
Abstract
Pacemaker lead infections with large vegetation and extensive adhesions pose significant procedural risks during surgical extraction. A 71-year-old woman with a 21-year-old pacemaker developed recurrent Staphylococcus aureus bacteremia. She underwent successful surgical lead extraction performed under cardiopulmonary bypass, with concomitant tricuspid valve repair, due to the presence of a large vegetation and strong adhesions to the right ventricular myocardium and tricuspid valve. Surgical lead extraction under cardiopulmonary bypass should be considered a viable option in patients with long-standing pacemaker lead implantation or large vegetation to reduce the risk of life-threatening complications.
Introduction
Pacemaker lead infections are generally treated by transvenous lead extraction (TLE). However, cases with extensive adhesions or large vegetations may necessitate surgical extraction.1,2 Such cases are associated with an increased risk of serious complications during TLE, such as cardiac tamponade and valve damage, which may result in fatal outcomes. Here, we report on the case of successful surgical lead removal under cardiopulmonary bypass with tricuspid valve repair in a patient with long-standing pacemaker infection.
Case study
A 71-year-old woman with a dual-chamber pacemaker for complete atrioventricular block, implanted 21 years prior, was hospitalized three times within the past year for bacteremia caused by methicillin-sensitive Staphylococcus aureus. Each time, her symptoms improved with intravenous cefazolin. She had also been receiving long-term oral prednisolone therapy for rheumatoid arthritis, which was diagnosed 10 years ago.
During her third hospitalization, transthoracic and transesophageal echocardiography and contrast-enhanced computed tomography revealed no signs of active infection. The patient was discharged and prescribed oral trimethoprim-sulfamethoxazole and rifampicin. Approximately 2 months later, she was readmitted with fever (38.1°C) and chills unresponsive to the oral antibiotic regimen. The physical examination was unremarkable.
Electrocardiography revealed sinus rhythm at 68 bpm without pacing activity (Figure 1). Laboratory tests showed elevated white blood cell count (13.9 × 10³/μL), C-reactive protein (6.12 mg/dL), and 82.1% neutrophils; the remaining results were normal. Blood cultures were positive for methicillin-sensitive S. aureus on two occasions. Intravenous cefazolin (2 g every 8 h) was initiated. Chest radiography revealed pleural effusion without lead displacement (Figure 2).
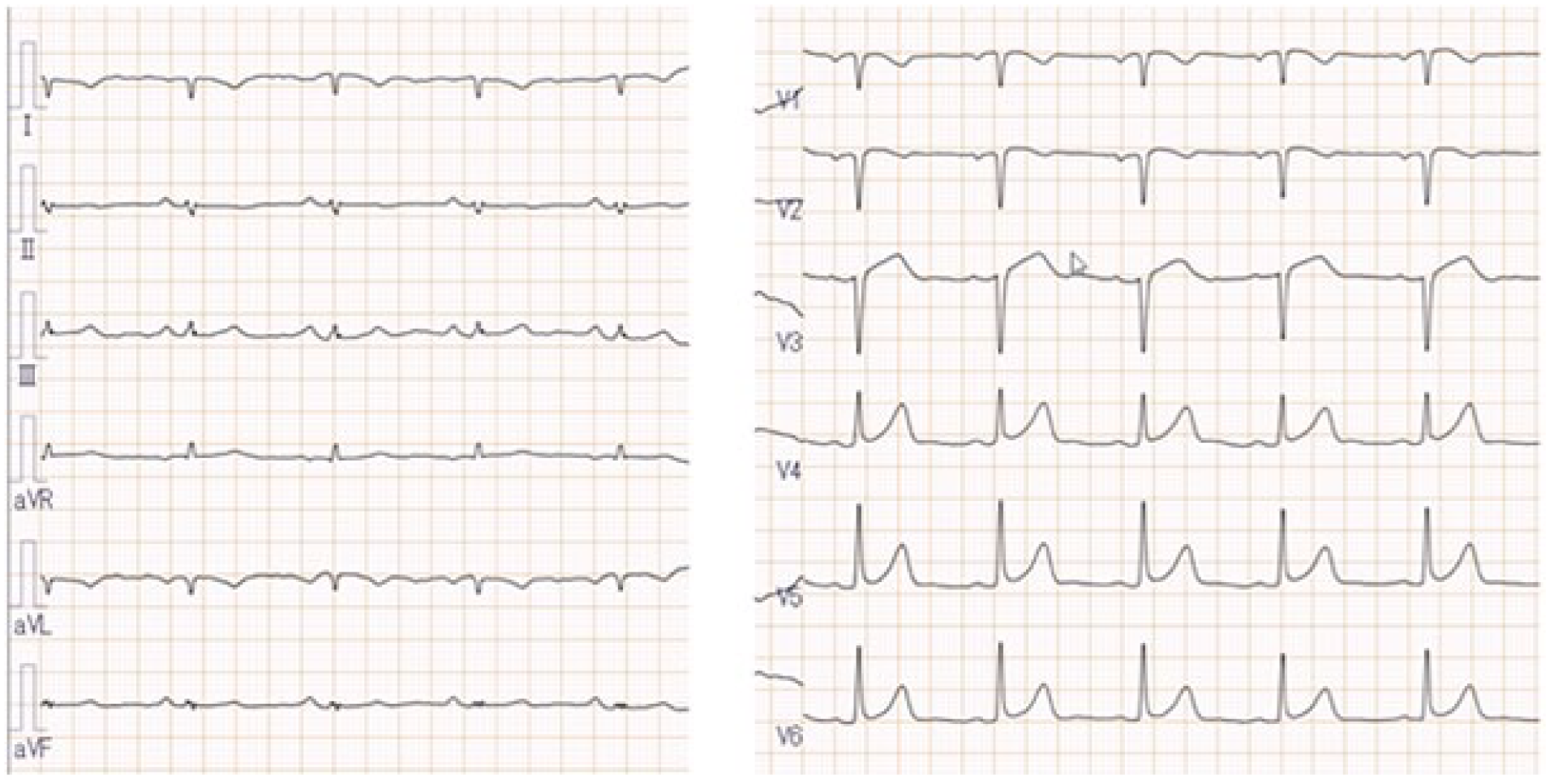
Electrocardiography shows sinus rhythm at 68 bpm without evidence of pacing activity.

Chest radiography demonstrates pleural effusion without evidence of lead displacement.
Transthoracic echocardiogram revealed two vegetations—22.7 × 7 mm near the tricuspid valve and 13.6 × 8 mm in the right atrium—adherent to the ventricular pacing leads (Figure 3(a) and (b)).
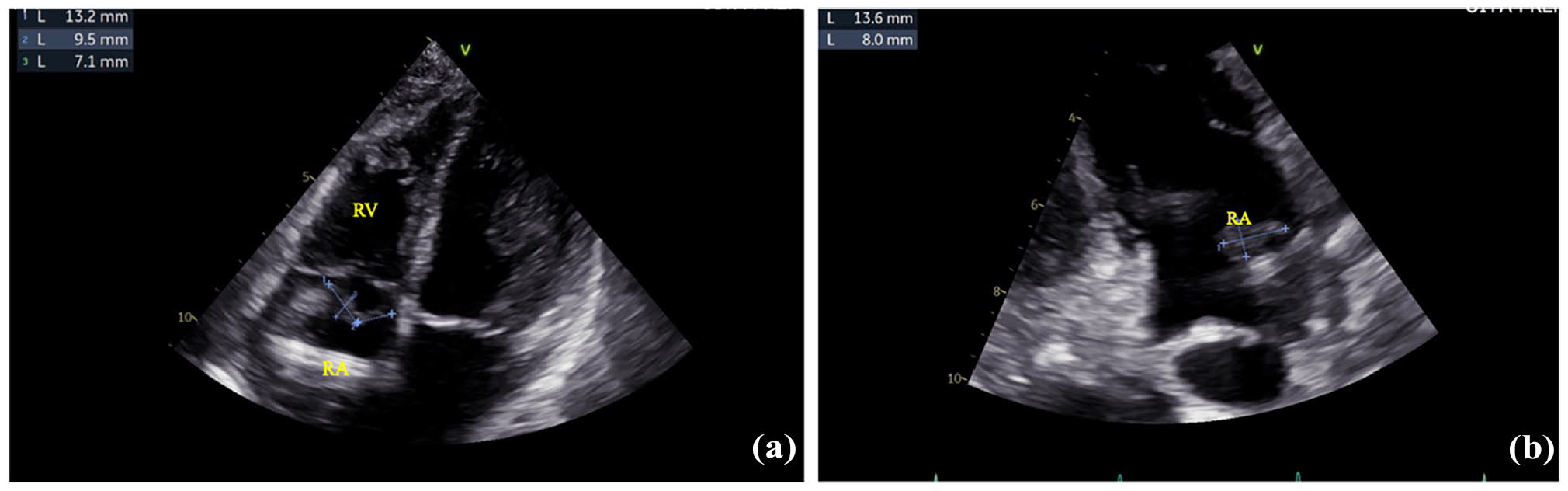
Preoperative transthoracic echocardiography showing two large vegetations: (a) A 22.7 × 7 mm mass adjacent to the tricuspid valve. (b) A 13.6 × 8 mm mass in the right atrium.
We opted for open-heart surgery because of the long-standing leads and large vegetation. Median sternotomy was performed, and the lead was removed under cardiopulmonary bypass. Intraoperatively, a large vegetation strongly adhering to the septal leaflet of the tricuspid valve and right ventricular myocardium surrounded the ventricular lead (Figure 4(a)). The lead was dissected and extracted using an 11th scalpel blade (Figure 4(b)). The tear in the septal leaflet was repaired using 5-0 polypropylene sutures (Figure 4(c)).

Intraoperative photographs: (a) The ventricular lead is strongly adhered to the septal leaflet of the tricuspid valve and the right ventricular myocardium (upper yellow arrow). A large vegetation is also observed in the right atrium (lower yellow arrow). (b) The lead is dissected and extracted using an 11th scalpel blade from the tricuspid valve and right ventricular myocardium. (c) The septal leaflet of the tricuspid valve is repaired using two 5-0 polypropylene sutures.
Cultures from the lead and vegetation confirmed methicillin-sensitive S. aureus infection. Intravenous cefazolin was administered. The patient’s postoperative course has been uneventful at 1 month, and she remains hospitalized under close observation. A new pacemaker was implanted once the inflammation subsided.
Discussion
Here, we present the case of a patient with a long-standing pacemaker lead infection and large vegetations who required surgical lead extraction under cardiopulmonary bypass with tricuspid valve repair.
Infection following pacemaker implantation is relatively uncommon, with an incidence rate of 0%–19%.3,4 However, sepsis or infective endocarditis increases the mortality rate, ranging between 12.5% and 25%.3,5
Major complications, such as cardiac tamponade, valve damage, and hemothorax, have been reported in 0%–3.5% of TLE procedures.2,6 The outcomes of such complications can be severe. U.S. Food and Drug Administration data (2007–2008) showed a 44% mortality rate among 62 patients who required emergency surgery for myocardial perforation or venous laceration after lead extraction. 7 Further, a 75% mortality was reported among four patients who required emergent surgery following 112 laser-assisted extractions. These findings underscore the significant risk of fatal complications and the importance of careful procedural selection. 2 Risk factors for such complications include longer lead implant duration (>6 years), female sex, corticosteroid use, and nonelective scheduled extraction,1,7 several of which were present in our patient.
When extensive adhesions are present in the right ventricular myocardium or tricuspid valve, or when vegetations exceed 20 mm, TLE carries a high risk of right ventricular perforation or severe tricuspid regurgitation. In such cases, open surgical removal without TLE is recommended.2,6 Despite being more invasive, lead extraction using cardiopulmonary bypass is considered a safe and reliable method. Furthermore, surgical intervention has shown high success rates even in older or hemodynamically unstable patients. 4
In our patient, the pacemaker leads had been in place for 21 years and were firmly adhered to the septal leaflets of the tricuspid valve and right ventricular myocardium. Transvenous removal would risk tricuspid valve or right ventricular injury; thus, surgical extraction under cardiopulmonary bypass was performed. This approach enables precise dissection and valve repair, likely preventing regurgitation and structural damage. While TLE is generally considered the initial strategy for managing pacemaker lead infections, upfront surgical extraction is sometimes preferred in high-risk cases. In one study involving 42 patients, surgical removal was chosen as the primary approach for 4 patients (9.5%) because of factors such as lead adherence, valve involvement, or concerns regarding procedural complications. 4 In the present case, the patient’s long-standing lead, large vegetation, and tricuspid valve adherence justified our selection of surgical intervention as the initial management strategy.
Conclusion
Surgical lead extraction under cardiopulmonary bypass is a recommended approach in cases involving long-standing pacemaker leads or large vegetations, particularly when conventional transvenous extraction may pose life-threatening risks.
Footnotes
Author Contributions
All authors made substantial contributions to the conception and design of the study, were involved in drafting the manuscript and revising it critically for important intellectual content, and approved the final version to be published.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.