
Abstract
Venetoclax, a BCL-2 inhibitor used in chronic lymphocytic leukemia and acute myeloid leukemia, has been rarely associated with autoimmune hemolytic anemia, mostly in chronic lymphocytic leukemia. We report the first case of venetoclax-triggered autoimmune hemolytic anemia in acute myeloid leukemia secondary to chronic myelomonocytic leukemia. An 80-year-old man developed abrupt warm autoimmune hemolytic anemia 4 days after venetoclax initiation with azacitidine. Hemolysis resolved rapidly after venetoclax withdrawal and corticosteroid therapy. Rechallenge led to compensated hemolysis. This case supports venetoclax causality and highlights that autoimmune hemolytic anemia can occur beyond lymphoid malignancies. Clinicians should monitor for autoimmune cytopenias during venetoclax therapy, even in myeloid disorders.
Keywords
Introduction
Venetoclax is an oral BCL-2 inhibitor approved for the treatment of chronic lymphocytic leukemia (CLL) and acute myeloid leukemia (AML) in combination with hypomethylating agents. Its main toxicities include cytopenias, gastrointestinal events, and tumor lysis syndrome. Reports of venetoclax-triggered autoimmune hemolytic anemia (AIHA) have been almost exclusively described in CLL, a context in which underlying immune dysregulation is known to predispose patients to autoimmunity. This has led to the perception that AIHA in this setting may be primarily disease-related rather than drug-related. Pharmacovigilance data suggest that venetoclax-triggered AIHA could also occur in other hemopathies (prolymphocytic T-cell leukemia), but there are no published reports outside lymphoid malignancies. 1
Here, we report a case of venetoclax-triggered AIHA in a patient with AML secondary to chronic myelomonocytic leukemia (CMML), suggesting that this adverse event may represent a drug-class effect.
Timeline
April 15, 2023: Diagnosis of CMML. Favorable response to erythropoietin (EPO), routine outpatient follow-up.
June 12, 2024: AML transformation.
June 24, 2024: Start of treatment with azacitidine and venetoclax.
June 27, 2024: Onset of hemolytic anemia, venetoclax was withdrawn while azacitidine was continued.
June 28, 2024: Beginning of treatment with corticosteroids.
July 5, 2024: Decrease in corticosteroids.
July 11, 2024: End of corticosteroid treatment; second cycle of azacitidine and restart of venetoclax, with recurrence of chronic compensated hemolysis since. Continuation of treatments every month, and persistence of compensated hemolysis.
Narrative
An 80-year-old man with a history of CMML presented with AML transformation. He had received EPO with transient benefit. At AML progression, white blood cell count was 61 with 19 g/L monocytes. Bone marrow examination showed 16% blasts with monocytoid features, along with 10% monocytes and persistent dysmyelopoiesis. Karyotype was normal, with no 17p deletion.
Treatment with azacitidine and venetoclax (100 mg/day for 7 days) was initiated after rasburicase prophylaxis. No cases of AIHA have been reported in association with rasburicase or azacitidine, and no other treatment has been started recently.
Baseline hemoglobin was 11.4 g/dL. On day 4, the patient developed a sudden, dramatic drop in hemoglobin to 7.1 g/dL, with reticulocytosis (384 g/L), elevated LDH (lactate dehydrogenase: 3384 U/L), unconjugated hyperbilirubinemia (31 µmol/L), undetectable haptoglobin, and a positive direct antiglobulin test (IgG) (Table 1). White blood cell counts had decreased (leukocytes 28 g/L, monocytes 3 g/L), platelet counts were normal, and tumor lysis syndrome was controlled. These findings confirmed warm AIHA.
Summary of diagnostic tests and results.
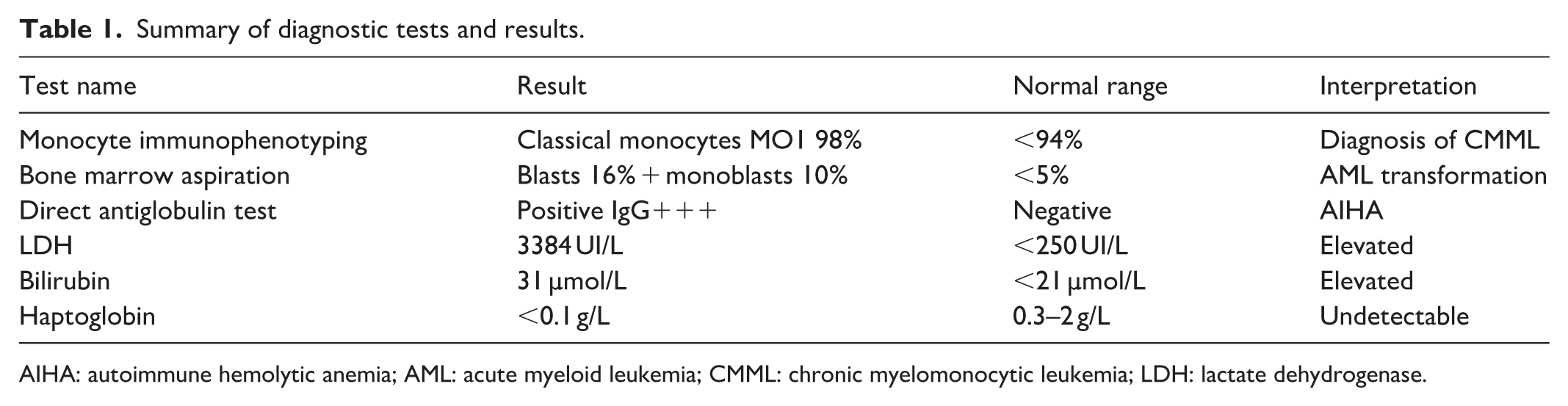
AIHA: autoimmune hemolytic anemia; AML: acute myeloid leukemia; CMML: chronic myelomonocytic leukemia; LDH: lactate dehydrogenase.
Venetoclax was withdrawn while azacitidine was continued, as venetoclax was considered the most likely causative agent after discussion with our clinical pharmacists. Rasburicase had been administered as a single dose and was already stopped. We had planned to stop azacitidine if there had not been a rapid improvement in hemolysis, which fortunately was not necessary. Corticosteroids (prednisone 1 mg/kg) were initiated, leading to rapid hematological recovery, allowing steroid taper after 7 days and cessation after 14 days.
The decision to re-administer venetoclax was carefully discussed in a multidisciplinary team meeting, weighing the benefit–risk balance. We also consulted our clinical pharmacists and reviewed pharmacovigilance data. Considering the rapid and favorable evolution of AIHA, the expected significant benefit of venetoclax, the absence of equally effective alternatives for this patient, and his request to continue treatment, we decided to resume venetoclax under close in-hospital daily monitoring of hemolysis parameters (complete blood count, reticulocytes, LDH, bilirubin, haptoglobin) to ensure patient safety. Corticosteroids and rituximab were considered; however, given the patient’s age and vulnerability to infections, and the absence of previously reported cases of AIHA under venetoclax in myeloid malignancies, our suspicion of a venetoclax-related AIHA was initially uncertain and these treatments were therefore not initiated.
During the next cycle, venetoclax was thus cautiously reintroduced in combination with azacitidine. We observed recurrence of hemolysis, but it remained moderate and compensated, without clinically significant consequences.
Treatment is pursued every month, with persistence of chronic compensated hemolysis ever since. The patient is being closely monitored for potential long-term risks of this compensated hemolysis, including thrombosis and renal impairment. Despite these risks, he is tolerating the treatment very well, does not require transfusions, and the benefit–risk balance remains favorable for this now 83-year-old patient.
Diagnostics
Patient perspective
The patient has confidence in the treatment and its management and tolerates venetoclax well.
He is proud that his experience is being shared. He continues to be followed regularly in the clinic and remains active in his personal life.
Discussion
This is one of the first reported cases of venetoclax-triggered AIHA outside of CLL, and the first in a myeloid malignancy. We acknowledge that the patient’s underlying CMML, a condition associated with a higher baseline risk of autoimmunity, represents an important confounding factor. Nevertheless, the chronology of events, absence of alternative triggers, and rapid resolution following drug withdrawal support a contributory role of venetoclax in the development of AIHA in this patient. The causative role of venetoclax was considered “probable/likely” according to the WHO–UMC criteria, and a “definite adverse drug reaction” (9/12) according to the Naranjo Adverse Drug Reaction Probability Scale, consistent with a scenario in which the drug precipitated an autoimmune reaction in a predisposed individual.
AIHA associated with hematologic malignancies
Autoimmune cytopenias are a common complication of CLL, which may predispose patients to such events; indeed, AIHA can occur in 10%–15% of CLL patients. The association between AIHA and myeloid pathologies (particularly CMML or AML) is less commonly recognized, even though some single-center studies report incidences of up to 20% in the case of CMML. 2 AIHA may be underreported in AML, as it can be attributed to disease progression, concurrent infections, or overlapping cytopenias due to myelosuppression.
Literature of venetoclax-triggered AIHA in CLL context
Several cases of venetoclax-triggered AIHA have been reported, almost exclusively in CLL patients3–5 (see Tables 2 and 3).
Case reports of venetoclax-triggered AIHA in CLL patients.

AIHA: autoimmune hemolytic anemia; CLL: chronic lymphocytic leukemia.
Case series of venetoclax-triggered AIHA in CLL patients.

AIHA: autoimmune hemolytic anemia; AML: acute myeloid leukemia; CLL: chronic lymphocytic leukemia.
These data suggest that venetoclax may predispose to AIHA in CLL, although this complication is not consistently observed across studies,11,12 and its incidence in myeloid hemopathies is not known.
Potential mechanisms of venetoclax-triggered AIHA
The mechanism by which venetoclax may contribute to AIHA remains incompletely understood. Emerging evidence suggests a central role of BCL-2, as it is essential for lymphocyte development and maintenance of peripheral tolerance. 13 Several studies have shown that BCL-2 inhibition can lead to an increase in regulatory T cells (Tregs), 14 but with reduced suppressive capacity, 15 potentially favoring autoimmunity. In addition, BCL-2 inhibition has been reported to enhance dendritic cell activation and anti-tumor immune responses, 16 potentially promoting an autoreactive immune environment.
The rapid onset of AIHA in our patient (4 days) suggests that underlying immune dysregulation from CMML, combined with transient disruption of tolerance by venetoclax, precipitated the autoimmune response.
The absence of reported AIHA cases with azacitidine monotherapy supports a contributory role of venetoclax. However, AIHA in this setting is likely venetoclax-triggered rather than purely venetoclax-induced, as venetoclax may unmask or exacerbate a pre-existing autoimmune predisposition (as seen in CLL but also in CMML 2 ).
While this may represent a class effect, data on immune-mediated adverse events with other BCL-2 family inhibitors remain limited, and further mechanistic studies are needed to clarify these observations.
Conclusion
Clinicians should be aware of this rare but potentially severe complication. Close monitoring for autoimmune hemolysis should be included in the safety surveillance of patients treated with venetoclax, especially as its indications expand. We could also suggest baseline autoimmune screening before starting venetoclax (e.g. direct Coombs test, autoimmune serology), particularly in patients with underlying autoimmune risk, such as patients with CLL, but also CMML. Early recognition of AIHA and prompt withdrawal of venetoclax, together with corticosteroids, allows rapid resolution. Rechallenge may be cautiously considered on a case-by-case basis.
Footnotes
Acknowledgements
We would like to thank the patient for his consent and the entire team for their care.
Ethical considerations
The study was conducted in accordance with Helsinki’s declaration. This case report adheres to the CARE guidelines.
Consent to participate
Informed oral and written consent was obtained from the patient prior to submission.
Author contributions
Conception and design: K.B., G.F. Collection and assembly of data: K.B., P.L., S.M., G.F. Manuscript – writing and editing: K.B., P.L., B.G., S.M., G.F.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.