
Abstract
Background
Opioid-related deaths are at record levels in the UK and contribute to over half of all drug-related deaths. The prevalence of psychiatric disorders within people who uses substances is known to be considerably higher than the general population, yet only 4% of people accessing treatment are thought to receive integrated care for coexisting conditions. This study aimed to explore perspectives on treatment for people with substance use disorders and coexisting psychiatric problems.
Methods
Face-to-face semi-structured interviews with community drug workers, specialist nurses, prescribing administration worker and one clinical psychologist were conducted. Deductive analysis of three preconceived themes (i.e. reasons for substance use, treatment provision, the role of medication) was conducted.
Results
There was agreement between drug treatment professionals and mental health professionals for the complexities for being in treatment for people who use substances. An expectancy of prolonged periods of abstinence from drug and alcohol use before psychological treatment would be initiated leading to relapse was reported. Individual judgements of practitioners, stigmatisation and fear of people who use substances and organisational barriers often meant psychological help was unavailable which contributed to a reliance on medication, against national clinical guidance which was known by only one interviewee.
Conclusion
The UK drug treatment and mental health services should review the pathways to ensure that national guidelines are followed so that people who use substances are not excluded from accessing psychological therapies. Data from the coronavirus pandemic indicates heightened psychiatric problems, where illicit drug use may escalate as a means of self-medication leading to further increases in drug-related deaths.
Keywords
Introduction
The UK drug-related deaths are at crisis level; of 4561 registered drug-related deaths in 2020, 64.5% involved opioids when deaths without drug type recorded were excluded (Office for National Statistics, 2021). Deaths involving cocaine doubled from 2015 (n = 320) to 2020 (n = 777) and cocaine remains the second highest used illicit drug after cannabis (Office for National Statistics, 2021). Substance use disorders do not occur in isolation. Social-ecological models of addiction identify complex interactions between the individual, social relationships, community engagements and societal structures influence drug-seeking behaviours (Jalali et al., 2020). In 2013, a change in the UK benefits system amalgamated all existing payments into one. This led to payment delays, increasing debt and a rise in the use of food banks (Walker, 2019). Drug-related deaths in the UK increased by 41.17% between deaths reported in 2011 (n = 2652) and deaths reported in 2016 (n = 3744) (Office for National Statistics, 2011; Office for National Statistics, 2016). Up to 90% of overall substance use is non-problematic for drugs associated with dependency such as methamphetamine and heroin (Schlag, 2020) so drugs are not the sole cause of problem drug use. Greater understanding of the causes of substance use will allow for targeted drug-related death prevention strategies at population level. An important such influence on drug use are coexisting psychiatric disorders.
Exposure to traumatic events has been detected in up to 88% of people who use heroin with childhood sexual abuse, emotional abuse, physical neglect and violence typical (Lawson et al., 2013). Consequently post-traumatic stress disorder (PTSD) can develop, associated with poorer physical and mental health, suicide attempts and depression (Mills et al., 2006). Schizophrenia and psychosis are often diagnosed alongside PTSD (NICE, 2014), however, symptoms can be confounded at assessment by symptoms of opioid withdrawal (Patel et al., 2017). There is a similar complex interaction with depression and anxiety (Clinical Guidelines on Drug Misuse and Dependence Update, 2017) leaving clinicians with the dilemma of assessing whether patients who use opioids are in psychological distress, physically withdrawing from opioid dependence or both. One way to reduce uncertainty is by ensuring the patient is in receipt of opioid substitution therapy at doses known to eliminate withdrawal but under-dosing is common practice in England (ACMD, 2015), further impeding psychiatric comorbidity detection by maintaining people in mild opioid withdrawal. Cannabis is the most used illicit drug globally and dependent people who use cannabis are over five times more likely to have a related anxiety disorder, 73% of these meeting criteria for a primary anxiety disorder (Buckner et al., 2012). Up to 80% of adults with attention deficit hyperactivity disorder have a coexisting mental health problem including mood and anxiety disorders, personality disorders and a bidirectional relationship with substance use disorders is widely accepted (Katzman et al., 2017). Use of cannabis, alcohol, cocaine, amphetamines and nicotine are most prevalent where people use substances to self-medicate mood or aid sleep. As with opioid dependence, overlapping symptomology can lead to misdiagnosis and delays in treatment. It is clear that identification of psychiatric disorders within people who use substances is complex.
Multiple factors affect progress of psychiatric disorders and the influence of societal structures are particularly apparent in relation to substance use. In 2010, the UK government launched a new drug strategy (HM Government, 2010) which focused on achieving independence (‘recovery’) from both illicit opioids and substitute opiates. This differed from previous policy where opioid dependent individuals could receive substitute opiates indefinitely. Although the new UK strategy did not state that people could not be maintained indefinitely on substitute opiates, community treatment services were monitored for number of successful completions. In the case of opioid users, this meant exiting treatment free of all opioid use including substitute opioids for at least 1 month and not returning to structured treatment for at least 6 months. A payment-by-results model was trialled whereby treatment services received payments for these successful completions amongst other key performance indicators such as reduced injecting practice. Observational studies of 154,175 people accessing drug and alcohol treatment (10,716 in payment-by-results localities and 143,459 in treatment-as-usual localities) between 2010 and 2014 found that payment-by-results led to lower numbers of treatment initiation and lower numbers of completions, but there was no significant changes in housing, criminal activity or mortality within services (Jones et al., 2018). Retention in treatment on substitute opiates is a protective factor in reducing opioid-related deaths with most opioid-related mortality found in people not accessing treatment (Clinical Guidelines on Drug Misuse and Dependence Update, 2017). The changes in how the UK drug treatment services were monitored in the 2010 drug strategy were not incentivised for services to allow for evidence-based treatment provision that reduced opioid-related deaths.
Recent impact of social change on psychiatric disorders is already being seen during the COVID-19 pandemic, where one cohort study of 3097 UK adults found 64% of participants reported symptoms of depression and 54% reported symptoms of anxiety. Of these, 31.6% met the criteria for moderate-to-severe depression and 26% moderate-to-severe anxiety qualifying for high-intensity NHS psychological treatments (Jia et al., 2020). This contrasts with 10% of the general English population typically estimated to meet the criteria for depression and 5% expected to meet anxiety criteria (Stansfeld et al., 2016). It is clear that socio-economic changes impact the onset of psychiatric disorders.
The estimated prevalence of psychiatric problems within drug and alcohol services ordinarily is between 60% and 93%, of those 4% receive integrated substance use disorder and mental health treatment (Guest and Holland, 2011). This is compounded by only 1% of global healthcare workforce employed for provision of mental health care (World Health Organization, 2016). With such a small pool of available resource to identify and treat coexisting mental health problems in people who use substances, there is an obvious requirement to understand how this treatment need might be met. To our knowledge, there is no other qualitative research contextualising the experiences and perceptions of drug treatment professionals (DTPs) and mental health professionals (MHPs) who deliver services. As such, this service evaluation aimed to explore their perspectives on psychiatric diagnosis and treatment for people with substance use disorders and coexisting psychiatric problems.
Methods
The study design was a service evaluation as a pilot study for the methodology using individual semi-structured interviews to explore the perspectives and experiences of DTPs and MHPs regarding three preconceived themes: (1) Reasons for substance use; (2) Treatment provision for people who use substances who have coexisting psychiatric diagnoses; (3) The role of medication in treatment of individuals who use substances with coexisting psychiatric diagnoses.
Rationale
The qualitative data reported here were collected as part of a larger, unpublished PhD thesis study examining the prevalence of diagnosis of psychiatric disorders amongst people in England where opioids were found at post-mortem between 2006 and 2015 (Houghton et al., 2020). Two key findings were lower prevalence of reported psychiatric problems in deaths in England, where opiates were found at post-mortem versus prevalence of psychiatric disorders in the general population and escalating numbers of prescription medications were found in deaths in England where opiates were found at post-mortem between 2010 and 2015 inclusive. Interviews were initiated to add context to this data around why this may be the case.
Recruitment and sampling
Convenience sampling was used to recruit both drug treatment (n = 6) and community mental health (n = 2) professionals. Convenience sampling recruits participants based on accessibility and availability is quick and inexpensive (Elfil and Negida, 2017). Interviewees were comprised of community drug workers who provide psychosocial interventions (motivational interviewing, cognitive behavioural therapy, etc.) to people who use substances (n = 4), substance use disorder specialist nurse (n = 1) prescribing administration worker who generates prescriptions within the drug service for people who use substances (n = 1), mental health nurse (n = 1) and clinical psychologist (n = 1). Participants were recruited from two community drug treatment services operated by a single non-statutory treatment provider, Cranstoun, and one NHS organisation, Berkshire Healthcare Foundation Trust, who provide mental health services to the regions where both drug treatment services operate. Professionals working within the mental health treatment pathways only were included. The final sample comprised of one male and five females from two drug treatment services and one male, one female from the mental health services in one location. Participants were White British (n = 5), Black African (n = 2) and Asian (n = 1).
Interviews were conducted with eight professionals by one white, male author (BH). The interview schedule was designed by BH and reviewed by CN prior to interview start. One DTP had been working in the field for less than 2 years with the remainder having at least 5 years’ experience of working with people who use substances. The DTPs had broad experience of working with people who use substances in multiple settings across differing geographical regions such as community drug treatment services, the criminal justice system, homeless hostels and women's refuges. One substance misuse nurse had worked within statutory mental health services and one community drug worker was qualified in counselling. MHPs had experience working with people who use substances in supported living, on acute wards in inpatient psychology units, leading psychology teams, within child and adolescent mental health services and with crisis teams. All DTPs and one clinical psychologist from the MHPs described a personal experience either through self or others with addiction.
Data collection
Participants were interviewed once in June 2019, privately digitally recorded at each participant's place of work with nobody else present during interview. No participant had visibility of the interview schedule prior to interview. Emails to all staff were sent by their managers informing them of the non-mandatory and confidential opportunity to attend a research interview regarding substance use and mental health. Interviews with DTPs took place on two dates, 1 week apart. Three attempts across 2 months to interview MHPs were made, however, despite organisational willingness to participate, continued staffing shortages meant only two were interviewed. The nature of the interview was explained and participants were given the opportunity to wait 24 h before deciding whether they wanted to take part prior to signing consent forms. No participant asked to consider their involvement or withdrew following consent. Interviews ranged between 15:06 and 39:19 min in length, no handwritten notes were made during the interviews and no interviews were repeated. All participants were offered visibility of their final transcript, none requested this. No reimbursement was given. The interview schedule is available in Supplemental material.
There was complete discussion with potential participants who gave written informed consent. NHS ethical approval was not required for professional interviews as this study was deemed service evaluation.
Analysis
Interview recordings were transcribed verbatim and anonymised. A deductive framework was devised and thematic framework analysis was conducted (Gale et al., 2013). Themes were preconceived by one male author (BH). Nvivo12 software was used to aid analysis. Digital recordings of interviews were deleted immediately following transcribing. Interviews were read with an open mind; however, BH had an established relationship with 3 of the DTPs and 0 of the MHPs. Due to convenience sampling, interviews were susceptible to self-selection bias either from community drug workers desire to support an ex-colleague or from a desire to express existing opinions on the interview topic. To minimise the influence of BH preconceptions and rationale for undertaking the research, coding was checked by one female author with no relationship to the participants (CN) and discussed where disagreements in coding were found. As the senior academic, CN decision was final.
Although a number between 6 and 12 interviews may be enough to reach data saturation (the point at which no new information, codes or themes are found), the preconceived deductive approach of our analysis in a small sample size meant achieving data saturation was questionable and neither appropriate nor useful for our study design (Braun and Clarke, 2021).
The study was conducted in accordance with the Declaration of Helsinki. This paper complies with COREQ reporting standards (Tong et al., 2007).
Results
Table 1 demonstrates the topics identified by all DTPs and MHPs. Interviewees agreed that psychiatric disorders were highly prevalent in people who use substances. Interviewees agreed that funding cuts on treatment services had stretched services and that there was an over-reliance on prescribed medication. Minor themes were not explored as the small sample size meant minor themes were assessed as being individual opinion but descriptions can be found within the coding tree (Figure 1). To protect anonymity, the three preconceived major themes are described through anonymous quotations labelled by cohort, i.e. DTP or MHP.
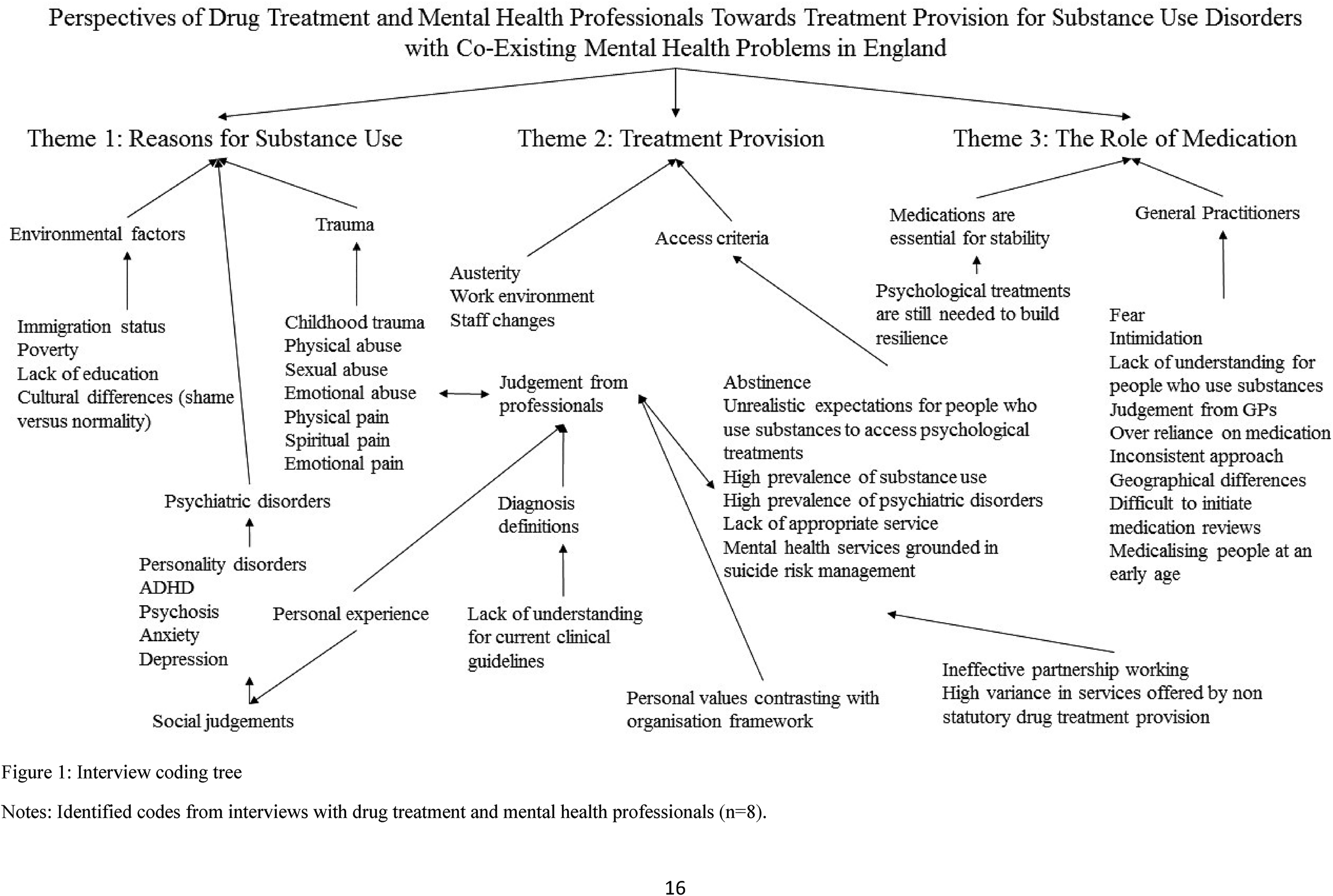
Interview coding tree.
Common topics identified during interview.

Note: Topics which were identified by all interviewees (n = 8) during thematic framework analysis coding.
Reasons for substance use
“We don’t exist in a vacuum there's several things going on around us, all of those things are contributing to our sense of who we are, our identity, our desires and all those things shape how we see the world and I think mental health and mental illness is a response to that” (431-1, Clinical Psychologist, MHP)
Environmental factors such as immigration status, poverty, lack of education and cultural differences were reported by all DTP and one MHP as playing a role in the onset of substance use.
“…trauma seems to be the biggest underlying instigator of people picking up substances…I think it's about what people experience and how they cope with what they experience. I think it triggers, trauma triggers a lot of mental health issues…yeah the way I see it trauma is a big, massive, underlying issue” (430-1, Community Drug Worker, DTP)
Childhood trauma was recognised by DTPs. DTPs and MHPs estimated prevalence of psychiatric problems with substance use disorders to be upwards of 80% of all service users. Childhood trauma was seen as denying exposure to modelling of coping mechanisms by DTPs and one MHP referenced pain as a reason for substance use.
“I see that person in a great deal of pain and they don’t know how else to soothe this pain and so that's why they use the substances. It's a way of escaping the pain, the turmoil, sometimes its spiritual pain, emotional turmoil, it could be physical pain” (431-1, Clinical Psychologist, MHP)
Personality disorders, attention deficit hyperactivity disorder, psychosis, anxiety and depression were suggested pre-existing conditions by both cohorts which people may seek relief from through substance use.
One female, White, late-20s community drug worker believed people who used substances were unfairly judged: “I think people are judged very much. The same as mental health like 20 years ago or 30 years ago everyone was judged for having mental health like ‘oh you’re a nutter’, that's moved on but substance misuse hasn’t” (430-4, Community Drug Worker, DTP)
Moral judgements were detected:
“…people who are making life choices and that's their decision but if they’re knocking on mental health doors in my opinion, well you need to address your substance use first…don’t come knocking on the door when you realise after you’ve been using crack and heroin for fifteen years and its completely destroyed your life. That's my personal opinion” (431-2, Mental Health Nurse, MHP)
There was overall agreement regarding complexity of people who use substances.
Treatment provision
MHPs and DTPs suggested relaxing criteria from Community Mental Health Teams (CMHT) to allow people who use substances to access mental health services was seen as achievable change. One White, male, mid-30s mental health nurse reported an independent audit of referrals to statutory mental health services across a 4- month period in 2017, 3% met CMHT thresholds and of those 2% were accepted. Acceptance meant people receive an opt-in letter and discharged if they made no contact. Requirements for sobriety were ratified by both MHPs who confirmed current drug use resulted in automatic referral decline unless psychiatric disorders were diagnosed prior to initiation of substance use.
“if they’ve got a severe and enduring disorder that's already established then they’re using drugs on top of that, that is dual diagnosis…Someone who's had a traumatic upbringing, is very dysfunctional and using drugs is not going to meet their criteria” (431-2, Mental Health Nurse, MHP)
“…a particular referral has taken almost 6–7 months before that persons got an appointment with a clinical psychologist It's just impossible for people to just be seen very quickly. For the crisis team for example, it's very short, sharp interventions…the diagnosis is complex emotional personality disorder, emotional disorder so virtually no sort of coping mechanisms to deal with anything that can trigger an emotional reaction or response. That client is very dependent on alcohol…in and out of hospital for detoxes but because she comes out of her detox and goes straight back home, home is her trigger she’ll pick up alcohol straight away after a detox…thereby making herself unable to receive the next level of care in mental health services, she's very, very high risk of completing suicide but the crisis team are there providing those emergency interventions but that's as far as it can go…the next stage, you have to be mentally robust in order to start, I’ve never quite understood that because it's chicken and egg isn’t it? The criteria is a minimum of 3–5 months of sobriety from the problem substance so it's chicken and egg” (430-2, Community Drug Worker, DTP)
Drug and alcohol use was reportedly present in 70%–80% of referrals to mental health services followed by problems related to benefits sanctions.
“drug and alcohol is the big one. It's under-reported by the GPs…I assessed a client yesterday, she smokes cannabis every day, is that gonna be preventative for therapy? Therapeutic services in secondary care or primary care with Talking Therapies will say if a client is using crack, alcohol, abusing heroin or using cannabis or whatever then they’re not going to be eligible for therapy” (431-2, Mental Health Nurse, MHP)
One female, African substance misuse nurse with qualifications and employment history in mental health nursing across multiple localities had seen treatment provision from the perspective of both drug treatment and mental health professionals: “when they are referred to mental health they just think whatever they’re using is causing the mental health issue whereas from the drugs area we think the mental health issue is the one that's causing them to use the drugs so they don’t really get proper treatment. Wherever I’ve worked it's just going back and forth with the mental health people, they will say ‘ask the person to stop using this then we can see them’. I think I understand where they are coming from, the person who uses drugs aren’t thinking clearly but they don’t really get proper treatment in my own perspective” (430-3, Substance Misuse Nurse, DTP)
Lack of specialist services was identified: “We assess them and nine times out of ten it's either refer it to the crisis team or signpost to drug and alcohol…if we were going to be really honest with these patients we’d say we’re not offering you an assessment because there's nothing to offer you at the end of this assessment so we’re giving them false hope… we’re assessing them to make sure that we’ve done an assessment and said we’ve done an assessment” (431-2, Mental Health Nurse, MHP)
This experience was supported by DTPs.
“…there is a high level of people needing mental health services and they’re under resourced however my experience is that they can be really dismissive and once a person is engaged with another agency, another service they feel they don’t really have to do anything” (430-1, Community Drug Worker, DTP)
Organisational frameworks contrasted with the beliefs of one female, African clinical psychologist: “I’m against these one size fits all rules, I think it depends on the person. If you have a substance misuse problem but you’re able to engage in therapy… you can turn up to therapy sober and maybe be part of a therapeutic group… if you’re able to make use of the therapy then why should you be denied treatment” (431-1, Clinical Psychologist, MHP)
In order to provide psychological treatments, DTPs operated a counselling service where abstinence was not a prerequisite: “Clients just rave about their experience with the counsellors…not to say that they have stopped using or that they’re not still relying on substances in some shape or form at some level, it's not a cure but it is there to give clients a really good experience and build up there coping mechanisms” (430-2, Community Drug Worker, DTP)
DTPs supported partnership working without requiring abstinence from substances before accessing psychological treatment. MHPs felt drug treatment should be managed by the NHS as non-statutory providers differ significantly in services offered, hindering partnership working. One DTP from the six interviewed knew the national guidance for working with coexisting mental health problems and substance use disorders but neither MHP knew what guidance directs.
The Role of medication
Medication was unanimously viewed as essential for stability in severe and enduring conditions but generally should not be prescribed in isolation. DTPs felt psychological therapy was critical to provide coping strategies and resolution of trauma.
“GPs don’t help at all from what I’ve seen. They just overload them with a variety of drugs that they are using and then buying extra on the street in addition. Also they’re getting medicated then selling them on without even using them themselves in some instances” (430-5, Prescribing Administrator, DTP)
“they might have had a diagnosis but they’re still on the same medications for many years, when you know they might not need that level of medication” (430-2, Community Drug Worker, DTP)
General Practitioners (GPs) were thought to prescribe antidepressants without offering alternatives such as nutritional advice and counselling. One male, white, mental health nurse suggested GPs feel threatened, intimidated or pressured to prescribe medications. These patients are then referred to CMHT who then redirect to drug treatment services creating a perpetual loop. One White, male community drug worker who had worked in multiple localities identified differences in GP prescribing depending on geographical region: “It seems here, whatever you want you’re gonna get even if you make stuff up…a lot of my clients on medication are on various types, all on the same script…one client over in <place>, mirtazapine, tramadol, oramorph, quetiapine and something else I can’t remember what that is. I think she's on two kinds of antidepressant sertraline I think the other one was. Why? Do you know what I mean?” (430-6, Community Drug Worker, DTP)
Medication reviews were reportedly difficult to initiate despite patient request One female, Asian community drug worker cited lack of GP understanding for people who use substances and because of illicit use, ‘the shutters come down’. Another female, African substance misuse nurse stated: “Theres still some judgemental attitude there. I remember working in GP shared care, all the doctors would do is just print the script and sign then you were like this person is due for medical review but it wasn’t a concern for them as much as someone who doesn’t use. For them it was like this person has put it on themselves” (430-3, Substance Misuse Nurse, DTP)
One White, male mental health nurse suggested medicalisation can begin during adolescence. “there was one girl, she was 15 she had a diagnosis of ASD, conduct disorder, psychosis, you name it she had every diagnosis under the sun. She was 15 and she was on sodium valproate, diazepam, some really sedating medications, antipsychotics…she was 15. Like she’d been medicalised” (431-2, Mental Health Nurse, MHP)
Discussion
There was consensus for the complex nature of supporting individuals with coexisting psychiatric disorders and substance use disorders. The need for psychological treatments was encouraged by interviewees, but a perception of organisational barriers was found to block access to these for people who uses substances from both DTPs and MHPs.
The small cohort of MHPs prohibited exploration of whether childhood trauma influenced substance use was supported by MHPs (Theme 1). Both MHPs reported differences in opinion in comparison to unanimous belief amongst DTPs. Greater exposure to the holistic needs of the client group in DTPs and differences in specialist training between MTPs and DTP may provide some explanation to the differing views, but this contrast of professional opinion further highlights the complex interaction between environmental influences, mental health problems and substance use disorders.
Organisational barriers were suggested to be produced by austerity affecting provision of services as demonstrated by difficulties in interviewing MHP. Recent analysis of disinvestment in 151 of 152 local authority commissioned UK drug and alcohol treatment services between 2013/14 and 2018/19 found that local authority spending cuts were associated with fewer people accessing and completing treatment but were not associated with deaths (Roscoe et al., 2021). Evidence shows that retention in drug treatment is a protective factor against mortality and so it is surprising that fewer people in treatment is not associated with the increase in mortality. This may suggest that whilst austerity has an impact on the ability of services to provide treatment, it is the quality and appropriateness of the treatment which has a greater influence on mortality. Current substance use was present in the majority of referrals to CMHTs and benefits sanctions were the second highest characteristic of referrals (Theme 2) supporting evidence that social and economic change negatively affects mental health and reflecting the impact of austerity on mental health (Malcolm et al., 2019). Although professionals agreed specialist services were needed for people who use substances with psychiatric problems, services already exist within CMHT and trauma teams (NICE, 2016). Theme 2 demonstrated organisational gatekeeping hinders access to these mental health services. UK quality standards recommend substance use and severely intoxicated presentation should not be reason to exclude people (NICE, 2019) and UK guidance recommends proactive service led approaches to engage this population in treatment (NICE, 2016). Our findings suggest guidance is not being followed. Wider revaluation may be required if quality standards are not pragmatic to deliver within current service capacity.
The validity of psychiatric diagnosis has been debated with viewpoints who prefer symptom triggered treatments arguing diagnosis results in a disingenuous categorical system (Allsopp et al., 2019). Whilst this may explain perceived reliance on medication (Theme 3), lack of diagnosis is a barrier to receiving statutory psychological therapies (Theme 2). It is important that medications are not demonised as they may play a crucial role in the stabilisation of symptoms prior to initiation of psychological therapies. However, NHS prescribing trend increases between 2006 and 2015 show increases of antidepressant items dispensed by 0.98˟, antiepileptics 1.33˟, hypnotic/anxiolytics 0.0027˟, antipsychotics and related disorders 0.51˟. Opioid analgesics, which included non-steroidal anti-inflammatory drugs as well as opioids, increased by 0.38˟ (NHS Digital, 2017). This period coincides with socio-economic change and self-reported substance use during referral for mental health services may have created detection bias (Theme 2), prohibiting assessment leading to prescription medication only as treatment. This reliance is reflected in emerging evidence showing opioid analgesics are increasingly used to manage emotional problems, supporting self-medication theories (Cicero and Ellis, 2017), research showing increasing opioid prescribing correlation with opioid-related deaths (Taylor et al., 2019) and non-prescribed opioid analgesic recreational use (Yedinak et al., 2016). The complexities of overlapping symptomology between psychiatric disorders and substance use disorders should be shared to increase treatment provider understanding and formulate trauma informed treatment plans rather than be used as rationale for which agency is accountable for suicide risk (Theme 2).
This analysis highlights professional views of a population asking for help but organisational barriers often mean psychological help is unavailable. The key differences between medication prescribed by professionals and illicit substances used to manage coexisting mental health problems are legal status and the known purity of each substance. People who use substances are required to stop using the illicit substances which they know provide immediate relief for at least 3 months (Theme 2) without normative coping skills in place prior to accessing psychological therapies. The psychological therapies themselves will not provide the comparable, immediate relief of illicit substance use and so abstinence from illicit substance use is unlikely to be an attractive proposition. From a behavioural economic viewpoint, people who use substances with psychiatric disorders then choose short-term gain (substance use) and long-term sacrifice (health implications, risk of overdose) (Rachlin, 2007). This seems irrational to people who do not use substances but for people who use substances, this is the optimal choice where maladapted coping mechanisms exist (Theme 1), creating a vicious cycle of continued substance use that prohibits access to evidence based psychological therapies due to organisational barriers.
Strengths and limitations
Interviews were undertaken with a small sample size across two localities and subject to self-selection bias. Data were self-reported and all accounts were taken at face value, representing the ‘truth’ for individuals at the time of interview, rather than universal ‘truth’. However, detailed narratives echo globally identified barriers in accessing evidence based treatment (World Drug Report, 2019) and reflect estimates in prevalence of psychiatric disorders within drug treatment services (Guest and Holland, 2011). Larger qualitative studies to explore the perceptions of professionals working within care pathways towards people who use substances with coexisting psychiatric problems are warranted.
Conclusion
DTPs and MHPs share understanding of the complex interactions between substance use disorders and coexisting mental problems. Barriers to access psychological therapies are organisational in nature and result in reliance on medication to manage symptoms. This is correlated in national prescribing trends with escalating drug-related deaths (Taylor et al., 2019) and periods of socio-economic unrest Findings suggest that the UK drug treatment and mental health services should review the pathways to psychological therapies to ensure national guidelines are followed so that people who use substances are not excluded from accessing psychological therapies. Data from the coronavirus pandemic indicates heightened psychiatric problems, where illicit drug use may escalate as a means of self-medication leading to further increases in drug-related deaths.
Supplemental Material
sj-docx-1-dsp-10.1177_20503245211055382 - Supplemental material for Perspectives of drug treatment and mental health professionals towards treatment provision for substance use disorders with coexisting mental health problems in England
Supplemental material, sj-docx-1-dsp-10.1177_20503245211055382 for Perspectives of drug treatment and mental health professionals towards treatment provision for substance use disorders with coexisting mental health problems in England by Ben Houghton, Alexis Bailey, Christos Kouimtsidis, Theodora Duka and Caitlin Notley in Drug Science, Policy and Law
Supplemental Material
sj-docx-2-dsp-10.1177_20503245211055382 - Supplemental material for Perspectives of drug treatment and mental health professionals towards treatment provision for substance use disorders with coexisting mental health problems in England
Supplemental material, sj-docx-2-dsp-10.1177_20503245211055382 for Perspectives of drug treatment and mental health professionals towards treatment provision for substance use disorders with coexisting mental health problems in England by Ben Houghton, Alexis Bailey, Christos Kouimtsidis, Theodora Duka and Caitlin Notley in Drug Science, Policy and Law
Footnotes
Acknowledgements
Professionals for qualitative interview were provided by the Cranstoun Group and Berkshire Healthcare Foundation Trust. Neither organisation had a role in study design, data collection, data analysis, data interpretation or writing of this report.
Disclosures
BH was employed by the Cranstoun Group as a psychosocial recovery worker at the time of conducting interviews. There are no further disclosures by the authors to make.
Funding
No funding support has been received for this study.
Declarations of competing interests
BH was employed by the Cranstoun Group as a psychosocial recovery worker at the time of interview. There are no further disclosures by the authors to make..
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.