made them more paranoid. A minority of participants reported that their MDMA consumption blunted their emotional experiences (6.9%), made them more socially anxious in daily life (6.7%), or made them less able to acknowledge and reflect on their emotions (5.7%).
Agreement with items related to long-term effects and thoughts about MDMA (n = 1039).
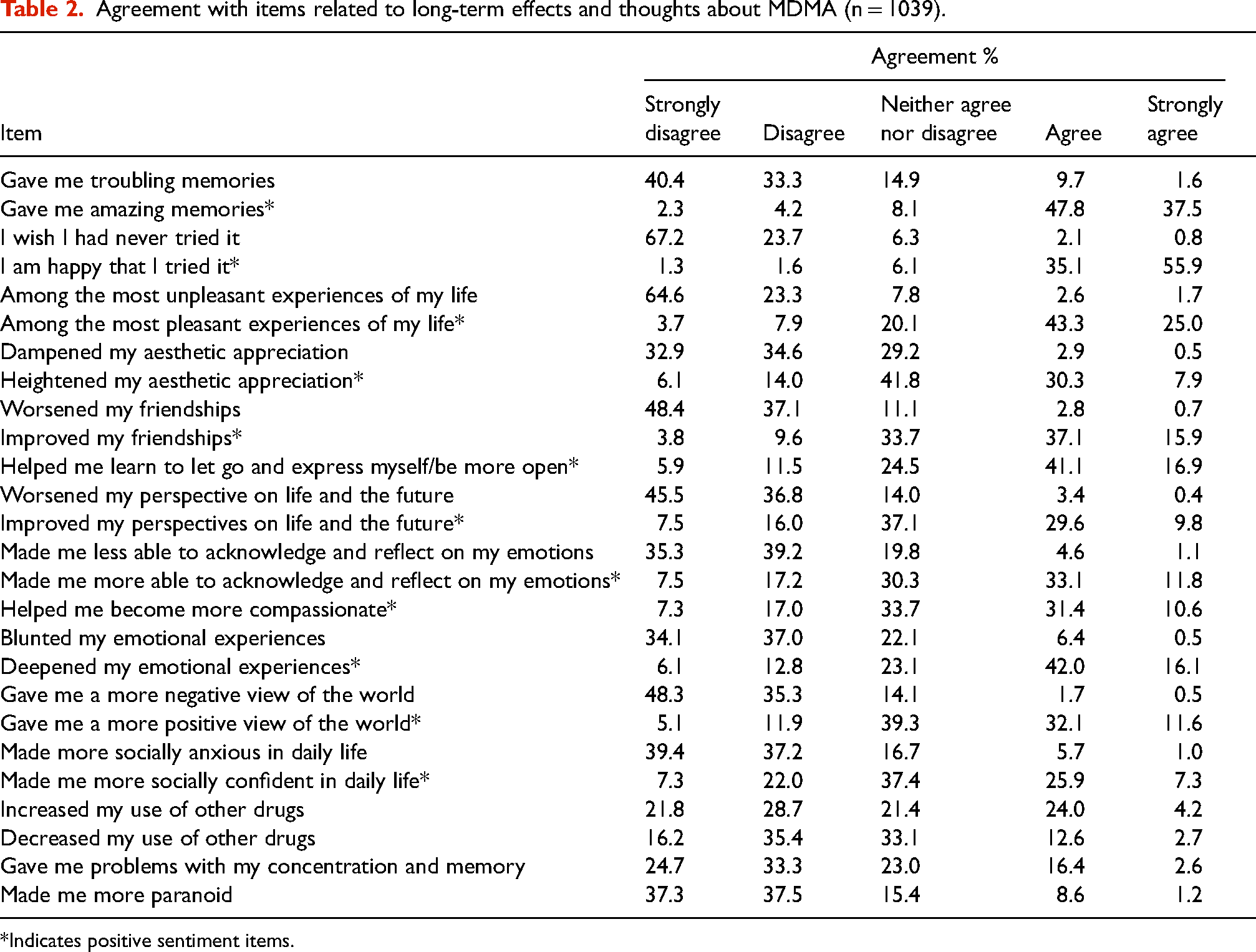
*Indicates positive sentiment items.
Discussion
As with other drugs, consumption behaviours associated with MDMA are known to vary considerably, and our findings confirm those of studies in other locations (Peroutka et al., 1988; Topp et al., 1998). Firstly, per-session consumption varied largely, although the median was similar to the 200 mg described in a recent global survey (Winstock, 2021). Reported frequency of use, and the significant correlation between this and per-session consumption implies that some consumers experience some form of tolerance or adjustment to MDMA effects. Females are overrepresented at the lower end of consumption, which may be related to lower body weight, and consumer adjustment of dose based on this consideration. Although previous data has indicated that Māori adults were more likely to have used MDMA in the past year (Ministry of Health, 2023), our results found no differences between Māori and non-Māori in average amount of MDMA consumed. Given the findings regarding frequent and high dose consumption, future harm reduction efforts aimed at reducing such consumption behaviour may have the highest impact regarding MDMA-associated harms and long-term impacts.
Over a fifth (21.9%) of the sample reported prior consumption of MDMA whilst also taking an antidepressant. The top three antidepressants reported were all selective serotonin reuptake inhibitors (SSRIs), which are known to significantly diminish the subjective and physiological effects of MDMA (Liechti and Vollenweider, 2001), and are dispensed to approximately 9% of adults in Aotearoa (Best Practice Advocacy Centre New Zealand, 2019). Whether a lack of subjective experience changes drive higher levels of consumption, and whether this has led to subsequent harm, is unknown, but clearly highlights a point for future study and public education. It may be the case that individuals who have combined these drugs were unaware of SSRI's MDMA-attenuating effects as physicians do not share illicit drug information at the point of prescription. Prescribers should be careful to share this information with patients, and other relevant drug–drug interactions, whenever possible.
Reported prices of MDMA also generally align with previous Aotearoa research (Wilkins et al., 2019; 2023). Most of the sample reported acquiring their MDMA through friends, indicative of social supply (see van der Sanden et al., 2021), resulting in more distributed purchasing networks as fewer individuals interact with drug dealers themselves, which is likely perceived as less risky. Given the high amount of social supply, promotion of harm reduction via pre-existing friendship networks may provide a useful additional avenue for information sharing that is valued and trusted beyond public health messaging or direct contact with health and drug-related services, positively influencing peer behaviour.
Party environments were reported as common locations for MDMA use, of which house parties were the most common, potentially due to ease of access, greater frequency, reduced fear of legal repercussions and reduced cost of attendance. Unsurprisingly, given the relationship between MDMA and clubbing and festival culture (Mounteney et al., 2018), over half the sample reported use in these settings. The most highly endorsed drugs co-used with MDMA were similar to those reported in the past year (alcohol and cannabis), many of which have long been explored and reported on by consumers (Erowid, 2023). Past 3-month consumption of other ‘party’ drugs such as LSD and ketamine was also relatively high amongst the sample, including in combination with MDMA. Although studies in other countries have found that illicit/prescription depressants are often used to alleviate stimulation and aid sleep as MDMA effects subside (Allott and Redman, 2006; Panagopoulos and Ricciardelli, 2005), these drugs were not commonly reported as consumed in the same session as MDMA. This is likely due to Aotearoa's unique drug landscape and relative unavailability of these drugs (e.g. benzodiazepines), where alcohol, cannabis, or ketamine may instead be used in this way.
Aotearoa has significant levels of hazardous drinking, particularly among younger people (Ministry of Health, 2023). Therefore, it is unsurprising that the largest past month drinking session was above 10 standard drinks, and that the mean score on the AUDIT is indicative of hazardous drinking behaviour. Moreover, the median number of standard drinks consumed when combined with MDMA was higher than a common cut off for a binge session (≥5; Ball et al., 2020). With concomitant use of alcohol with MDMA potentially increasing the risk of hyperthermia and dehydration (van Amsterdam et al., 2021), reduction of alcohol consumption when consuming MDMA is a clear target for harm reduction education and intervention efforts in the future. Additionally, large portions of the sample also scored above cut-off thresholds as measured by the DUDIT, which is suggestive of potential drug use problems in this sample. However, this should be interpreted with caution as no research has validated or utilised the DUDIT in a sample of people who use drugs in Aotearoa.
As negative after effects are commonly described following MDMA use, it is not unexpected that the main reason for stopping MDMA use reported by our sample was mental health concerns, aligning with previous research on the issue of quitting (Verheyden et al., 2003). Other reasons such as no longer finding MDMA enjoyable may indicate tolerance (potentially chronic tolerance; Parrott, 2005), whilst a bad experience with MDMA may also result from mistakenly consuming other drugs. We were unable to ascertain whether this stoppage equates to what one might normally consider ‘quitting’ the substance, or some other decision to cease use for a specific amount of time. Notwithstanding the limits of interpretation, these findings provide interesting insights into the reasoning for stopping consumption and highlights individual willingness to cease use for health preservation.
The primary motivations for MDMA use reported here were enhancement, social, and self-expansion, which are all similar to previous findings, where people discuss feeling good, having fun, interpersonal connection, and altered experience (Sottile et al., 2023; ter Bogt and Engels, 2005). Motivation scores across all factors significantly differed between MDMA and alcohol, and although social motivations for alcohol were higher, alcohol scored higher for the negatively framed motivations of conformity and coping. Previous research has shown that conformity and different types of coping are typical motives for alcohol consumption (Cooper, 1994), whilst more recent research has captured coping as a motivation for MDMA consumption (Sottile et al., 2023). In general, it is encouraging to see that coping motivations appear to be less important for MDMA consumption than alcohol, although this further highlights issues related to consumption of alcohol. It should be noted that the SUMM has not been previously used to assess motivations of people who use MDMA, nor within Aotearoa, therefore, our findings relating to motivations should be interpreted with caution.
Typical acute effects of MDMA were reported as frequent during intoxication, while negative acute effects that may indicate significant and potentially hazardous levels of intoxication (e.g. confused thoughts, difficulty standing or moving) were reported as infrequent. Characteristic after effects such as depressed mood, physical tiredness and sore jaw were commonly reported, replicating previous findings of the often reported come down experience (Curran and Travill, 1997; Kelly, 2009; Topp et al., 1997). Self-report of a ‘come down’ experience was common, although the frequency of such experiences differed considerably within the sample, while 27% of the sample did not report this. Experience of an ‘afterglow’ effect, which is commonly associated with psychedelics (Evens et al., 2023), but also MDMA (Freye, 2009), was also reported by most of the sample. Although no direct comparisons were made to psychedelic effects, this may indicate that a similar serotonergic mechanism underlies the afterglow experience following consumption of these drugs. Collectively, the frequency of come down and afterglow experiences implicates other variables in the production, or interpretation, of states following MDMA consumption, and signals the need for further research into how drug, set and setting factors contribute to these after effects. ‘Brain zaps’, a poorly characterised electrical shock type experience often associated with discontinuation of SSRIs (Papp and Onton, 2022), were also somewhat common, and potentially indicative of heavy/frequent use resulting in changes to serotonin or norepinephrine regulation in the brain (Papp and Onton, 2018), emphasising the need to explore this phenomenon in future work.
Like the findings of Elsey et al. (2023), participants’ thoughts regarding MDMA use and long-term effects were primarily positive, with positive sentiment items receiving high levels of agreement relative to comparison negative sentiment items. The findings related to social and emotional benefits are of significant interest, as previous work that has shown MDMA can increase prosocial behaviour (Bershad et al., 2016; Hysek et al., 2014) and empathy (Carlyle et al., 2019). It seems to be the case that similar changes have occurred for many of the participants in this study, who have experienced their use of MDMA as particularly positive overall. Given the primarily positive reflections about MDMA, future harm reduction messaging would likely benefit from acknowledgement of the benefits of MDMA consumption generally, and how harm reduction behaviour may not only reduce harms, but increase pleasure associated with use (Global Drug Survey, 2014), serving both public health and consumer goals. Importantly, our results also highlight potential negative impacts of MDMA consumption, of which increased paranoia and impaired concentration and memory are of concern. Attention and memory issues have been reported in the literature (Gouzoulis-Mayfrank et al., 2000; Laws and Kokkalis, 2007), as has paranoia (McGuire and Fahy, 1991; Schifano and Magni, 1994), and these concerns highlight an area for ongoing attention within MDMA consuming populations. Just over 5% also reported being more socially anxious in daily life and having blunted or lesser ability to acknowledge and reflect on emotions. A large proportion of people who decided to stop MDMA use cited mental health concerns, which likely reflects the impact that particular MDMA use behaviours can have on the mental health of some people. Ultimately, the bidirectional impact that MDMA can have on mental health and wellbeing highlights the importance of being mindful about consumption and carrying out harm reduction behaviour whenever possible. To increase awareness of these risks and reduce the burden of overall harm, harm reduction-based drug education programmes should be developed and implemented at a national level.
Limitations
As this research design incorporated a survey, the findings come from a convenience sample, which increases the risks of selection bias and limits generalisability. Although there is evidence of negative thoughts regarding MDMA experiences within the data, participation in the survey may have been more attractive to people who felt positively about their MDMA experiences. However, the online survey likely facilitated more honest participant responses than face-to-face research due to increased confidentiality (Miller and Sønderlund, 2010). The age distribution of our sample is impacted by the portion of undergraduate psychology students included in the sample, however, this is not likely to impact the findings dramatically, given that MDMA consumption is more common in younger populations (Ministry of Health, 2023; United Nations Office of Drugs and Crime, 2018). Although this research includes a significant portion of people who have ceased MDMA use, all participants had consumed within the past 5 years, and thus may more prone to reflect upon the impacts of MDMA more positively than those who have people who have been abstinent from MDMA for a longer time period.
Conclusion
This article provides a general overview of MDMA consumption behaviour and associated factors within Aotearoa, with findings highlighting that MDMA consumption behaviours and experiences are relatively wide ranging, but most individuals are using MDMA relatively infrequently and at doses which are less likely to result in harm. Furthermore, perceptions of long-term effects and thoughts related to MDMA consumption are primarily positive, and MDMA use motivations are primarily associated with enhancement and socialising. Ongoing harm reduction efforts may benefit from addressing the consumption of large quantities of alcohol in addition to MDMA, whilst those who exhibit frequent or high-dose consumption of MDMA present as specific targets for harm reduction intervention and future investigation. Although the presented findings are relatively detailed, continued monitoring of MDMA use (and other drugs) and/or the refinement of a national monitoring system could allow for analysis of trends that may benefit people who use drugs and health professionals, whilst allowing for comparison between countries that can facilitate global harm reduction initiatives and greater understanding of the population of people who use MDMA.
Supplemental Material
sj-docx-1-dsp-10.1177_20503245241274170 - Supplemental material for 3,4-Methylenedioxymethamphetamine (MDMA) consumption in Aotearoa New Zealand: A quantitative survey exploration
Supplemental material, sj-docx-1-dsp-10.1177_20503245241274170 for 3,4-Methylenedioxymethamphetamine (MDMA) consumption in Aotearoa New Zealand: A quantitative survey exploration by Jai Whelan, Geoff Noller and Ryan D Ward in Drug Science, Policy and Law
Footnotes
Acknowledgements
JW thanks the University of Otago for support via a doctoral scholarship.
Authors’ contribution
JW contributed to conceptualisation, methodology, formal analysis, writing – original draft preparation, and writing – review & editing. GN and RW were involved in supervision and writing – review & editing.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: All resources and funding required for this research was provided by the University of Otago.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.