
Abstract
Background
Various detoxification regimens are used for gamma-hydroxybutyrate (GHB) and gamma-butyrolactone (GBL), including diazepam, barbiturates, baclofen and GHB itself. However, these regimens are primarily derived from inpatient units, and literature on outpatient GBL detoxification is sparse with no previous reports on chlordiazepoxide. We describe the characteristics of outpatient GBL detoxification using chlordiazepoxide.
Methods
Observational study of all patients who attended a community outpatient addiction service in South London between August 2015 and November 2017 seeking detoxification from GBL. The outpatient caseload is predominantly patients with alcohol, opioid and stimulant dependence. Routine clinical data including patient demographics, GBL usage, daily chlordiazepoxide dose and Clinical Institute Withdrawal Assessment for Alcohol-revised (CIWA-Ar) score were recorded.
Results
In the study period there were 17 attendances for GBL detoxification, 14 of which were undertaken in the outpatient setting. Twelve (86%) patients who had an outpatient detoxification were male, all of whom were men who have sex with men. Of 14 outpatient GBL detoxifications managed with chlordiazepoxide, 10 were successfully completed. One of the four patients that did not complete detoxification required inpatient treatment in an acute hospital. The average successful detoxification took 10 ± 3.1 days. For patients who completed a detoxification, the median maximum CIWA-Ar score on day one of the detoxification was 11 (range 2–17), with the mean dose of chlordiazepoxide used on day one being 140 mg (range 80–225 mg).
Conclusions
Chlordiazepoxide can be used for outpatient GBL detoxification in combination with a provision for crisis admission to hospital. CIWA-Ar score can be applied to GBL withdrawal to measure severity and inform a reducing regimen of chlordiazepoxide.
Introduction
Gamma-hydroxybutyrate (GHB) and its precursor gamma-butyrolactone (GBL) are dependence forming drugs that exert their pharmacological effects through the gamma-aminobutyric acid system (Kamal et al., 2017). Presentations to addiction services for treatment of dependence on GHB/GBL (subsequently referred to as GBL alone) are rare in England making up 0.2% of those in National Health Service (NHS) treatment for alcohol and drug dependence in 2016/2017 (Knight et al., 2017). Previous literature has demonstrated successful detoxification from GBL in inpatient or specialist outpatient clinics using diazepam or pharmaceutical GHB (Bell and Collins, 2011; Kamal et al., 2017). Baclofen and barbiturates have been used as an adjunct to benzodiazepines in refractory withdrawal (Kamal et al., 2017).
Most areas of England lack specialist community GBL clinics and inpatient beds for planned detoxification (Kalk et al., 2018). Furthermore, many patients are reluctant to undergo inpatient detoxification (Bell and Collins, 2011). Although GBL presentations to outpatient addiction services are relatively rare, the lack of inpatient detoxification beds in much of England, combined with patient preference for outpatient treatment, mean that services will intermittently be presented with cases for which outpatient detoxification must be considered. In this paper, we describe outpatient detoxification from GBL, in a community addiction service primarily treating alcohol, opioid and stimulant dependence, using protocols developed from the literature and local alcohol detoxification pathway.
Methods
Participants
This observational study includes all patients who presented to a South London community addition service with GBL dependence seeking abstinence through detoxification between August 2015 and November 2017.
Clinical management
Patients were assessed by a doctor and offered inpatient detoxification. If patients declined inpatient detoxification, they were assessed for outpatient detoxification based on the criteria below.
Outpatient detoxification eligibility criteria:
GBL dependence; reports or demonstrates withdrawal symptoms and can evidence GBL use (e.g. empty containers) Have 24 h support throughout the detoxification by a non-drug- or alcohol-dependent adult Be able and willing to attend daily appointments for the duration of the detoxification (excluding weekends) Have sought outpatient detoxification Have no contraindications to community detoxification (below) Prior serious withdrawal symptoms in treated GBL withdrawal, including seizures and delirium Previous repeated failed outpatient detoxifications Significant unmanaged physical comorbidities (such as decompensated liver disease or an exacerbation of chronic obstructive pulmonary disease) Significant poorly controlled mental ill health Social isolation; lack of a supportive non-drug- or alcohol-dependent adult to monitor the detoxification Using ≥30 mL GBL per day (based on clinical experience that this level of GBL use carries a higher risk of severe withdrawals that are more difficult to control with benzodiazepines)
Outpatient detoxification contraindications:
Ethics
This audit of GBL detoxification treatment was approved by the South London and Maudsley addictions clinical governance committee.
Detoxification regimen
Prior to commencing the detoxification, patients were given information on the detoxification procedure. To allow five consecutive days of observation prior to the weekend, detoxifications began on a Monday except in exceptional circumstances.
Patients were prescribed a variable dose of chlordiazepoxide based on a symptom triggered protocol as measured by the Clinical Institute Withdrawal Assessment for Alcohol-revised (CIWA-Ar) score (Sullivan et al., 1989). The CIWA-Ar score comprises ten symptoms (nausea and vomiting, tremor, paroxysmal sweats, anxiety, agitation, tactile disturbances, auditory disturbances, visual disturbances, headache and orientation) each scored out of seven, excluding orientation which is scored out of four, giving a total score out of 67. A typical interpretation of the score, as applied to alcohol withdrawal, is that ≤9 is minimal withdrawal, 10–19 is mild to moderate withdrawal and ≥20 severe withdrawal.
Starting doses were determined by the initial CIWA-Ar score, level of GBL use and clinical judgement. Staff were familiar with the use of CIWA-Ar in alcohol withdrawal. On day one of the detoxification, patients were asked to stop using GBL 1–1.5 h before attending and were seen at least twice to ensure symptomatic control without over-sedation. Patients were subsequently seen daily, excluding weekends. On these visits, any arising issues were discussed, observations and CIWA-Ar score were recorded and chlordiazepoxide dose was determined. Chlordiazepoxide was titrated based on withdrawal severity and dispensed to the patient to self-administer as advised over the next 24 h with the support of their accompanying adult. Patients were initiated on four regular doses of chlordiazepoxide across 24 h and given an additional supply of ‘as required’ chlordiazepoxide to be taken if the patient felt their symptoms were not being adequately controlled. Chlordiazepoxide was weaned down and stopped at the conclusion of the detoxification. No other pharmacological treatment was used during or after the detoxification.
Patients and their carers were advised how to seek crisis support outside of clinic hours. This involved a large local acute hospital where the community addictions service had close links to the hospital addiction care team.
Alongside the detoxification, patients were offered blood-borne virus (BBV) screening and psychosocial support, including harm minimisation advise, key work and group sessions. If appropriate, patients were offered a sexual health appointment with an in-house specialist.
Data
As part of routine clinical practice, the following data were collected on all patients: demographics, employment status, BBV status, sexual orientation, daily GBL use (mL), length of detoxification, daily dose of chlordiazepoxide used, CIWA-Ar score, heart rate, blood pressure, use of other recreational drugs and detoxification outcomes. On days with multiple clinical contacts (e.g. day one of the detoxification), the highest CIWA-Ar score was used.
Results
Patients and treatment
Between August 2015 and November 2017, there were a total of 17 attendances to the specialist addictions clinic for GBL detoxification by 14 individuals (Figure 1). Three patients requested an inpatient detoxification and are not included in this report. A total of 14 outpatient detoxifications were undertaken by 11 individual patients. Of these 11 patients, three relapsed following completion of the detoxification, and subsequently presented with GBL dependence a second time during the study period giving a total of 14 detoxifications from 11 individuals.

Flowchart of patient attendances for gamma-butyrolactone (GBL) detoxification and outcomes in the study period.
The baseline characteristics of patients that underwent outpatient detoxification are shown in Table 1. All male patients (n = 10) were men who have sex with men, of whom three were HIV positive (27%), and one had hepatitis C (9%).
Demographic characteristics of all detoxifications (including three repeat detoxifications) and first detoxification only.
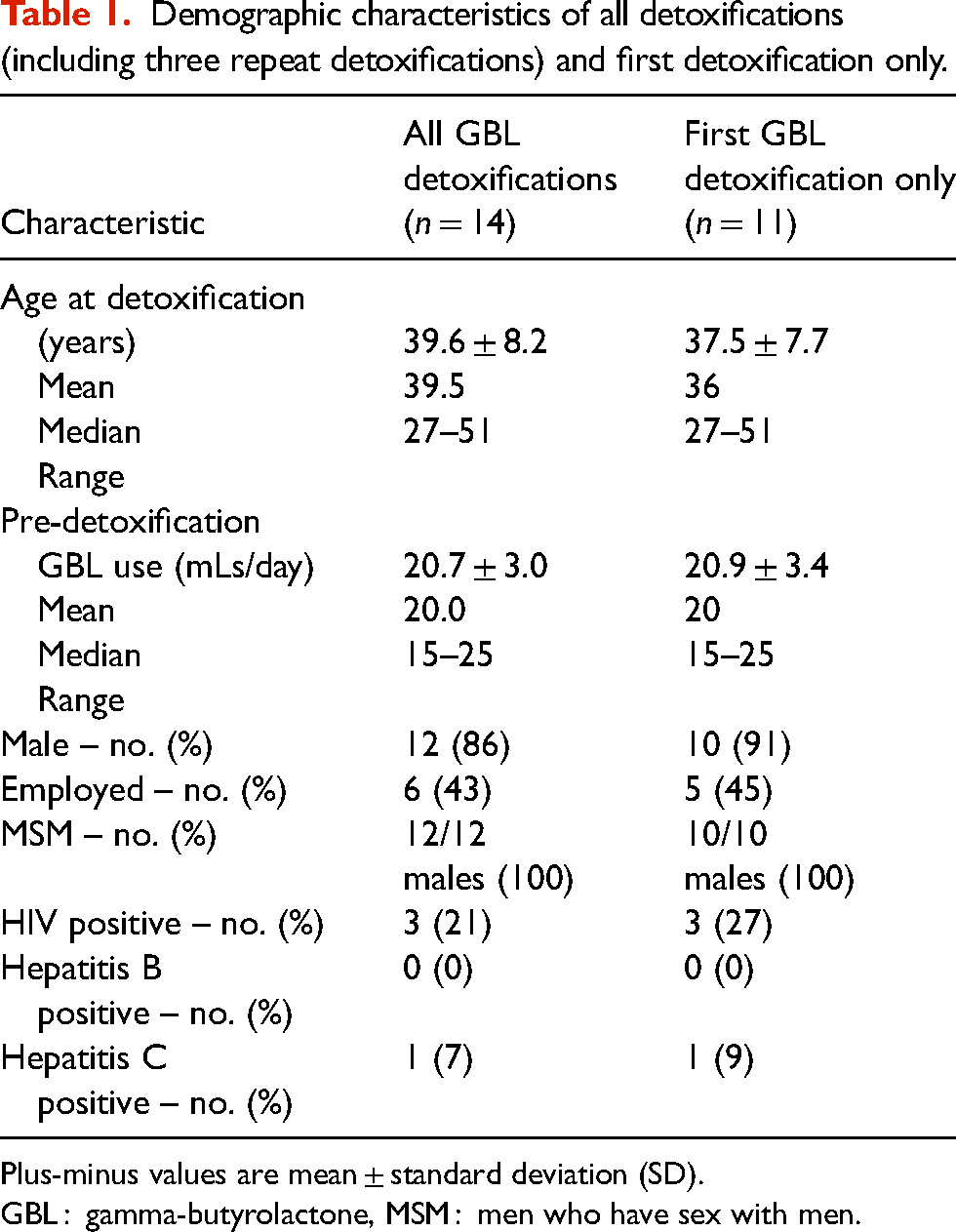
Plus-minus values are mean ± standard deviation (SD).
GBL : gamma-butyrolactone, MSM : men who have sex with men.
Six individuals were using other recreational drugs before detoxification: three used methamphetamine; one used methamphetamine and cocaine; one used mephedrone and alcohol, and one used benzodiazepines, zopiclone, cocaine and methamphetamine.
Ten out of 14 detoxifications (71%) were completed in the community. The four uncompleted detoxifications were excluded from further analysis regarding chlordiazepoxide dose and CIWA-Ar score.
The first patient that did not complete detoxification continued to use GBL and presented on day three with an increase in withdrawals having ceased GBL use. Given the difficulties in ensuring compliance with the detoxification procedures in the community, an immediate continuation of detoxification in an inpatient setting was arranged through the local acute hospital. The patient completed the detoxification and was discharged four days later. The second patient used methamphetamine on day one of the detoxification and subsequently relapsed to GBL use. The third patient stopped their detoxification on day one due to a visit from their parents, whom the patient did not wish to inform about their drug use. The fourth patient stopped the detoxification after five days due to a court hearing; the patient subsequently re-presented to the service two weeks later free from GBL.
Detoxification characteristics
All patients that completed a detoxification had a CIWA-Ar score of nine or below (absent/minimal withdrawal) on day two of the detoxification (Figure 2). The median CIWA-Ar score on the first day of detoxification was 11 with a range of 2–17 (Supplemental Table 1).

CIWA-Ar score by day of detoxification. Where more than one CIWA-Ar score was recorded per day, the highest CIWA-Ar score is shown.
The mean dose of chlordiazepoxide needed to manage withdrawal symptoms on the first day of detoxification was 144.0 mg (95% CI 115–173 mg, Supplemental Table 1). The mean prescribed chlordiazepoxide dose decreased each day except on day eight. This is because detoxifications that were longer than seven days had a higher mean chlordiazepoxide dose on day one compared to detoxifications that were seven days or shorter (147.5 mg vs 112.5 mg), and therefore had a longer tapering course (Figure 3). Successful detoxifications took a median of 9.5 days with the shortest being 7 days, and the longest being 14 days (Supplemental Tables 1 and 2).

Total daily dose of chlordiazepoxide (mg) by day of detoxification.
Discussion
The literature on GBL detoxification remains relatively sparse. This is especially true of detoxifications in an outpatient setting (e.g. community or ambulatory). Two previous reports on GBL detoxification were produced from this NHS trust – firstly in an inpatient setting in 2003 (McDonough et al., 2004) and secondly in 2011 in a specialist ‘club drug clinic’ (Bell and Collins, 2011). Both these services have ceased to exist; in part due to lack of funding (Kalk et al., 2018). In the case of inpatient treatment, there were no specialist NHS funded detoxification beds in the Greater London area at the time of this study, and a lack of sufficient activity and funding mechanisms to sustain a specialist outpatient GBL detoxification clinic.
In response to service user needs we developed an outpatient protocol to serve local GBL-dependent individuals. We have demonstrated that it is possible to manage GBL withdrawal in a community setting primarily focussed on other substances of dependence. This has been supported by close links with a local acute hospital in case of a crisis.
Most patients in this study declined the option of inpatient detoxification. On balance of risks, the decision was made to proceed with outpatient detoxification. Although English national criteria describing who can receive an outpatient GBL detoxification do not exist, our inclusion and exclusion criteria were informed by National Institute for Health and Care Excellence (NICE) guidelines for alcohol treatment (NICE, 2011).
Our detoxification procedures differed from much of the previous literature in that we used chlordiazepoxide, rather than diazepam (Bell and Collins, 2011, McDonough et al., 2004), pharmaceutical GHB or baclofen (Kamal et al., 2017). The reason was that these GBL detoxifications were taking place within a service detoxifying many more patients from alcohol. To fit within this alcohol detoxification structure and to reduce the chances of medication errors, we endeavoured to follow the same medication procedures as for alcohol; albeit in generally higher doses (from in-house data, the typical alcohol chlordiazepoxide dose on day one of a community detoxification was 80–100 mg).
Additionally, we used the CIWA-Ar to measure withdrawal symptoms. This has been suggested as perhaps insufficient to measure withdrawal from GBL (Lingford-Hughes et al., 2016). However, in the absence of a validated tool, we took the view that CIWA-Ar was suitable as GBL withdrawal resembles alcohol withdrawal clinically, with symptoms including autonomic overactivity, hallucinations, seizures and a state of delirium akin to delirium tremens (Kamal et al., 2017). Working within an alcohol detoxification treatment pathway, we found that the CIWA-Ar enabled monitoring of withdrawal symptoms over time and a consistent approach to chlordiazepoxide dosing.
Limitations
A limitation of this study is that patients self-reported their GBL use and the amount of ‘as required’ chlordiazepoxide taken, as well as their social history. With GBL dependence being an uncommon presentation, the sample size is limited. Furthermore, as this is an observational study of routine care it is not possible to directly compare the efficacy of chlordiazepoxide with other detoxification regimens. However, one study that used diazepam with baclofen for outpatient GBL detoxification reported the mean dose of diazepam prescribed in the first 24 h to be 75 mg (Bell and Collins, 2011), equivalent to 187.5 mg of chlordiazepoxide. This is comparable with the mean day one chlordiazepoxide dose in this study (144 mg).
Conclusion
This study demonstrates that for some patients it is possible to perform outpatient GBL detoxification in a service directed against wider substance dependence, adapting skills and protocols developed from the treatment of alcohol dependence. Like others (Bell and Collins, 2011; Kamal et al., 2017), we found that there are challenges in treating this patient group given the rapid onset and severity of withdrawals, and the lack of a suitable biological test for GBL use. Considering these challenges in the absence of specialist detoxification beds, it is important to have access to acute hospital admission if it proves impossible to continue the detoxification in the community.
Supplemental Material
sj-docx-1-dsp-10.1177_20503245231167544 - Supplemental material for The use of chlordiazepoxide for outpatient gamma-butyrolactone (GBL) detoxification: An observational study
Supplemental material, sj-docx-1-dsp-10.1177_20503245231167544 for The use of chlordiazepoxide for outpatient gamma-butyrolactone (GBL) detoxification: An observational study by Alfred Balston, Kuljit Hunjan and Michael J Kelleher in Drug Science, Policy and Law
Supplemental Material
sj-docx-2-dsp-10.1177_20503245231167544 - Supplemental material for The use of chlordiazepoxide for outpatient gamma-butyrolactone (GBL) detoxification: An observational study
Supplemental material, sj-docx-2-dsp-10.1177_20503245231167544 for The use of chlordiazepoxide for outpatient gamma-butyrolactone (GBL) detoxification: An observational study by Alfred Balston, Kuljit Hunjan and Michael J Kelleher in Drug Science, Policy and Law
Footnotes
Author contributions
Alfred J Balston: conceptualization, data curation – lead, formal analysis – lead, investigation, methodology, writing – original draft – lead, writing – review & editing. Kuljit Hunjan: conceptualization, data curation, investigation. Michael J. Kelleher: conceptualization, investigation, methodology, supervision – lead, writing – original draft, writing – review & editing.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.