
Abstract
Background
It has been suggested that the outcome of the psychedelic experience is dependent on set and setting. While scientific research into the therapeutic potential of psychedelics is growing, it is clear that in clinical populations an optimal set and setting will not always be attainable. It was aimed to assess under which emotional and environmental circumstances psychedelic users use psychedelics, and the outcome of use given clinical characteristics, defined as low well-being and higher rates of neuroticism.
Methods
Online respondents (N = 1967) provided information about their psychedelic use, environment they consume the substance in (setting), and mood state pre/post-substance (set). Based on subjective mental well-being, respondents were separated into two groups, those with low (N = 643), and those with normal well-being (N = 1324). Personality traits, with a particular focus on neuroticism, were also assessed.
Results
Findings showed that psychedelics such as lysergic acid diethylamide and psilocybin were most commonly used at home and methylenedioxymethamphetamine (MDMA) in a party/festival setting. In most instances, all substances were used when individuals were in a positive mood, and this remained in general positive, or, when not initially positive, shifted to positive, after use. Individuals with low well-being were more likely to experience a positive mood change after use of lysergic acid diethylamide, psilocybin or MDMA than individuals with normal well-being. Furthermore, as neuroticism scores increased, so did likelihood of positive mood change, as well as likelihood of experiencing negative side effects.
Conclusion
It is demonstrated that psychedelics are used in varying emotional states and environmental settings. Importantly in the light of future clinical studies with patients, individuals with low psychological well-being and higher scores of neuroticism report consuming such substances with positive outcomes.
Introduction
Psychedelic drugs are a class of substances including classic psychedelics, like lysergic acid diethylamide (LSD), psilocybin, and dimethyltryptamine (DMT) found in ayahuasca, and empathogens, like methylenedioxymethamphetamine (MDMA). When ingested, they induce profound altered states of consciousness including acute alterations in perception and cognition, and amplified emotional states (Preller and Vollenweider, 2018). Currently, there is a renewed interest in the use of psychedelics in the treatment of certain psychiatric conditions (Carhart-Harris et al., 2016; Carhart-Harris and Goodwin, 2017; Mithoefer et al., 2018; Sessa, 2014). Specifically, recent clinical studies have suggested that LSD (Gasser et al., 2014), psilocybin (Carhart-Harris et al., 2016), ayahuasca (Palhano-Fontes et al., 2018), and MDMA (Mithoefer et al., 2011, 2018) can provide therapeutic relief for those suffering from post-traumatic stress disorder, anxiety, and depression. Importantly, non-pharmacological factors, termed set and setting, have been suggested to mediate the long-term (therapeutic) effects of these substances (Eisner, 1997; Haijen et al., 2018; Hartogsohn, 2017; Kaelen et al., 2018; Leary et al., 1963; Metzner and Leary, 1967).
Set refers to the internal state of the individual taking the substance, including mood, expectations, intentions, and pre-existing psychological factors, and setting refers to the physical and social environment the substance is taken in (Leary et al., 1963). Previous research with psychedelics suggests that the acute substance experience can be highly influenced by these non-pharmacological factors; studies have suggested that the outcome of the experience can be mediated by trait personality factors (Barrett et al., 2017; Haijen et al., 2018; Studerus et al., 2012), pre-existing psychological well-being (Studerus et al., 2012), mood state prior to substance intake (Studerus et al., 2012), and exposure to highly clinical, experimental settings (Studerus et al., 2012) and music (Kaelen et al., 2018).
With the renewed interest in the use of psychedelics in the treatment of these psychiatric conditions (Carhart-Harris et al., 2016; Carhart-Harris and Goodwin, 2017; Mithoefer et al., 2018; Sessa, 2014), it is important to define the most optimal circumstances for administration of these substances. Specifically, as psychiatric populations are often characterized by low psychological well-being and higher traits of neuroticism (Kotov et al., 2010; Saklofske et al., 1995), two set factors previously suggested to negatively impact the psychedelic experience (Barrett et al., 2017; Studerus et al., 2012), it is important to establish whether psychedelics are still a suitable therapeutic option, not leading to negative mood or (more) negative, unwanted effects. Although current clinical trials are small, including only a small number of highly selected/screened individuals, there is a wealth of information to be gained from recreational users, who report using the substance in various emotional and environmental circumstances, and for a number of different (therapeutic) reasons (Kettner et al., 2019; Mason and Kuypers, 2018).
The present study was therefore designed to assess under which emotional (set) and environmental (setting) circumstances psychedelic users use such substances, and the outcome of use, per substance, given clinical characteristics, namely low psychological well-being and higher traits of neuroticism (Kotov et al., 2010; Saklofske et al., 1995). Psychedelic users were asked what setting they usually used the substance in, and were asked what mood (set) they were in prior to, and after, substance intake. In order to assess outcome of use in individuals with clinical characteristics, respondents’ were divided into normal well-being and low well-being groups, dependent on their World Health Organization (WHO)-5 well-being index score. Furthermore, personality traits, with a particular focus on neuroticism, were assessed and compared between groups. This study is part of a larger questionnaire, which has previously been published elsewhere (Kettner et al., 2019; Mason and Kuypers, 2018).
Method
Design
An online questionnaire was launched on several websites and forums
In total 4892 participants started the survey and 1967 respondents (40%) consented, were 18 years or older, and completed the questionnaire (Figure 1). The duration to complete depended on the number of substances a person had ever used before. It was possible to pause the survey and complete it at another time. It took respondents on average 96 minutes to complete.

Flow chart of study respondents.
Measures
Demographic information
Demographic details included age, gender, history of a mental health disorder, of origin, and the highest level of education. The level of education was recoded into six separate categories (<high school; high school degree/equivalent; university/college; advanced/post-graduate degree; vocational/trade school; not specified). Continent of origin, age, gender, mental health history, and education will be reported to provide population information of the included sample.
History of substance use
Respondents were asked whether they had ever used or still currently used the empathogen MDMA/Ecstasy, or the classic psychedelics psilocybin, LSD, or ayahuasca. If respondents indicated that they had used one of the substances before, they were further asked about their use, including if they had ever experienced any unwanted or negative effects. The latter question could be answered with yes/no, and no further details were asked. Further questions about use have been described elsewhere (Kettner et al., 2019; Mason and Kuypers, 2018).
Setting
If respondents indicated that they had used one of the substances (MDMA/ecstasy, psilocybin, LSD, or ayahuasca), they were further asked in which setting they usually used the substance in. Respondents were able to choose between a party setting, festival setting, home setting, work setting, ceremonial or spiritual setting, or an “other” setting, in which they could specify. They were allowed to select all settings that applied.
Set
If respondents indicated that they had used one of the substances (MDMA/ecstasy, psilocybin, LSD, or ayahuasca), they were further asked which mood state (positive, negative, neutral, or other) they were usually in when they decided to use it. They were further asked if the mood state usually changed during use (yes, no), and, if yes, what mood state (positive, negative, neutral, or other) this usually changed to. If respondents indicated that they usually used the substance in a negative or neutral mood, and reported that their mood changed to a positive mood after use, this was recorded as a “positive mood change.” Subsequently, if respondents indicated that they usually used the substance in a positive or neutral mood, and reported that their mood changed to a negative mood after use, this was recorded as a “negative mood change.” As analyses were hypothesis
Well-being
The WHO-5 Well-being Index is a short, self-administered questionnaire assessing subjective psychological well-being and covering five positively worded items, related to positive mood (good spirits, relaxation), vitality (being active and waking up fresh and rested), and general interests (being interested in things). It has been shown to demonstrate good construct validity as a unidimensional scale measuring well-being, high reliability (Dadfar et al., 2018), and to be a reliable measure of emotional functioning, as well as a good screener for depression (Topp et al., 2015).
Each of the five items is rated on a 6-point Likert scale from 0 (=not present) to 5 (=constantly present). Scores are summated and multiplied by 4 to yield the WHO-5 score, a well-being index running from 0 to 100 with higher scores meaning better well-being. Evidence suggests a score of 50 or below is indicative for low mood, though not necessarily depression. A score of 28 or below indicates likely depression and warrants further assessment (diagnostic interview) to confirm depression (Bech et al., 2003; Topp et al., 2015).
Personality
In order to assess the personality profile of participants, the Big Five Inventory 10-item version was used (Rammstedt and John, 2007). Each item is scored on a scale from 1 (disagree strongly) to 5 (agree strongly); five personality trait domains can be distinguished: Extraversion, Agreeableness, Conscientiousness, Neuroticism, and Openness to experience. The 10-item version has been found to be generalizable across items, as compared to the full item version, generalizable across time, and demonstrated to have sufficient structural and convergent validity and retest reliability (Rammstedt and John, 2007).
Statistical analysis
Data entered the statistical program SPSS (version 24.0). Respondents were divided into two groups based on their well-being score. Those with a well-being score of greater than 50 were categorized with “normal” well-being, and those with a well-being score of 50 or less were categorized as “low” well-being (Topp et al., 2015).
Frequencies (N) and proportions (%) are reported for respondent demographics, substance use history, substance use setting, mood before and after use, and reports of negative, unwanted effects. Mean (±SD) personality score and age is given separately for the two well-being groups. Differences in personality traits and age between well-being groups were assessed by an independent samples t-test, whereas differences in groups regarding frequencies of gender, education, mental health disorders, and substance use were assessed via chi-squared tests.
In order to assess whether the likelihood of mood change after psychedelic use differed between respondents with low and normal well-being, binary logistic regression was used to calculate odds ratio (OR). To do this, two logistic regression analyses were run, one with positive mood change (yes, or no = their post-use mood stayed the same as pre-use) as the dependent variable, and the other with negative mood change as the dependent variable. For both analyses, the included predictor variables were group (binary; low or normal well-being) and the 5 (continuous) outcome variables of the personality questionnaire (Extraversion, Agreeableness, Conscientiousness, Neuroticism, and Openness to experience). The predictors were combined in each analysis, in order to control for potential confounding aspects between group and any of the personality traits. Importantly, interpretation of ORs differs according to whether the predictor is binary or continuous. When assessing a binary predictor, ORs can be interpreted as a measure of effect size. Whereas in regard to continuous variables, the OR is scale dependent and thus not able to be interpreted as a measure of effect size. Instead the OR is interpreted in terms of each unit increase on the scale.
Finally, a series of exploratory logistic regression analyses were run to assess whether set-specific characteristics, namely well-being scores and personality, were predictive of unwanted side effects. Predictor variables were the same as the mood change analyses, however dependent variables now consisted of reported side effects (yes or no) after LSD, psilocybin, MDMA, and ayahuasca, separately.
For each OR, 95% confidence intervals (CIs) were given and statistical significance was set at p ≤ .05. An OR of 1.5 is defined as small, 2 as medium, and 3 as large (Sullivan and Feinn, 2012).
Results
Demographic information
Total group demographic information and detailed substance use history have been reported elsewhere (Mason and Kuypers, 2018). Well-being scores indicated that 1324 (67.3%) respondents had an average (SD) well-being score of 67.9 (10.8) and were classified in the normal well-being group; and 643 (32.7%) respondents had an average (SD) well-being score of 35.47 (10.88) and were in the low well-being group.
Participant demographic information, per well-being group, can be found in Table 1. Analysis demonstrated that demographics of well-being groups differed statistically with low well-being groups consisting of a higher proportion of females, a lower amount of individuals with an advanced degree, a higher frequency of mental health disorders, and a lower use of MDMA and psilocybin use compared to the normal well-being group.
Demographic information for low vs normal well-being respondents that completed the study (N = 1967).

*Significant p values.
aχ2 test for frequency data; effect size = Cramer’s V.
bIndependent t-test; effect size = Cohen’s d.
Personality. Independent samples t-tests showed that respondents in the low well-being group reported lower scores on Extraversion (t(1965)=10.55, p < .001, d = 0.50), Agreeableness (t(1965) = 7.53, p < .001, d = 0.36), Conscientiousness (t(1965) = 10.31, p<.001, d = 0.50), and Openness to experience (t(1965)=2.157, p = .031, d = 0.10), and higher scores on Neuroticism (t(1965) = −17.66, p < .001, d = 0.84), compared to those in the normal well-being group (Figure 2).

Mean (%) scores of personality characteristics among normal well-being and low well-being respondents.
Setting: Environmental circumstances under which users take psychedelics
Setting details are presented in Figure 2. It is shown that, regardless of group, respondents reported usually using LSD (N = 1313; 83.9%) and psilocybin (N = 1159; 80.6%) in a “home” setting, MDMA in a “party” (N = 800; 70.98%) or “festival” (N = 692; 61.41%) setting, and ayahuasca in a “ceremonial or spiritual ritual” setting (N = 80; 52.63%) or “other” (N = 102; 67.11%) type of setting (Figure 3).

Mean percentage (%) of respondents’ reported setting of substance consumption, per psychedelic, in the entire sample (a), normal well-being sample (b), and low well-being sample (c).
Set: Emotional circumstances under which users take psychedelics
Set details are presented in Tables 2 and 3. It is shown that, regardless of well-being group, respondents reported most commonly using all the substances when in a positive mood.
Number (percentage) of respondents’ mood state prior to and after psychedelic consumption, in the total sample.

Respondents were asked what mood state they were in prior to substance consumption and if their mood changed after substance.
LSD: lysergic acid diethylamide; MDMA: methylenedioxymethamphetamine; +: positive mood state; −: negative mood state; 0: neutral mood state.
Number (percentage) of respondents’ mood state prior to and after psychedelic consumption, in the entire sample as well as in the normal well-being and low well-being samples.
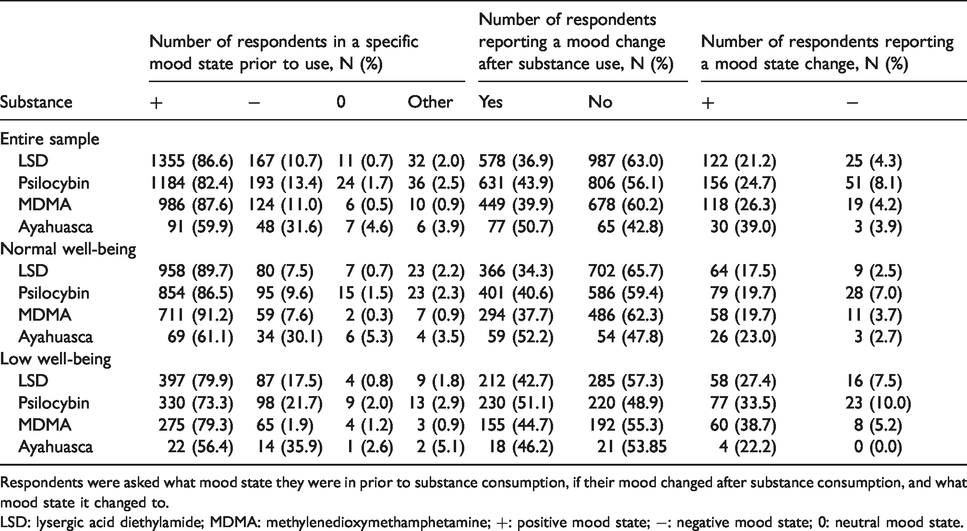
Respondents were asked what mood state they were in prior to substance consumption, if their mood changed after substance consumption, and what mood state it changed to.
LSD: lysergic acid diethylamide; MDMA: methylenedioxymethamphetamine; +: positive mood state; −: negative mood state; 0: neutral mood state.
Mood state
Substance-independent mood state
It was asked as to whether mood state changed after substance ingestion. Overall, it was found that around 60% of respondents did not experience a mood-state change after ingesting LSD and MDMA, whereas the percentage was around half (50%) for psilocybin and ayahuasca (Table 2).
Substance-dependent mood state
When mood state did change after substance ingestion, it was asked as to what mood state it changed to. Percentages of respondents who reported a positive or a negative mood change after substance use are displayed in Table 3.
Outcome of psychedelic use (mood) given set-specific characteristics
Well-being dependent positive mood state change
Logistic analysis demonstrated that the experiencing of a positive mood change after substance consumption was more likely in those with a low well-being score compared to those with a normal well-being, after taking LSD (b = 0.44, OR = 1.56; p = 0.036;[1.03, 2.37], psilocybin (b = 0.53, OR = 1.70; p = 0.01;[1.15, 2.47], and MDMA (b = 0.66, OR = 1.94; p = 0.003;[1.26, 2.98]). In contrast, a positive mood change was less likely in those with low well-being after ayahuasca consumption, compared to those with a normal well-being (b = −1.76, OR = .172; p = 0.008;[0.05, 0.63].
Well-being dependent negative mood state change
There were no significant differences between well-being groups regarding likelihood of a negative mood change (all p > 0.20).
Personality dependent positive mood state change
Further analysis demonstrated that when mood did change it was significantly more likely to experience a positive mood change after LSD (b = 0.01, OR = 1.01; p = 0.04;[1.00, 1.01]), psilocybin (b = 0.02, OR = 1.02; p < 0.001; [1.01, 1.02]), or ayahuasca (b = 0.02, OR = 1.02; p = 0.01; [1.01, 1.04] as scores in Neuroticism increased. Furthermore, it was significantly less likely to experience a positive mood change after psilocybin (b = −0.01, OR = 0.99; p = 0.014; [0.98, 0.99]) and LSD (b = −0.01, OR= 0.99; p = 0.02; [0.98, 0.99]) as scores in Openness to experience increased. Similarly, it was significantly less likely to experience a positive mood change after MDMA [b = −0.01, OR = 0.99; p = 0.02; [0.98, 0.99] as scores in Extraversion increased.
Personality dependent negative mood state change
A negative mood change was more likely after MDMA in those who scored higher in conscientiousness (b = 0.04, OR = 1.04; p = 0.02; [1.01, 1.08]) and less likely after ayahuasca in those who scored higher in agreeableness (b = −0.11, OR = 0.90; p = 0.04; [0.81, 0.99]).
Exploratory analyses: Unwanted effects given set-specific characteristics
Finally, it was assessed as to whether set-specific characteristics, namely well-being scores and personality, were predictive of unwanted effects.
Well-being and negative side effects
Analysis demonstrated that well-being score was not predictive of experiencing unwanted effects, regardless of substance (all p > 0.21).
Personality and negative side effects
Further analysis demonstrated that the likelihood of unwanted effects increased after taking LSD (b = 0.01, OR = 1.01; p < 0.001; [1.00, 1.01]), psilocybin (b = 0.01, OR = 1.01; p = 0.02; 95% CI[1.00, 1.01]), MDMA (b = 0.01, OR = 1.01; p = 0.02; [1.00, 1.01]), and ayahuasca (b = 0.02, OR = 1.02; p = 0.03; [1.00, 1.03]) as Neuroticism scores increased.
In addition, likelihood of unwanted effects also increased after taking psilocybin (b = 0.01, OR = 1.01; p = 0.04; [1.00, 1.01]) as Openness to experience scores increased. Contrarily, likelihood of unwanted effects decreased after taking psilocybin (b = −0.01, OR=.99; p = 0.001; [0.98, 0.99]) and MDMA (b = −0.01, OR=.99; p = 0.03; [0.98, 0.99]) as Agreeableness scores increased and the likelihood of unwanted effects decreased after taking ayahuasca (b = −0.02, OR=.98; p = 0.01; [0.96, 0.99]) as Extraversion scores increased.
Discussion
The present study sought to assess under which emotional (set) and environmental (setting) circumstances psychedelic users consume such substances. Utilizing a retrospective questionnaire, a self-selected sample of psychedelic users reported on the environment (setting) that they usually consumed such substances in and the mood state before and after use (set). It was further aimed to assess the emotional outcome of psychedelic use in those with clinical characteristics, defined as low psychological well-being and higher scores of neuroticism.
Although arguably well-known for years in both the psychedelic research, and subsequently the psychedelic using, community (Hartogsohn, 2017), to our knowledge this is the first study to systematically report on in which environmental setting users typically consume LSD, psilocybin, MDMA, and ayahuasca. Over 80% of respondents reported usually consuming the classic psychedelics LSD or psilocybin at home. This setting choice is in line with the approach of both historical and current-day psychedelic research, emphasizing a familiar, comfortable environment, often times mirroring a “living room” with a sofa, comfortable pillows, and decorations (Garcia-Romeu and Richards, 2018). Furthermore, approximately half of the respondents reported using ayahuasca in a ceremonial or spiritual ritual setting, or “other” type of setting, coinciding with both the historical and contemporary tradition of users to consume ayahuasca in these settings (Tupper, 2009). Importantly, although this questionnaire only inquired as to the typical environment in which participants consume psychedelic substances, it is in line with a previous report showing that specific aspects of the setting, including physical comfort, feeling of safety of the surroundings, and social support, play a role in the outcome of the psychedelic experience (Carbonaro et al., 2016). Together, these findings suggest that psychedelic substance users are cognizant of the potential impact of the environmental setting in which they take the classic psychedelic. MDMA, in contrast to the classic psychedelics, was usually used in the context of a festival or party, which is in accordance with users’ reported motives to consume MDMA, being mainly for hedonic and social reasons, a motive which is markedly different than that of classic psychedelics (Kettner et al., 2019).
Findings support previous research suggesting that psychedelic drug users are also aware of the role of mood (set) in the psychedelic experience (Shewan et al., 2000). Specifically, it was found that most respondents, regardless of substance or level of psychological well-being, use the substance when in a positive mood. Subsequently, most respondents also reported that mood did not change after use.
When mood did change after use, a positive mood change was more likely for those with low well-being, after taking LSD, psilocybin, or MDMA, whereas it was less likely after ayahuasca, compared to those with normal well-being. The finding of acute positive mood change after psychedelic use is in line with previous experimental research in both healthy and clinical populations (Bedi et al., 2010; Dolder et al., 2016; Gasser et al., 2015; Griffiths et al., 2006; Hasler et al., 2004; Kometer et al., 2012; van Wel et al., 2012; Vollenweider et al., 1998). However, the differentiation in mood effects based on well-being has yet to be investigated in placebo-controlled research. The higher likelihood of respondents with low well-being to experience a positive mood change could be due to the fact that those with low well-being will start off more frequently with a neutral or negative mood and thus have a potentially larger range to change after a psychedelic experience, than those with normal well-being (Haijen et al., 2018).
That being said, although previous research has highlighted the role of pre-administration mood state in predicting a response to a psychedelic (Metzner et al., 1965; Studerus et al., 2012), our findings suggest that mood may not be the most important aspect of an individual’s set when it comes to predicting their acute response to a psychedelic. Namely, it was found that nearly 100% of respondents who took any of the psychedelic substances in a negative mood state reported a mood change after use. Indeed, recent research suggests that other state set factors besides mood, like feelings of preparedness and readiness, and openness towards the experience, can predict a positive acute experience (Haijen et al., 2018; Studerus et al., 2012), whereas emotional excitability (Haijen et al., 2018; Metzner et al., 1965; Studerus et al., 2012) and apprehension (Leary et al., 1963) can contribute to a negative acute experience. Furthermore more complex set factors like intentions, expectations, and motives (Haijen et al., 2018; Metzner et al., 1965) also play a role in the outcome of the acute experience. In the current sample, main motivations to use LSD, psilocybin, and ayahuasca included to “broaden consciousness” and for a “spiritual experience” (Kettner et al., 2019). Thus, taking everything together, it is suggested that low mood state before the psychedelic experience does not per se induce a negative experience, while a combination of specific above-mentioned set factors potentially could. This is important as psychedelics are being investigated clinically in individuals characterized with negative mood (like depression and anxiety), and our findings support the idea that psychedelics are still a suitable therapeutic option. Additionally, it suggests that when preparing such individuals for a psychedelic experience, clinicians should focus on the other aforementioned set factors like preparedness and readiness for the experience, and expectations of the patient.
Findings demonstrated higher scores of neuroticism in respondents in the low well-being versus the normal well-being group. Neuroticism is a broad personality trait, associated with vulnerability to psychopathology and persistent negative mood (Clark et al., 1994; Costa and McCrae, 1980). Although previously assessed, research regarding the association between neuroticism scores and the psychedelic experience has been mixed. Specifically, one study found that, in individuals who previously had a negative response to a psychedelic, higher neuroticism scores correlated with the strength of the challenging experience (Barrett et al., 2017), whereas two other studies did not (Haijen et al., 2018; Studerus et al., 2012), however Studerus et al. (2012) actively screened out individuals scoring high (defined as greater than 2 standard deviations among the mean) in emotional lability, a construct related to neuroticism (Miller and Pilkonis, 2006). Nonetheless, our findings support the idea that trait neuroticism can be predictive of an individual’s response to a psychedelic. Specifically, it was found that as neuroticism scores increased, so did likelihood for experiencing a positive mood change after use of a classic psychedelic (LSD, psilocybin, or ayahuasca). Although indirectly, our findings are in line with previous studies which found positive mood change after administration of a classic psychedelic in patients with depression and anxiety (Carhart-Harris et al., 2016; Griffiths et al., 2016; Palhano-Fontes et al., 2018; Ross et al., 2016), clinical populations which are characterized by higher rates of neuroticism compared to the average population (Middeldorp et al., 2006; Saklofske et al., 1995). Taken together, our findings suggest that individuals who score high in neuroticism can use psychedelic substances with positive outcomes, and thus should not necessarily be excluded from controlled experimental trials, as has been done in the past (Hasler et al., 2004).
That being said, it was also assessed as to whether personality traits were predictive of experiencing unwanted effects after psychedelic use, and was shown that as ratings in neuroticism increased, so did the likelihood for experiencing unwanted effects after taking any of the psychedelic substances. Thus, as previously suggested (Barrett et al., 2017; Haijen et al., 2018) special consideration and attention could be given in preparing this population for a psychedelic experience. Specifically, considerations could include longer preparation time before and/or integration time after substance administration (Barrett et al., 2017). However, in order to incorporate this into practice, an additional screening measure for personality traits would have to be included upon participant enrollment. Nevertheless, it is important to note that, although the personality-dependent logistic regression analysis demonstrated statistically significant OR, and although ORs for continuous predictors cannot be interpreted as effect sizes, associations between some outcome variables were arguably small. It could therefore be argued that a weak association was made significant due to our relatively large sample size. Nonetheless, as findings are in line with previously discussed research, and are consistent in our data set across substances, they are suggestive as being valid findings.
The current cross-sectional, retrospective, self-report study is not without its limitations. Inherent limitations in this type of design include potential inaccuracies of reported answers (including, but not limited to, erroneous retrospective memory of drug experiences, and generalizability over multiple past experiences), as well as an inability to independently validate responses. Furthermore, as this survey was advertised on forums focusing on psychedelics, our sample is at risk for selection bias, as the population that had unwanted experiences with psychedelics may not be involved with such forums, and thus were not reached. Furthermore, the retrospective nature does not allow investigation into causality between set factors and respondents’ reaction to psychedelic use. Subsequently, two explanations are possible for the higher likelihood of positive mood change in the low well-being group; first those scoring lower in well-being and higher in neuroticism are more likely to experience mood change after substance use, second mood change after substance use leads to lower well-being and higher rates of neuroticism. However, current clinical studies investigating psychedelics as a therapeutic provide support for the former explanation. Specifically, administration of psilocybin has been found to induce long-lasting positive psychological changes, such as symptom remission and enhancement of well-being (Carhart-Harris et al., 2016; Griffiths et al., 2016; Johnson et al., 2017), and decrease neuroticism scores after treatment (Erritzoe et al., 2018). Finally, it is important to point out that our respondents were asked about their average experience with the substance. As it has previously been shown that one negative drug experience can have a greater, lasting impact than many positive experiences (Carbonaro et al., 2016), future studies should delineate between specific experiences.
In conclusion, the present study demonstrates awareness of recreational psychedelic users regarding the potential impact of set and setting on the psychedelic experience. Importantly, individuals with clinical characteristics, namely low psychological well-being and higher scores of neuroticism, report consuming such substances with positive outcomes.
Footnotes
Acknowledgements
The authors would like to thank the people who advertised this survey on their websites (https://www.reddit.com/, https://www.shroomery.org/, https://www.dhpforum.nl/forums/, and ![]() ), and all respondents for their time and effort, as well as all reviewers for their valuable input.
), and all respondents for their time and effort, as well as all reviewers for their valuable input.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.