
Abstract
Bouveret syndrome is a rare complication of gallstone ileus with a high mortality rate. It is defined as the migration of a large gallstone through a cholecystoduodenal fistula leading to gastric outlet obstruction. During this case, gastroenterology was urgently paged to the operating room during an elective cholecystectomy in a 61-year-old female when a large gallstone was found in a fistula. Subsequently, mechanical lithotripsy and basket removal of the stone were performed. This case highlights the importance of swift diagnosis and utility of less-invasive endoscopy procedures for treatment of Bouveret syndrome.
Keywords
Introduction
Bouveret syndrome (BS) is a rare complication of gallstones that can cause gastric outlet obstruction. It occurs in 0.3% to 0.5% of cases of cholelithiasis and is caused by the protrusion of a large gallstone with impaction in the proximal duodenum or pylorus. 1 BS carries a high mortality rate of up to 30% due to the elderly being more commonly affected and non-specific symptoms delaying diagnosis. 1 Additionally, there are no immediate guidelines on the management of BS due to the complex nature and rarity of this pathology. Generally, diagnosis is made through abdominal ultrasound and computed tomography (CT), while treatment is with surgery, though a few case reports exist that describe successful endoscopic therapy.2,3 We present a case of a 61-year-old female who was diagnosed with cholecystitis but was intraoperatively found to have a large gallstone in the duodenal bulb.
Case description
A 61-year-old Caucasian female with a past medical history of chronic cholecystitis and cholecystostomy tube placement was seen in a general surgery clinic after a right upper quadrant ultrasound demonstrated a contracted gallbladder, multiple gallstones, and a common bile duct measuring 1.2 cm. Her most recent labs demonstrate ALT (15 U/L), AST (22 U/L), ALP (131 U/L), total bilirubin (0.40 mg/dL), albumin (3.7 g/dL), hemoglobin (10.8 g/dL), and MCV (86.5 fl). The patient then had an MRI abdomen which revealed acute cholecystitis with a contracted gallbladder containing a 2.7 cm gallstone, some pericholecystic fat stranding, dilatation of the common bile duct measuring 13 mm, as well as dilatation of the extrahepatic biliary tree but without evidence of choledocholithiasis or pancreatic mass. The patient had complaints of nausea and dyspepsia, and it was decided to proceed with laparoscopic cholecystectomy with intraoperative cholangiogram.
The patient underwent a laparoscopic cholecystectomy which was aborted due to extensive lysis of adhesions of the gallbladder and duodenum. The patient then elected to opt for an exploratory laparotomy with esophagogastroduodenoscopy (EGD). During the surgery, the patient was found to have dense adhesions holding the transverse colon, mesocolon, and duodenum to the subhepatic area, and a hard and irregular 2.5cm firm mass behind the distal gastric antrum (Figure 1). Due to concerns of colonic and duodenal injury, cholecystectomy was not attempted. Gastroenterology was urgently called to perform an intraoperative EGD demonstrating a large, dark irregular mass consistent with a gallstone seen distal to the pylorus. The stone appeared to be stuck against the wall of the duodenal bulb, suggesting a cholecystoduodenal fistula with extrusion of the gallstone. Initially, mechanical lithotripsy was attempted but was aborted because the stone was too firm. Mechanical lithotripsy was performed multiple times to fragment the gallstone with sequential stone removal with a basket which was retracted into the stomach (Figure 2(a) and (b)). Her recovery was complicated by acute hypoxic respiratory failure secondary to lung atelectasis. Otherwise, the patient recovered well and was discharged on post-op Day 6 with supplemental oxygen.

Esophagogastroduodenoscopy visualizing a large gallstone seen distal to the pylorus protruding from a fistula.

(a and b) Mechanical lithotripsy being performed to fragment the large gallstone.
Discussion
BS is a rare form of gallstone ileus and is defined as a gastric outlet obstruction caused by the migration of a large gallstone through a cholecystoduodenal fistula. BS carries a high mortality rate with estimates of between 12% and 30%. 1 Due to the high mortality rate, swiftly making the diagnosis and treating is key. Although this condition is rare, there are common risk factors outlined in the literature that clearly overlap with cholelithiasis. Some commonly cited risk factors include an age greater than 60 years, female gender, and existing biliary disease. 1 BS occurs when an episode of acute cholecystitis causes inflammation with subsequent attachment of the gallbladder to the GI tract. This can cause formation of an ischemic tear leading to the development of a fistula between the gallbladder and bowel. 2 Necrosis secondary to chronic inflammation and decreased perfusion of the gallbladder and intestines may further facilitate spontaneous fistula formation and lead to BS. 2 In general, there are many types of bilioenteric fistulas. The literature suggests that the most common form is the cholecystoduodenal fistula which accounts for about 68% of cases. 3 Other variants, like cholecystocolic (17%), cholecystogastric (5%), and choledochoduodenal (5%) fistulas are less common. 3
Diagnosis is challenging since literature has shown that the most common symptoms are nonspecific such as nausea (86%) and abdominal pain (71%). 4 Rigler’s triad, which is gastric outlet obstruction, pneumobilia, and an ectopic gallstone, found on imaging is pathognomonic for BS 4 . Computed tomography (CT) scan has high sensitivity (90%–93%), specificity (100%), and a diagnostic accuracy of 99% in identifying ectopic gallstones. 5 Magnetic resonance cholangiopancreatography (MRCP) is also effective with a sensitivity of 97.7%. Other advantages include better detection of fistulas and Rigler’s triad (100%) when compared to CT (77.8%). 5 Our patient had MRCP findings of acute cholecystitis with a large 2.7 cm gallstone, but diagnosis of BS only occurred during an exploratory laparotomy requiring urgent endoscopic intervention.
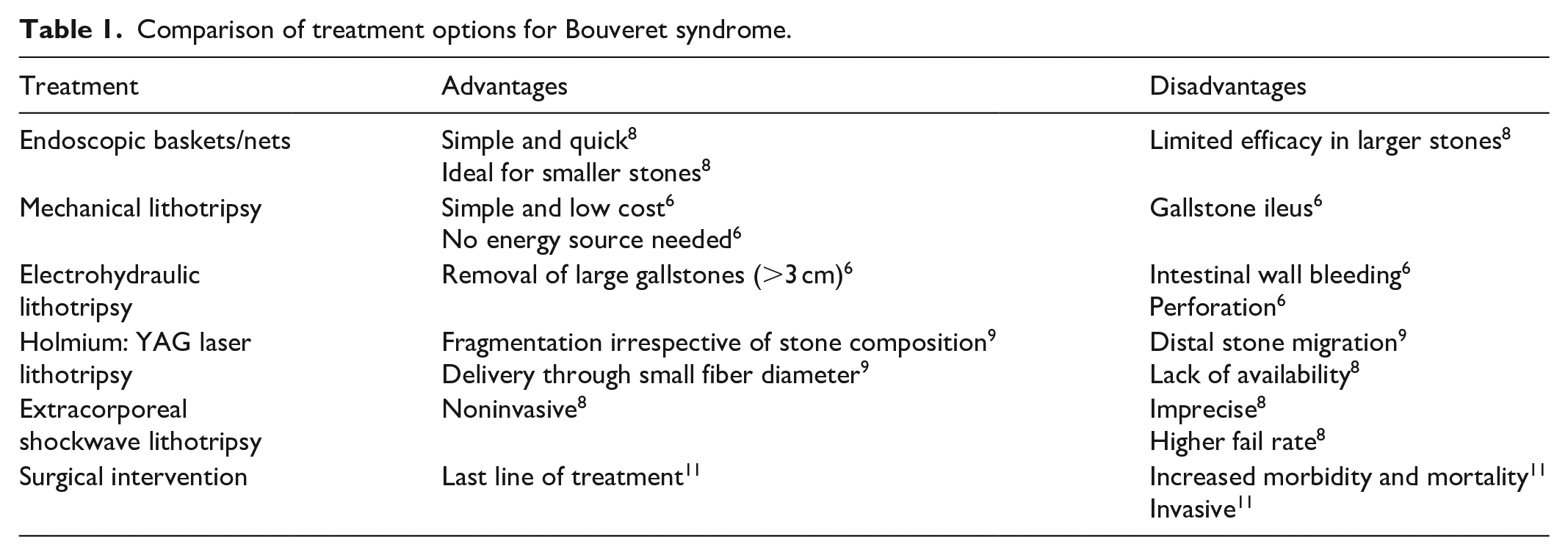
A comparison of treatment modalities is found in Table 1. Treatment generally consists of minimally invasive or surgical interventions but often requires endoscopic management with endoscopic nets and lithotripsy, especially in patients who are not surgical candidates. Mechanical lithotripsy is the most common form of lithotripsy and involves snares, baskets, or forceps to break gallstones into retrievable pieces. 6 For example, Afzal et al. reports a 79-year-old female diagnosed with BS that was endoscopically treated using mechanical lithotripsy and retrieval of stone pieces using nets. 6 Electrohydraulic lithotripsy involves shockwaves produced by a vaporization bubble expanding and collapsing repeatedly, creating a pressure wave to break up stones. 7 Allen et al. describes a case of a 71-year-old male presenting with melena and ultimately diagnosed with BS, who successfully underwent electrohydraulic lithotripsy. 7 Possible complications in this situation include intestinal wall bleeding or perforation, but these may be mitigated with water immersion and frequent irrigation. 8 Laser lithotripsy involves a targeted beam to break gallstones into smaller fragments and carries the benefit of precise targeting of gallstones, which is also outlined in the literature in cases involving rhodamine and holmium:YAG lasers.9,10 Extracorporeal shockwave lithotripsy utilizes acoustic shock waves to break down gallstones but has higher failure rates due to its imprecise nature. 8 It does, however, have a role when stones may not be easily accessible endoscopically, but typically requires other forms of lithotripsy in conjunction. 11 Endoscopic treatments carry lower morbidity and mortality rates compared to surgery (1.6% vs 17.3%) but have lower success rates (43% vs 94.1%)12,13 although literature has shown an increase in success rate over the years from initially around 13% to 16% to 43%. 14 A repeat EGD may also play a role in the management of BS due to the risk of recurrent BS, as outlined in a case by Goldstein et al. in which the patient had recurrent gallstone ileus after 1 month. 10
Comparison of treatment options for Bouveret syndrome.
Conclusion
Bouveret syndrome is a rare subtype of gallstone ileus causing gastric outlet obstruction secondary to bilioenteric fistula formation. Diagnosis is considerably challenging, needing high suspicion, due to vague symptoms and overlap with conventional cholelithiasis risk factors. This case highlights the potential limitations of the current gold standard imaging techniques and emphasizes the need for endoscopic consultation in patients with established history of cholelithiasis for rapid diagnosis.
Footnotes
Acknowledgements
Not applicable.
Ethical considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent to participate
Consent to participate was obtained from the patient.
Consent for Publication
Informed written consent was obtained from the patient for their anonymized information to be published in this article.
Author Contributions
All authors meet the four ICMJE authorship criteria. All authors contributed to the conception or design of the work and assisted in drafting, reviewing, and editing it. All authors approve of the final product and agree to be accountable for all aspects of the work.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Not applicable.