
Abstract
Traumatic and iatrogenic cataracts may conceal occult capsular injury that routine slit-lamp examination and biometry fail to detect, increasing the risk of intraoperative complications. We present a mechanism-aware, imaging-guided approach to cataract surgery in an eye with suspected capsular compromise. An elderly man with a dense cataract and limited fundus view underwent preoperative imaging, which revealed a focal anterior capsular defect on ultrasound biomicroscopy, while posterior capsule integrity remained uncertain. His history included multiple intravitreal injections and prior anterior chamber paracentesis, raising suspicion for iatrogenic capsular injury. Given possible posterior fragility, surgery was performed using a noncontinuous curvilinear capsulotomy with radial relaxing incisions, low-vacuum and low-flow phacoemulsification, and contingency planning for capsular support and anterior vitrectomy. A monofocal intraocular lens was successfully implanted in the capsular bag without complication. This case highlights the importance of linking mechanism, targeted imaging (swept-source OCT or ultrasound biomicroscopy depending on media clarity), and a modified surgical strategy to reduce the risk of posterior capsule rupture and improve intraoperative preparedness.
Keywords
Introduction
Complex cataracts with suspected capsular compromise carry a heightened risk of intraoperative complications and suboptimal outcomes. While slit-lamp examination and routine biometry remain foundational, they may not reveal subtle capsular or zonular pathology, particularly in dense lenses or when the ocular history raises concern for iatrogenic injury. Ultrasound biomicroscopy (UBM) offers high-resolution anterior-segment imaging through opaque media and has been shown to delineate lens and capsular morphology, quantify lens opacity, and inform phacodynamics and case difficulty. 1 Traumatic cataracts frequently coexist with posterior segment injury and visualization challenges, underscoring the need for adjunct imaging and individualized planning. 2
Beyond classic trauma, iatrogenic injury (repeated intravitreal injections, prior anterior chamber (AC) paracentesis, or prior vitreoretinal surgery) is increasingly relevant. Meta-analyses report an association between prior intravitreal injection exposure and posterior capsule rupture (PCR) during cataract surgery; effect size appears to rise with larger cumulative injection numbers.3,4 This approach aligns with contemporary reviews that highlight controversies in surgical timing, visualization, and intraocular lens (IOL) strategy and advocate tailoring imaging and operative technique to mechanism, media clarity, and zonular status. 2
In this article, we connect mechanism to operative management. In the era of widespread intravitreal therapy, often accompanied by AC paracentesis to manage injection-related IOP spikes, cumulative intravitreal injections and prior paracentesis should heighten preoperative suspicion for capsular fragility and occult posterior capsule violation. Because such injury may be inapparent at the slit lamp, an imaging-guided workup and surgical approach tailored to clinical history is essential. The sections that follow synthesize current evidence and practical pearls and anchor this principle to a clinical vignette illustrating mechanism-driven planning in an injection-exposed eye.
Methods
This single-patient case report was prepared in accordance with the CARE guidelines for case reporting. Written informed consent for publication of clinical details and images was obtained from the patient; all data were de-identified in compliance with HIPAA and institutional policy. Clinical information was extracted from the electronic medical record and operative report, and imaging was reviewed by the authors. Because this is an individual case report, formal IRB review was not required under our institution’s policy.
To contextualize the case with recent evidence, we performed a focused narrative literature review (PubMed/Embase; January 2019 through October 2025; English-language, human studies). We prioritized comparative imaging studies (SS-OCT vs UBM/20-MHz), randomized trials, systematic reviews/meta-analyses, and high-quality narrative reviews relevant to traumatic/iatrogenic cataracts, intravitreal interventions, and AC paracentesis. No formal systematic review methods (registration, dual screening, risk-of-bias scoring) were applied given the narrative scope.
A challenging case
A man in his early 80s presented with progressive visual decline, most severe in the left eye, affecting daily function. Visual acuity was 20/150 in the right eye and counting fingers at 3 feet in the left eye. Intraocular pressures were 11 mmHg (right) and 12 mmHg (left). Slit-lamp examination showed 2+ nuclear sclerosis in the right eye. In the left eye, there was 3+ nuclear sclerosis with 4+ cortical changes, and fundus visualization was severely limited by lens opacity.
Given the density of the cataract and the limited posterior segment view, further imaging was obtained to evaluate capsular integrity and guide surgical planning. Preoperative 50-MHz UBM demonstrated a focal anterior capsular violation. Anterior segment OCT was performed but could not definitively confirm posterior capsule integrity (Figure 1).

(a) 50-MHz longitudinal (radial) ultrasound view of the left eye showing suspicious anterior capsular insult at 6 o’clock (red arrow) with adjacent zonular dehiscence. (b) Infrared image of AS-OCT showing localized cataract inferiorly (red arrow).
The patient had a history of exudative age-related macular degeneration requiring multiple intravitreal injections and had recently undergone AC paracentesis during pneumatic displacement of a submacular hemorrhage. In this context, the imaging findings raised concern that prior intraocular interventions may have contributed to occult capsular compromise. Because posterior capsule status remained uncertain, the surgical plan proceeded under the assumption of potential posterior fragility.
Surgical intervention
The patient underwent complex phacoemulsification with monofocal IOL implantation assuming posterior capsule compromise, favoring a noncontinuous curvilinear capsulotomy (can-opener technique) and low-stress nuclear disassembly. Intraoperatively, trypan blue staining enhanced visualization (Figure 2). A temporal, clear-corneal incision with a steel keratome was made. An inferior anterior capsule discontinuity was noted spanning 2 clock hours (6–8 o’clock). To mitigate radial tear extension, a can-opener capsulotomy was performed with multiple radial relaxing incisions to distribute tension on the capsular bag and avoid posterior extension of the tear. During phacoemulsification under low vacuum/low flow settings, the nucleus was carefully segmented and removed using a horizontal chop technique and aspiration to avoid zonulysis and tear extension. Phacoemulsification parameters were increased only after initial debulking to minimize capsular and zonular stress. Cortical material was carefully aspirated, and an intact posterior capsule with adequate zonular stability was confirmed. The capsular bag was successfully expanded, and the IOL was placed within the bag. Intracameral moxifloxacin was administered. No intraoperative complications occurred.

Intraoperative stills showing anterior capsular violation (red arrow) (a) prior to instillation of Trypan blue, (b) after instillation of Trypan blue, and (c) following modified capsulotomy with radial incisions.
Postoperative course
On postoperative day 1, the left eye showed 2+ corneal edema and mild AC reaction. Vision was 20/200. The patient reported good comfort and satisfaction with results, and was treated with intensified topical steroids, nonsteroidal anti-inflammatory drops, antibiotic drops, and hypertonic saline therapy. The IOL was centered and stable.
Discussion
Traumatic and iatrogenic cataracts can conceal capsular violations that slit-lamp/biometry miss; imaging often determines intraoperative preparedness and surgical outcomes. Surgeons should adopt a mechanism-aware approach to cataract surgery in an injection-exposed eye with prior AC paracentesis. Our challenging case illustrates this approach, where AC paracentesis and repeated intravitreal injections likely contributed to the focal anterior capsular violation. UBM identified the anterior capsule defect but could not definitively assess posterior capsule integrity; given the history (multiple IVIs and prior AC paracentesis) and dense lens, suspicion for occult posterior compromise remained high. Accordingly, a non-CCC capsulotomy with radial relaxing incisions and low-stress nuclear disassembly were used to minimize tear extension. Although causality cannot be established in a single case, the convergence of imaging findings and procedural history supports a high index of suspicion in similarly exposed eyes (Figure 3).
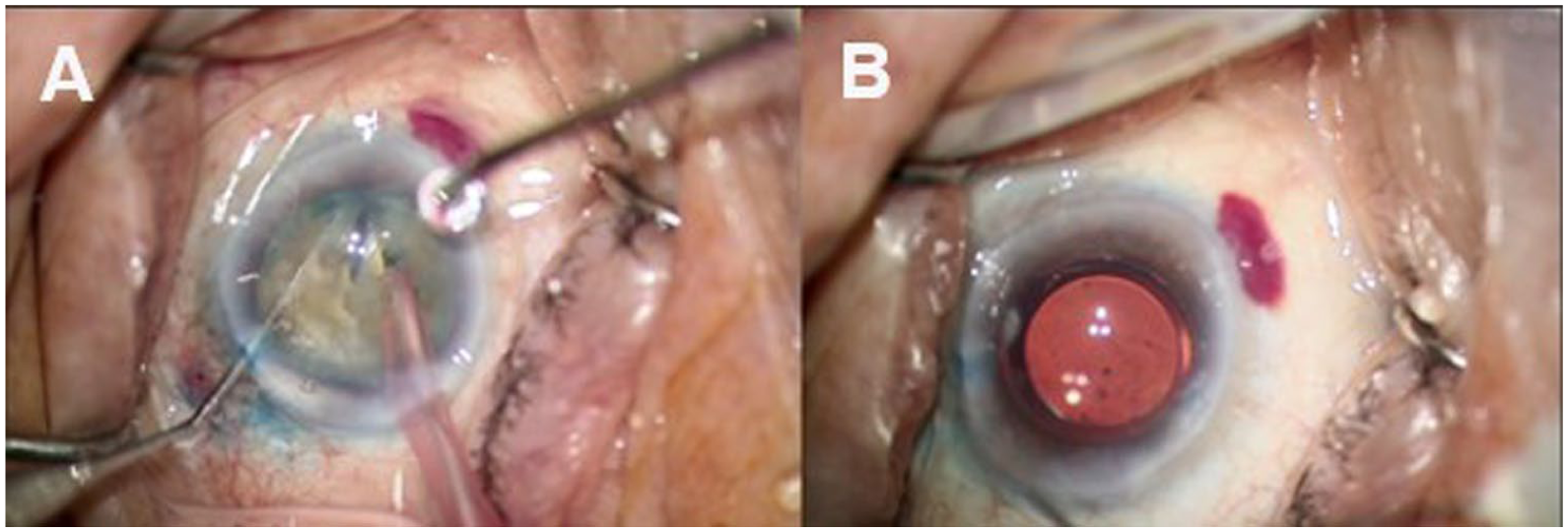
Intraoperative stills demonstrate (a) careful nuclear disassembly with horizontal phaco chop technique, and (b) completion of IOL placement in the capsular bag.
While AC paracentesis is generally considered safe, lens touch and anterior capsule violation are documented risks. 5 Prior intravitreal injections are increasingly recognized as an independent risk factor for PCR during cataract surgery, with supportive evidence from meta-analyses and large cohorts, and multiple reports of iatrogenic capsular/lens injury after injections.3,4,6,7
Role of imaging in preoperative evaluation
Importantly, preoperative imaging choices should reflect the suspected mechanism. In traumatic cataracts, SS-OCT can be at least comparable, and in some circumstances superior to UBM for detecting capsular defects, with higher sensitivity and overall accuracy observed in a comparative study of 67 eyes. 8 In the past, UBM has been shown to be capable of preoperatively detecting posterior capsule (PC) tears in traumatic cataracts, significantly influencing intraoperative preparedness. 9 More recently, a study showed that 25-MHz UBM provides quantitative assessment of lens opacity and correlates with phacoemulsification energy, further reinforcing its utility in surgical planning. 10
When optical access permits, SS-OCT can be at least comparable, and in some settings, superior to UBM for detecting posttraumatic capsule defects 8 ; in dense/intumescent lenses or with limited pupils, UBM’s through-opacity visualization remains advantageous for surgical planning. 10 In this context, preoperative UBM, prompted by history and slit-lamp suspicion, converted a nonspecific risk signal into an explicit plan, aiming to prevent propagation of capsular compromise and avoid intraoperative surprises.
Practical pearls for surgical management
Nuclear and cortex management should be explicitly low-stress. Begin with low vacuum and flow settings and reduced surge parameters; use small-segment or horizontal chop techniques within a central working zone to minimize stress on the posterior capsule. Re-up dispersive viscoelastic during irrigation/aspiration for endothelial and capsular protection, then reassess the bag (PC integrity, zonular stability) before IOL delivery.2,10
Plan capsular support according to the extent and location of zonular loss seen on UBM/20-MHz: use capsular hooks early when dialysis spans several clock hours; choose a capsular tension ring (CTR) for generalized laxity, and a capsular tension segment with scleral fixation when dialysis is focal but significant (more stabilizing than CTR alone for bag preservation). Keep anterior vitrectomy set-up ready (plus triamcinolone to highlight vitreous) and have a three-piece sulcus IOL with optic-capture option available when in-the-bag placement is unsafe. 2
Finally, contextualize any history of AC paracentesis. Around intravitreal injections and pneumatic displacement, AC paracentesis is used to mitigate acute IOP spikes but carries a low, real risk of lens touch/anterior capsule insult; in such eyes, it is prudent to screen for focal capsule injury and to proceed as if the capsule is fragile when uncertainty persists.8,11
Timing considerations
For truly traumatic cataracts after open-globe repair, a randomized trial suggests no major difference in 6-month vision or key complications between early (first week) and late (1–2 months) surgery; zonulysis may be higher when delayed, underscoring individualized timing guided by ocular status and visualization. 8
Limitations
This report describes a single patient and is therefore hypothesis-generating rather than definitive, limiting generalizability. Preoperative imaging identified an anterior capsule defect but could not confirm posterior capsule integrity, so the rationale for our modified technique rests partly on inference rather than incontrovertible preoperative proof. Interventions were not randomized; choices reflect one surgeon’s experience and local resources (i.e. UBM availability, capsular support devices), which may differ elsewhere. Follow-up is short and does not address longer-term outcomes such as IOL stability, visual recovery beyond the early postoperative period, or posterior capsular opacification. The accompanying literature review is narrative, English-language, and recent-years focused, introducing selection and publication bias. Finally, because the eye had multiple prior procedures (intravitreal injections and AC paracentesis), causal attribution of capsular injury to any single exposure remains uncertain.
Conclusion
Traumatic and iatrogenic cataracts, particularly in eyes with a history of intravitreal injections and/or AC paracentesis, can conceal capsular injury that standard preoperative evaluation may miss. A mechanism-aware, imaging-driven workflow reduces intraoperative surprises: use SS-OCT when optical media permit and UBM/20-MHz ultrasound when they do not or when zonular/capsular detail is required. If posterior capsule integrity remains uncertain, assume fragility and execute a non-CCC (can-opener) capsulotomy with radial relaxing incisions, paired with low-stress nuclear disassembly and a contingency-ready plan. This approach aligns surgical techniques with the underlying risk profile and enhances intraoperative preparedness.
Key points
Mechanism guides imaging: SS-OCT when optics permit; UBM/20-MHz when they do not or when zonular detail is needed.
Assume fragility when uncertain: Non-CCC capsulotomy with short radial relaxations; low-stress chop; reduced-surge I/A.
Risk contexts matter: Heavily injected eyes and those with prior AC paracentesis warrant targeted imaging and contingency readiness.
Footnotes
Ethical considerations
Our institution does not require ethical approval for reporting individual cases.
Author contributions
IO: writing – original draft, review/editing, data collection; MM: writing – review/editing; MS: writing – review/editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.