
Abstract
Aggregatibacter aphrophilus, a fastidious Gram-negative member of the Haemophilus, Aggregatibacter, Cardiobacterium, Eikenella, and Kingella group, is an exceptionally rare cause of hepatic abscess, particularly in immunocompetent individuals. We describe a case of a healthy, middle-aged man who presented with a 5-day history of cyclical fevers, chills, and night sweats. Computed tomography imaging revealed a solitary hepatic lesion, initially suspicious for malignancy. Magnetic resonance cholangiopancreatography confirmed a hepatic abscess. Culture from a computed tomography-guided aspirate identified A. aphrophilus as the causative organism. Despite empiric broad-spectrum antibiotics and drainage, the patient continued to experience febrile episodes until culture-directed therapy led to clinical resolution. He received 3 weeks of intravenous ceftriaxone 2 g q24 h and PO metronidazole 500 mg q8 h and percutaneous drainage. Upon follow-up with infectious disease, no recurrence was noted upon review of repeat computed tomography imaging. This case highlights the importance of early microbiological identification and targeted treatment, even in healthy hosts.
Background
Pyogenic liver abscesses (PLAs) are uncommon but potentially life-threatening infections. Their annual incidence in Western countries is estimated to be 2.3 cases/100,000 people, with highly variable mortality rates depending on timely diagnosis and treatment. 1 Most cases are caused by enteric Gram-negative bacilli (such as Escherichia coli and Klebsiella pneumoniae) or anaerobic organisms, with biliary tract disease being the most common underlying pathology. 2 Although less common, amebic and fungal liver abscesses are often caused by Entamoeba histolytica and Aspergillus spp., respectively. 3 When considering liver abscesses and potential etiologies, the risk factors for pyogenic, amebic, and fungal abscesses vary. For example, PLAs are more commonly associated with males of older age with a history of uncontrolled diabetes, poor nutrition, and biliary infection. 3 Meanwhile, patients involved in travel to endemic areas or who are exposed to poor sanitation are at a greater risk of developing amebic abscesses. 3 With regard to fungal abscesses, these are most commonly associated with immunocompromised patients (i.e., patients with immunodeficiencies, undergoing chemotherapy for an associated malignancy, etc.) and rarely affect immunocompetent patients. 3 Potential complications of liver abscesses include shock if the abscess ruptures, liver failure, fistulas to nearby organs, or venous thrombosis. 4
As mentioned previously, the prognosis of liver abscesses is highly variable based on the patient’s history and the specific type of pathogen involved. Uncomplicated amebic and PLAs have a good prognosis with mortality rates (<3% for amebic, 2.5%–19% for bacterial) as there is a large range of antimicrobial therapies that target a broad range of organisms. 3 However, fungal liver abscesses, such as those caused by Aspergillus spp., have a much higher mortality rate of 38% and overall poorer prognosis. 3 This is largely due to the challenging immunocompromised patient population, delays in diagnosis based on patient presentation, or limited success in obtaining positive fungal cultures identifying a specific pathogen. To diagnose liver abscesses, the most common diagnostic tools used are abdominal computed tomography (CT) and ultrasound, as they are highly sensitive and help to identify the presence of solitary vs. multiple abscesses. 3 Generally, PLAs more often appear as multiples and bilobar compared to amebic abscesses that are often solitary, but this is also variable. 5
Aggregatibacter aphrophilus, previously known as Haemophilus aphrophilus, is a facultative anaerobic Gram-negative coccobacillus of the HACEK group (Haemophilus, Aggregatibacter, Cardiobacterium, Eikenella, Kingella), that is, more commonly associated with infective endocarditis. 3 Generally, patients who are most susceptible to this pathogen are immunocompromised and may have poor dentition, cardiovascular valve abnormalities, substance use disorders (alcohol, intravenous (IV) drugs), or tongue piercings. 6 Although uncommon, A. aphrophilus has been identified by individual case reports as the causative organism of abscesses of the brain, lungs, and liver due to hematogenous seeding. Its identification in an immunocompetent patient with no known risk factors is uncommon and diagnostically challenging.Therefore, this case report highlights our findings about the presentation and treatment of a PLA caused by A. aphrophilus in an immunocompetent individual.
Case presentation/differentials/treatment
A man in his late 50s presented to a tertiary center on the East Coast with a history of hypertension and spinal disc disease presented to the emergency room of a tertiary-level care hospital with a 5-day history of cyclical fever, chills, night sweats, fatigue, and non-bloody diarrhea. He reported no recent travel, sick contacts, abdominal trauma, dental procedures, or family history of liver, colon, or pancreatic cancer. He also denied any history of IV drug use, tobacco use, or alcohol use. Two days prior to his admission, he was seen by his primary care provider, who prescribed sulfamethoxazole/trimethoprim for a suspected urinary tract infection without improvement. His initial vital signs were unremarkable. The physical examination demonstrated no abdominal tenderness or distention without hepatosplenomegaly. Initial laboratory findings are outlined below and were significant for elevated liver enzymes (Table 1). Abdominal CT scan revealed a 4.2 × 4.3 × 5.3 cm heterogeneous mass of the right hepatic lobe (Figure 1). Labs were negative for hepatitis B (HBsAg, HBsAb, HBcAb) and hepatitis C (HCV Ab). Blood cultures were obtained to assess for common microorganisms of PLAs, and the patient was admitted for further evaluation and started on empiric IV piperacillin–tazobactam 4.5 mg q8 h. Differentials at this time included malignancies, such as primary liver cancers, lymphoma, hepatic necrotic cyst, or bacterial/fungal hepatic abscess due to cyclic fevers.
Pertinent laboratory values from admission to follow-up after discharge.

H: high/abnormal level; WBC: white blood cell count; Hgb: hemoglobin; ALT: alanine aminotransferase; AST: aspartate aminotransferase; ESR: erythrocyte sedimentation rate; CRP: C-reactive protein; BUN: blood urea nitrogen.

a) Coronal view of the abdominal CT. (b) Axial view of the abdominal CT. Both views of the abdominal CT obtained on admission revealed one 4.2 × 4.3 × 5.3 cm hypodense lesion at the right liver lobe (red circle). The lesion was large, multilocular, and heterogeneous with potential concern for malignancy due to adjacent perfusion abnormalities.
On the second day of admission, magnetic resonance cholangiopancreatography (MRCP) revealed a partially centrally necrotic/liquefied right liver lesion consistent with a hepatic abscess (Figure 2). Ultrasound (US) was not performed after MRCP identified the lesion as an abscess. Following these results, a CT-guided hepatic abscess drain was placed, and the sanguinous, purulent aspirate was collected and sent for culture. Meanwhile, the patient continued to have nightly fevers, sweats, and chills despite placement of a drain and continued antibiotic treatment. On the fifth day of admission, A. aphrophilus was isolated solely from the aspirate culture obtained from the abscess. In addition, all blood cultures and fungal aspirate cultures were negative.
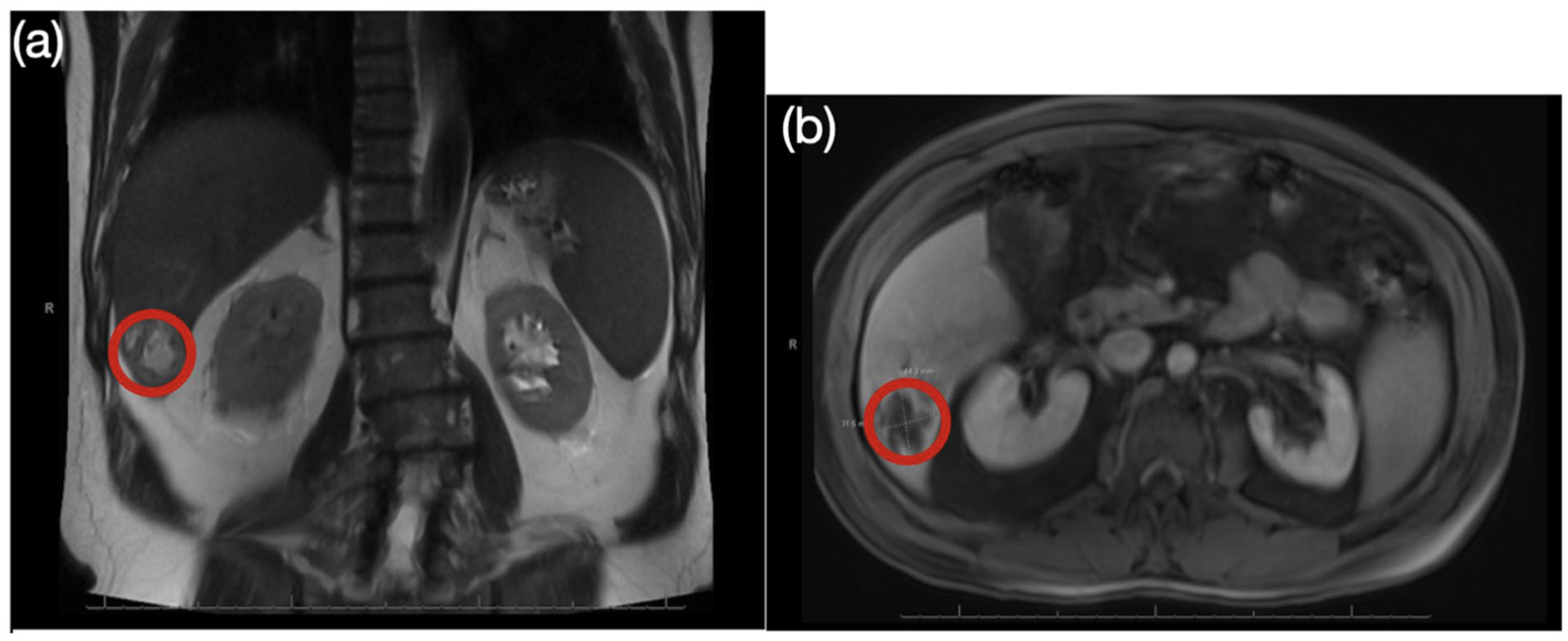
(a) Coronal view of the abdominal MRCP. (b) Axial view of the abdominal MRCP. Both views of the obtained MRCP revealed a 4.4 × 3.2 cm hypointense lesion in the liver parenchyma of the right lobe (red circle). The lesion had irregular borders with a low central signal, partial central necrosis, and adjacent edema within the liver parenchyma, consistent with a hepatic abscess.
Piperacillin–tazobactam was discontinued as Pseudomonas coverage was no longer needed. Antibiotic treatment was narrowed to IV ceftriaxone 2 g q24 h and PO metronidazole 500 mg q8 h as the dosing period of ceftriaxone was more feasible for home discharge planning compared to piperacillin–tazobactam. Additional labs and diagnostic studies were ordered, including E. histolytica IgG testing, E. histolytica DNA, CT Panorex, MRI of the lumbar spine with and without contrast, MRI of the brain with and without contrast, and a transthoracic echocardiogram (TTE) to determine the source of infection. The patient was negative for E. histolytica, and CT Panorex, MRI of the lumbar spine, and MRI of the brain were all negative for infection or additional abscesses. His TTE also showed normal left ventricular systolic function with an ejection fraction of 60%–65% with no valvular abnormalities. Therefore, no additional sources were identified outside the patient’s abscess as the cause for his infection. He clinically improved with the new antibiotic regimen and was discharged home with 2 more weeks of IV and oral antibiotic therapy and weekly lab draws (complete blood count (CBC) with differential and complete metabolic panel (CMP)). At his 2-week follow-up with the infectious disease, his symptoms had resolved. His antibiotic course and weekly labs were extended by 1 week as additional coverage while waiting for repeat CT imaging to be obtained the following week. Upon follow-up with emergency general surgery 3 weeks after being discharged, his drain was removed with no complications. No recurrence was appreciated based on improved labs and a repeat abdominal CT scan, and he made a full recovery, returning to work shortly after.
Discussion
A. aphrophilus is commonly associated with infective endocarditis, cerebral abscesses, and empyema, and is well documented as an endemic species of the oropharyngeal reservoir. In a recently published literature review, researchers found that 14 out of 20 patients with A. aphrophilus endocarditis had associated risk factors or underlying disease, including congenital heart disease, congenital valvular disease, poor dentition, chronic disease, or drug abuse; only six of 20 cases did not have risk factors present. 6 A. aphrophilus has been previously documented to cause brain abscesses likely caused by periodontal infection and recent dental procedures. 7 Its implication in hepatic abscess formation is exceedingly rare, with only seven cases reported. Only two of the seven cases published had other organ involvement; one case had a co-infection of the lungs, and the second case had a co-infection of the brain.8,9 All seven cases of liver abscesses found were in healthy and immunocompetent individuals. Two of the seven cases had a risk factor of dental surgery or manipulation, and one case had a recent history of trauma to the abdomen, as deemed a risk factor.9–11 What makes this case unique is that our patient had a solitary hepatic abscess, which has only been previously documented in one of seven cases; all other cases had evidence of two or more liver abscesses seen on imaging, and in this previously documented case with a solitary hepatic abscess, the patient had undergone a recent dental cleaning in Southeast Asia. To the best of our knowledge, this is the first known reported case of an A. aphrophilus solitary liver abscess in an immunocompetent patient with no underlying predisposing factors. Moreover, the cyclical nature of this patient’s fevers, which initially caused concern for malignancy, was unique, as the majority of cases described intermittent or remittent fevers. Upon discussion with the infectious disease team, possible sources could have stemmed from direct extension from a prior biliary or gastrointestinal infection or hematogenous seeding from a systemic circulation.12–14 Although the patient did not undergo any recent dental interventions prior to the development of this abscess, it is plausible that there could have been hematogenous seeding from transient oropharyngeal bacteremia, given the lack of trauma and common nature of exposure to this pathogen.
A. aphrophilus liver abscesses present a diagnostic challenge from a microbiologic and imaging standpoint. In previous case reports, four of the seven cases we found required 16S rRNA gene sequencing to diagnose the organism.8,9,10,15 As A. aphrophilus is a fastidious organism, it is difficult to culture, and it can be more easily identified when exposed to carbon dioxide or enriched blood culture medium. 16 However, once an aspirate was obtained from the liver abscess, his cultures grew A. aphrophilus. Our patient was initially told his liver lesion was most likely cancer. Malignant liver lesions can often mimic PLA as they can present with similar symptoms of fever, abdominal pain, chills, rigors, and anorexia. 17 When comparing the appearance of A. aphrophilus-associated liver abscesses to other types of liver abscesses, they present similarly to other types of PLAs on imaging. On abdominal CT, they tend to be hypodense and multilocular while having mixed echogenicity on abdominal US. 11 When comparing PLAs to other types of abscesses, the main differences are that pyogenic abscesses tend to aggregate into one large, localized area containing multiple, hypodense lesions, while amebic abscesses tend to present as solitary. 18 This appearance resembles the one depicted in Figure 1. A. aphrophilus-associated abscesses are also known to mimic tumors in appearance. For example, one study discussed how a large, left knee A. aphrophilus-associated abscess was initially thought to be a soft tissue tumor due to its appearance as an enhancing, heterogeneous mass with peripheral enhancement and inflammation on MRI. 19 Similar to how our patient case’s diagnosis was determined, the differentiation between malignancy versus abscess discussed within that study was determined by needle biopsy, culture samples, and repeat imaging showing improvement of the mass. 18 Therefore, based on these studies and our patient case, MRI can be helpful in further differentiating between abscesses and malignancy when CT and US are less clear, though biopsy or aspiration with cultures are key in confirming the diagnosis.
A review of reported cases of A. aphrophilus-associated liver abscesses (Table 2) reveals a consistently favorable prognosis when appropriate drainage and antibiotics are administered. The antibiotic regimen usually included 4–6 weeks of IV antibiotics, specifically third-generation cephalosporins, due to their easier dosing for patients who were discharged home with continued therapy and their tissue penetration for the central nervous system if brain abscesses were present. Upon review, patients who developed primarily hepatic and pulmonary abscesses fully recovered within 5–6 weeks of treatment, which was similar to our patient who recovered within 4–5 weeks, indicating a positive prognosis. However, those who presented with or developed additional brain abscesses sometimes required more than 6 weeks of treatment if they had additional complicating factors, such as a patent foramen ovale (PFO) that allowed the bacteria to spread via systemic circulation. Upon reviewing these cases, it is difficult to discern if there is a significant difference in mortality specifically between other types of liver abscesses and A. aphrophilus-associated liver abscesses, as the patients discussed recovered.
Additional case reports focused specifically on hepatic abscesses caused by Aggregatibacter aphrophilus.

IV: intravenous; CMP: complete metabolic panel; CBC: complete blood cell count; US: ultrasound; PFO: patent foramen ovale; MALDI-TOF: matrix-assisted laser desorption/ionization time-of-flight mass spectrometry.
Further review of previously reported cases, most patients were male and primarily in their 30s and 40s. In addition, there was only one reported case of a patient with a solitary hepatic abscess, like our patient. The majority of cases had multiple abscesses in the liver rather than a solitary hepatic region. However, the underlying source is often undetermined. This emphasizes the importance of maintaining a broad differential diagnosis and considering atypical pathogens, especially when standard treatments fail.
Finally, this case underscores the value of a multidisciplinary approach. Collaboration among infectious disease specialists, interventional radiologists, hepatologists, and microbiologists facilitates timely diagnosis, effective treatment, and optimal outcomes.
Conclusion
In summary, this case highlights A. aphrophilus as a rare, potential etiology for PLA in young, immunocompetent patients, especially when standard empiric regimens are ineffective. Moreover, CT imaging of hepatic abscesses may mimic neoplastic lesions; therefore, additional workup involving MRCP and image-guided aspiration can aid in differentiation and antimicrobial treatment. By promoting awareness about A. aphrophilus as a potential cause for abscesses in healthy individuals, this aids in preventing delays in diagnosis and improving treatment management.
Patient perspective
“The worst part was the extreme chills and fevers I had before the hospital, and I think that was the hardest part of the ordeal in general. That experience taught me a lot about patience, that’s for sure. When I was in the hospital on the first night in the emergency room, and they took the scans, they came back saying they found a mass on my liver. The doctor said every mass they’ve seen like this was always cancer, and they were thinking about sending me home to sort things out with outpatient doctors. At that time, my blood pressure dropped so low, they ended up admitting me. I remember two doctors coming in to tell me they didn’t think it was cancer and that it looked like an infection. It was really frustrating waiting on the second day for the scan to wait for the difference between whether it was a mass or an infection, and then waiting again for the next steps about needing a drain. After the drain was placed, I felt a lot better. When I went home after my 8 days in the hospital, it helped that my wife was a nurse since she helped with flushing the drains and giving me the IV antibiotics. The experience was one that was like no other for me, and it was strange because I didn’t know what caused it. We never really found out. When I followed up with the doctors for the drain and the antibiotics, they suggested I take another week of antibiotics. I used all my vacation time to take off work to recover at that time, and I actually went out of state after that appointment to visit my daughter. While we were traveling, we would stop at restaurants where my wife would pump the antibiotics for me. I think the treatment wasn’t as hard for me to deal with because my wife knew how to do everything, and I was grateful for that. After the drain was removed and I finished the antibiotics, I eventually went back to work about a month after I was originally sick. Since then, I feel great now, and I’ve completely healed up! I’m grateful for all the doctors who helped me get better and that everything worked out.”
Footnotes
Acknowledgements
We thank the Department of Internal Medicine at Penn State Health for giving us the opportunity to conduct this work.
Ethical considerations
Penn State Ethics Committee does not require ethical approval for reporting individual cases.
Consent for publication
Written informed consent was obtained from the patient for their anonymized information, including the case and its relevant images, to be published in this article.
Author contributions
Angela Tran: manuscript writing, clinical care, literature review. Evelyn Marin: manuscript writing, clinical care, literature review. Ahmad Matarneh: manuscript writing, clinical care, literature review. Joshua Zent: manuscript writing, clinical care. Zarish Umar: manuscript writing, clinical care. Kunal Desai: manuscript writing, clinical care.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting the findings of this study are available on request from the corresponding author.