
Abstract
Malignant tumours within the nipple-areola complex (NAC) should be considered when a non-healing, bleeding, or painful unilateral lesion persists. We report the unusual case of an 81-year-old male with prior melanoma and non-melanoma skin cancers who presented for a 1- to 2-year history of a painful lesion on the left nipple. On examination, there was a pink, crusted, tender, indurated papule within the left nipple without underlying breast masses or axillary lymphadenopathy. Histopathology revealed nodular basal cell carcinoma (BCC). The patient also had suspicious pulmonary nodules, which demonstrated metastatic melanoma. Unexpectedly, the BCC rapidly grew. It was ultimately treated with Mohs micrographic surgery. This case highlights the importance of maintaining a high index of suspicion for malignant tumours in atypical areas like the NAC, especially unexpected tumours such as BCC. Within the NAC, tumours may display more aggressive features, be misdiagnosed or undiagnosed until later stages, or inadequately treated.
Introduction
The unique tissues that make up the nipple-areola complex (NAC) allow for various cutaneous lesions to arise, including benign, inflammatory, and malignant. 1 Inflammatory manifestations, such as nipple dermatitis, can present as bilateral erythema with scaling, and when chronic, fissures may appear, leading to erosions.2,3 However, when a non-healing, bleeding, or painful unilateral lesion persists within the NAC, concern for malignancy should arise. Malignant tumours that can occur within the NAC or breast include, but are not limited to, Paget’s disease of the breast and invasive or inflammatory breast cancer.1,2 While basal cell carcinoma (BCC) is recognized as one of the most common skin cancers worldwide, it rarely presents on non-sun-exposed areas, especially the NAC.1,2,4 While BCCs commonly grow slowly over years, there is conflicting evidence that in certain anatomic sites, such as the NAC, BCCs may have potential for more aggressive growth characteristics.5–7 Recognition of this unusual location and subsequent treatment, especially with margin-controlled surgical techniques, is of the utmost importance. We present the atypical case of a BCC that presented as an eroded, painful papule with rapid growth on the NAC of a male.
Case report
An 81-year-old male, who was an active runner, presented for a 1- to 2-year history of a painful lesion on the left nipple, attributed to friction from his clothing. They had a past medical history of melanoma on the right back (T3b (2.05 mm, ulcerated)), N2a (2/15 sentinel lymph nodes positive), diagnosed over 10 years prior and treated with wide local excision. They also had a history of non-melanoma skin cancers, coronary artery disease, dyslipidaemia, osteoarthritis, and osteoporosis. Medications included omeprazole, atenolol, and atorvastatin. On examination, there was a pink, crusted, tender, indurated papule within the left nipple (Figure 1). There was no underlying breast mass or axillary lymphadenopathy. The clinical differential included Paget’s disease of the nipple as well as inflammatory conditions. Punch biopsy revealed nodular BCC (Figure 2(a)–(c)). Given the atypical location and need for tissue conservation, the patient was referred to Mohs micrographic surgery. Within approximately 3 months, the lesion had rapidly grown and developed more oedema and crusting (Figure 3(a)). During this time, the patient was worked up for suspicious pulmonary nodules, which demonstrated recurrent metastatic melanoma. He elected to delay Mohs micrographic surgery. Approximately 5 months later, on the day of his Mohs micrographic surgery, the BCC had further increased in size, now encompassing and obscuring the entire nipple. A second papule was identified on the superior portion of the areola (Figure 3(b)). The tumour was excised in two stages, and pathology revealed BCC with adenoid and nodular features. No perineural or lymphovascular invasion was identified. The patient was offered reconstruction with a C-V transposition flap to reconstruct the nipple, but instead, opted for a simple linear closure.

(a) & (b) Clinical images of both NACs, with a pink eroded papule within the left nipple.
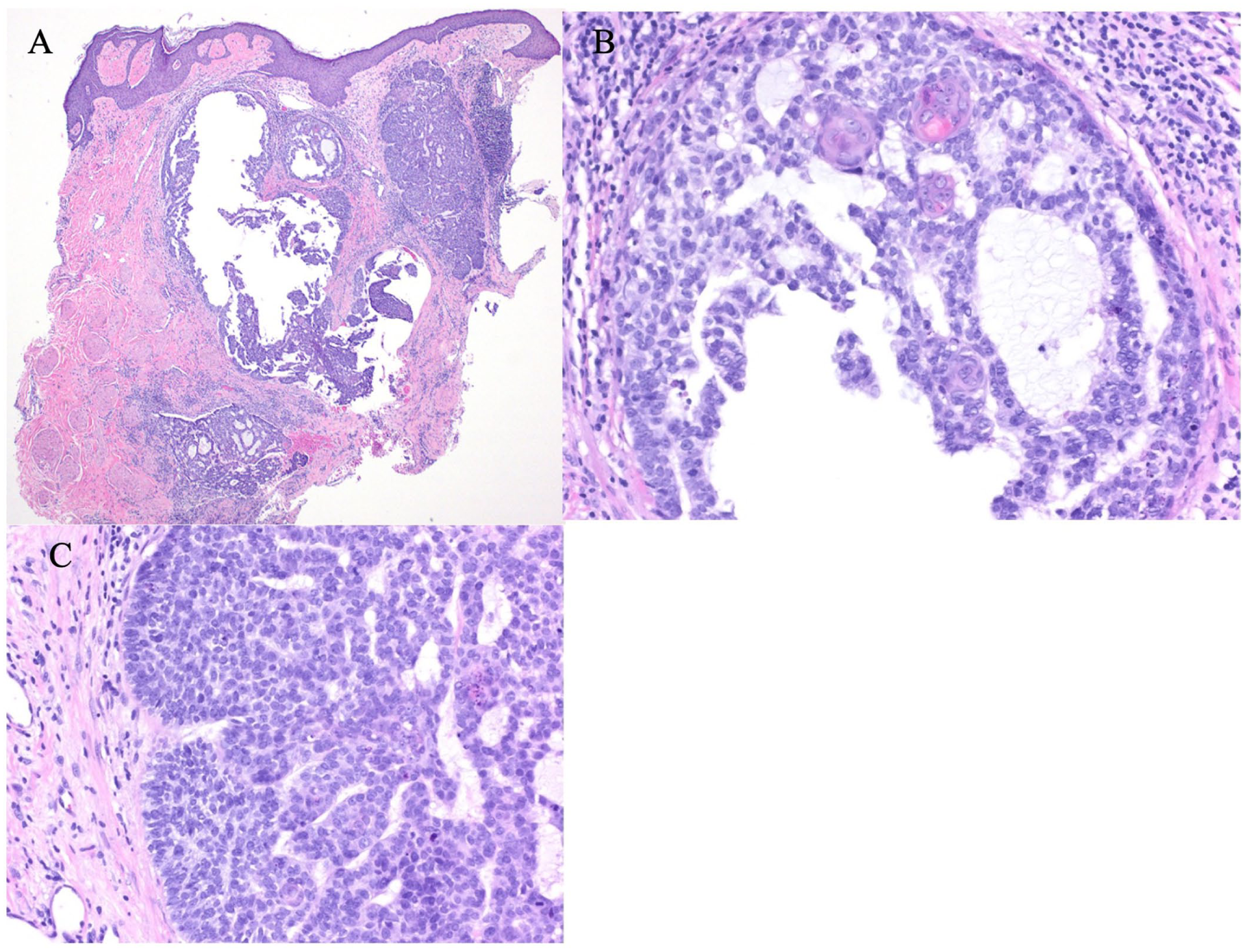
(a) 40×; H&E; Nodules of basaloid cells with a cribriform pattern, containing mucin with retraction artefact around the periphery. (b) 400×; H&E; nodule of mildly atypical basaloid cells with focal squamatisation, cribriform pattern, scattered mitotic cells, and fibrous, mildly inflamed stroma. (c) 400×; H&E; nodule of mildly atypical basaloid cells with a cribriform pattern, scattered mitotic cells, and a fibrous stroma.
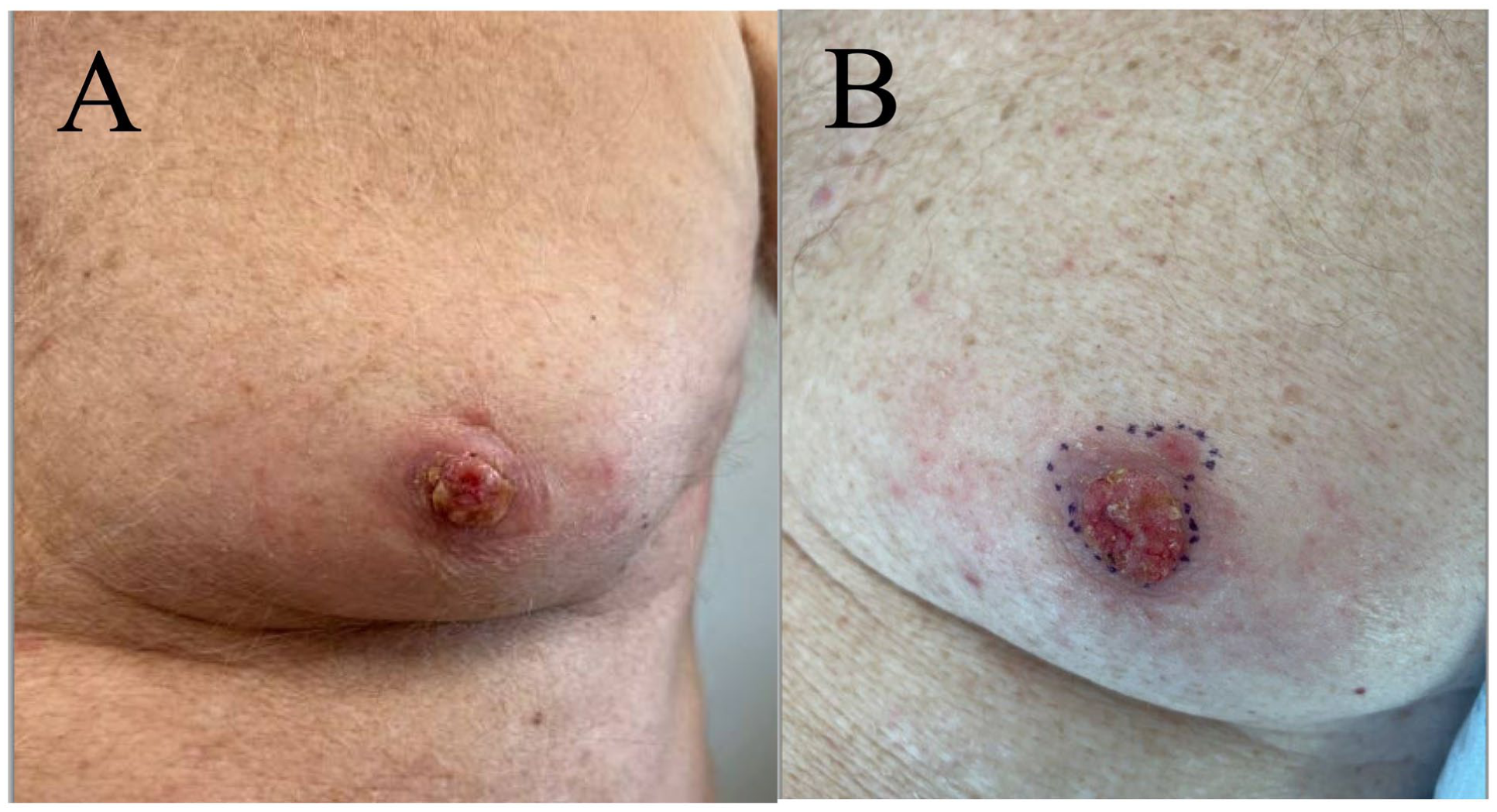
(a) Clinical image of BCC on the left nipple demonstrating progression in size approximately 3 months after initial consultation. (b) A pink ulcerated plaque encompasses the entire nipple with a second papule seen on the superior aspect of the NAC approximately 8 months after initial consultation.
Discussion
Chronic and intense intermittent sun exposure is a key etiological risk factor for BCC7,8 since it results in direct DNA damage from ultraviolet (UV) radiation. 8 Although the male NAC is more likely to encounter UV radiation compared to females, 3 20% of BCCs have been reported to arise on non-sun-exposed skin, which has been attributed to multiple factors, including ionizing radiation, arsenic exposure, immunosuppression, or genetic predisposition.8,9 This patient’s extensive history of skin cancer and unique location of his BCC raise the possibility of significant chronic sun exposure or an underlying genetic predisposition, both of which may confer a notable risk. Chronic friction to the nipple from rubbing of his shirt while running might have also played a role.
Up to 80% of BCCs are of nodular subtype, and typically present as slow-growing shiny, pearly papules or nodules with a smooth surface, rolled borders, and visible telangiectasias, and a tendency to bleed. 7 By contrast, NAC-BCCs have been described variably as ill-defined erythematous plaques with or without ulceration, erosion, scale, or crust.3,6,9 Thus, a wide differential should be considered when a lesion appears on the NAC, including contact dermatitis, erosive adenomatosis, Paget’s disease of the nipple, and inflammatory breast cancer.2,6 An increased incidence of NAC-BCCs has been reported in males, and have predominantly occurred in Caucasians, with the most common histologic subtype being nodular, and the onset age range from 35 to 86 years. 10 This patient’s presentation aligns with other previously reported cases of NAC-BCCs regarding gender, ethnicity, age, and histologic characteristics. Some studies have suggested NAC-BCCs have increased metastatic potential due to increased lymphatics of the NAC providing a direct route for tumour spread. 10 However, a global review reported only three cases with metastatic disease to the lymph nodes. 10 While metastatic BCC overall is extremely rare, less than 20% of patients with metastatic BCC survive longer than 1 year, underscoring the importance of establishing a diagnosis promptly. 5 High-risk BCC subtypes, such as infiltrative and micronodular, have been shown to grow at an approximate rate of 4.46 mm per year, whereas lower-risk subtypes, including nodular and superficial, grow approximately 1.06 mm per year. 4 Despite this patient’s lower-risk nodular subtype, his tumour size nearly doubled in approximately 8 months, which may be attributed to the NAC location or his underlying metastatic cancer. Tumour extent and the involvement of other anatomical structures guide management. Within the literature, treatment of NAC-BCCs has included medical therapy with topical 5-fluorouracil, laser therapy, radiotherapy, or surgery, including Mohs micrographic surgery or partial or simple mastectomy.9,10 Since treatment may have implications on functional and aesthetic outcomes, patient preference should be of high importance. 9 For tissue preservation, this patient’s tumour was treated with Mohs micrographic surgery.
This case highlights the importance of maintaining a high index of suspicion for BCC in atypical areas, especially the NAC, where it may display more aggressive features, be misdiagnosed or undiagnosed until later stages, or inadequately treated.
Footnotes
Consent to participate
The patient has provided informed written consent for the use of their photographs and medical information to be published.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.