
Abstract
Cervical stenosis and labial adhesion associated with vulvovaginal atrophy (VVA) obstruct access to the uterine cavity and reduce quality of life. Removal of intrauterine contraceptive devices (IUD) is challenging without adequate cervical ripening in postmenopausal women. Local estrogen administration and mechanical dilatation are performed to improve these conditions; however, alternatives are necessary for those who have difficulty with vaginal medication. We report five cases of short-term oral estriol administration in postmenopausal women. Case 1 was a 60-year-old woman with an endometrial lesion requiring differentiation from malignancy. Endometrial examination was challenging because of cervical stenosis and VVA. Case 2 was an 82-year-old woman who had a giant ovarian tumor with fluid retention in the cervical canal owing to complete obstruction of the cervical external os. Case 3 was an 80-year-old woman who presented with pain during urination due to recurrent labial adhesion despite undergoing a surgical incision. Case 4 was a 58-year-old woman with suspected cervical cancer. Magnetic resonance imaging and conization were challenging owing to the difficulty in removing a metallic IUD from the uterine cavity. Case 5 was a 56-year-old woman who presented with abnormal uterine bleeding with a metallic IUD embedded in the myometrium and cervical canal. Improvement of cervical stenosis and obstruction after oral estriol administration allowed cervical and endometrial examinations, including cytology, biopsy, and hysteroscopy, and removal of IUD. Furthermore, incision followed by oral estriol administration prevented re-adhesion of the labia and improved urinary symptoms. Adverse events involving grade 1 abnormal genital bleeding and urinary urgency in two women were tolerable. Although this is a preliminary observation requiring confirmation, short-term estriol administration improved VVA, induced cervical ripening, prevented re-adhesion of the labia, and facilitated IUD removal in postmenopausal women in this case series.
Introduction
Postmenopausal cervical stenosis and labial adhesion associated with vulvovaginal atrophy (VVA) reduce the quality of life of postmenopausal women. Patients with VVA frequently present with related symptoms such as vaginal dryness, dyspareunia, abnormal vaginal discharge, and genital pain. 1 Cervical stenosis with VVA makes endocervix and endometrium examinations, including cytology, biopsy, and diagnostic hysteroscopy, difficult to perform. 2 They also lead to fluid retention in the cervical canal and endometrial cavity, resulting in local inflammatory conditions such as pyometra. Labial adhesion with VVA not only obstructs access to the uterine cavity but also causes lower abdominal pain and a sensation of incomplete bladder emptying due to urinary symptoms. 1 Moreover, the removal of an intrauterine contraceptive device (IUD) is challenging in such patients.
Postmenopausal cervical stenosis and labial adhesion associated with VVA are caused by long-term estrogen deficiency; therefore, local estrogen replacement in the vagina can resolve these conditions. Estriol, an estrogen naturally synthesized in the human placenta, has a weaker estrogenic effect than estradiol and is effective for VVA without adverse events when administered vaginally. 3 Therefore, the vaginal administration of estriol tablets and the vaginal application of estriol cream are often performed to replace local estrogen in postmenopausal women with VVA. Notably, the local administration of estriol has a minimal effect on the endometrium compared with 17β-estradiol. It is considered not to increase the incidence of endometrial hyperplasia or endometrial cancer in postmenopausal women. 4 However, the administration of vaginal medication is sometimes challenging for individuals with cognitive decline or physical disability. Even among young women, some patients have psychological resistance to vaginal self-medication. Oral estriol administration is a potential alternative for improving VVA for such patients. Here, we report five cases in which short-term oral estriol treatment was administered to postmenopausal women who had cervical stenosis, recurrent labial adhesion, and challenging IUD removal.
Methods
Patient selection
We administered oral estriol to postmenopausal patients with VVA who needed cervical ripening to resolve cervical stenosis or closure of the external cervical os, to those who had a recurrent labial adhesion, and to those who had difficulty removing an IUD. These patients either had difficulty with vaginal administration of medication or preferred not to undergo vaginal administration.
Treatment protocols
The patients took 1 mg estriol tablet orally each day. In principle, a re-evaluation of the affected areas was to be performed after 14 days of administration; however, due to outpatient scheduling, some patients underwent re-evaluation after 10 or 16 days of administration.
Outcome assessments
The cervical ripening effect induced by estriol was confirmed through speculum examination. In cases with closure of the external cervical os, we confirmed resolution of the closure by visual inspection. In cases of stenosis near the internal cervical os, we inserted a uterine sound and Hegar cervical dilators to confirm alleviation of the stenosis. In cases of labial adhesion, we used visual and physical examinations to confirm that re-adhesion had not occurred.
Adverse event monitoring
Adverse events were monitored from the initiation of estriol administration until the end of follow-up. Abnormal genital bleeding, genitourinary symptoms, breast tenderness, thromboembolic events, and gastrointestinal symptoms were included as monitoring targets. The severity of adverse events was graded using Common Terminology Criteria for Adverse Events version 5.0 (https://ctep.cancer.gov/protocolDevelopment/electronic_applications/ctc.htm#ctc_60).
Follow-up procedure
In cases where cervical ripening was achieved and the scheduled procedure was successfully performed, no further follow-up was conducted. In cases of IUD removal, patients returned 2 weeks later for confirmation that the uterus showed no abnormalities after removal.
Cases
Detailed characteristics of all cases are shown in Table 1. The first case was a 60-year-old nulliparous woman who had multiple uterine fibroids and a thickened endometrium, and for whom endometrial malignancy should be ruled out (Figure 1(a) and (b)). Endometrial biopsy and diagnostic hysteroscopy were challenging owing to the cervical stenosis associated with VVA. Moreover, the patient was afraid of pain experienced during repeated unsuccessful endometrial biopsies at a former facility and psychological resistance to vaginal procedures. We administered 1 mg of oral estriol for 14 days, and a hysteroscope was passed through the cervical canal (Figure 1(c)). Diagnostic hysteroscopy revealed an irregularly shaped polypoid mass with abundant blood flow on its surface, suggesting an endometrial malignancy (Figure 1(d)), and the endometrial biopsy identified serous carcinoma of the endometrium. The patient underwent hysterectomy and retroperitoneal lymph node dissection followed by adjuvant chemotherapy. The pathological diagnosis of the resected uterus was serous carcinoma, and the clinical stage was stage 1A (pT1aN0M0) according to the TNM classification of malignant tumors, UICC eighth edition. VVA improved, and cervical ripening was achieved along with an increase in cervical mucus. No adverse events were observed during estriol administration and follow-up. The patient has maintained a disease-free survival for 14 months.
Summary of patient characteristics and treatment outcomes.

IUD: intrauterine contraceptive device; MRI: magnetic resonance imaging.
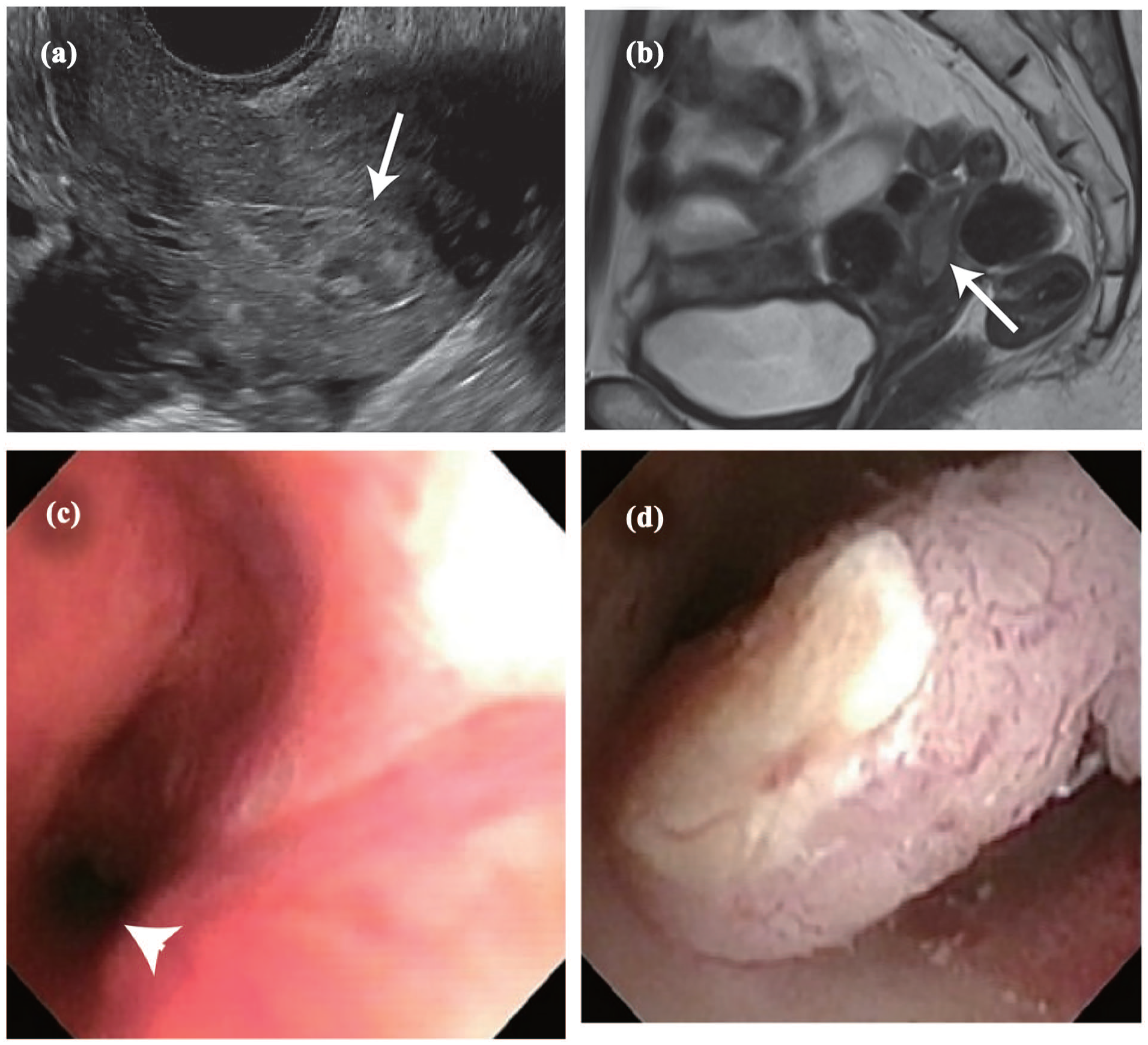
A case of endometrial cancer in which cervical stenosis was relieved by short-term oral estriol enabling diagnostic hysteroscopy and endometrial biopsy. (a) Transvaginal ultrasound imaging reveals endometrial thickness, suggesting an endometrial polyp (arrow). (b) T2-weighted sagittal MRI reveals endometrial thickness (arrow) and multiple uterine fibroids. (c, d) Changes after estriol administration. (c) After 14 days of oral estriol administration, the hysteroscope passed through the internal cervical os (arrowhead). (d) Diagnostic hysteroscopy after administration of oral estriol reveals a polypoid tumor with abundant atypical vessels on the surface, suggesting endometrial cancer.
The second case was an 82-year-old woman with a giant ovarian cystic tumor who presented with fluid retention in the cervical canal due to complete obstruction of the cervical external os (Figure 2(a)–(c)). The patient also had comorbid dementia with Lewy bodies. Cancer screening of the cervix and endometrium was required before surgery for the ovarian tumor. After 14 days of administration of 1 mg of oral estriol, the external cervical os was dilated enough to allow passage of a uterine sound, and fluid retention improved after aspiration of brownish contents using the Nelaton catheter (Figure 2(d)). Endocervical cytology was negative for malignancy. Subsequently, the patient underwent bilateral salpingo-oophorectomy, including resection of the ovarian tumor, along with omentectomy. The pathological diagnosis of the resected ovarian tumor was malignant; however, there was no evidence of peritoneal dissemination or metastasis to other organs. Considering the patient’s advanced age, no additional surgery or adjuvant chemotherapy was performed. Eight months after surgery, the patient’s dementia progressed, and follow-up was discontinued. VVA improved, and cervical ripening was achieved along with an increase in cervical mucus. No adverse events were observed during estriol administration and follow-up.

A case of fluid retention in the cervical canal due to obstruction of the external cervical os along with a giant ovarian tumor. (a) T2-weighted sagittal MRI reveals a giant ovarian cystic tumor 20 cm longest in diameter and fluid retention in the cervical canal (arrow). (b) T2-weighted axial MRI reveals a round fluid retention in the cervical canal (arrow). (c) Transvaginal ultrasound imaging reveals the fluid retention to be 3.1 cm longest in diameter due to the obstruction of the external cervical os. (d) After 14 days of administering 1 mg of oral estriol, the obstruction of the external cervical os resolved, and the fluid retention naturally flowed out of the vaginal cavity. Transvaginal ultrasound imaging reveals a normal cervical canal.
The third case was an 80-year-old woman with recurrent labial adhesion, despite repeated release procedures at a former facility, who presented with difficulty in urination. The patient was also treated with paracyclovir for genital herpes at a former facility. We released the adhesion using iris scissors under magnification at initial inspection and locally applied 17β-estradiol gel to prevent re-adhesion. However, the patient complained of localized pain, and re-adhesion occurred 2 weeks later (Figure 3(a)). Therefore, we re-released the adhesion using the same procedure and administered 1 mg of oral estriol for 16 days. No re-fusion was observed for at least 3 months postoperatively, and the patient’s urinary symptoms improved (Figure 3(b)). Therefore, regular follow-up was discontinued. Labial adhesion and VVA improved, and no adverse events were observed during estriol administration and follow-up.
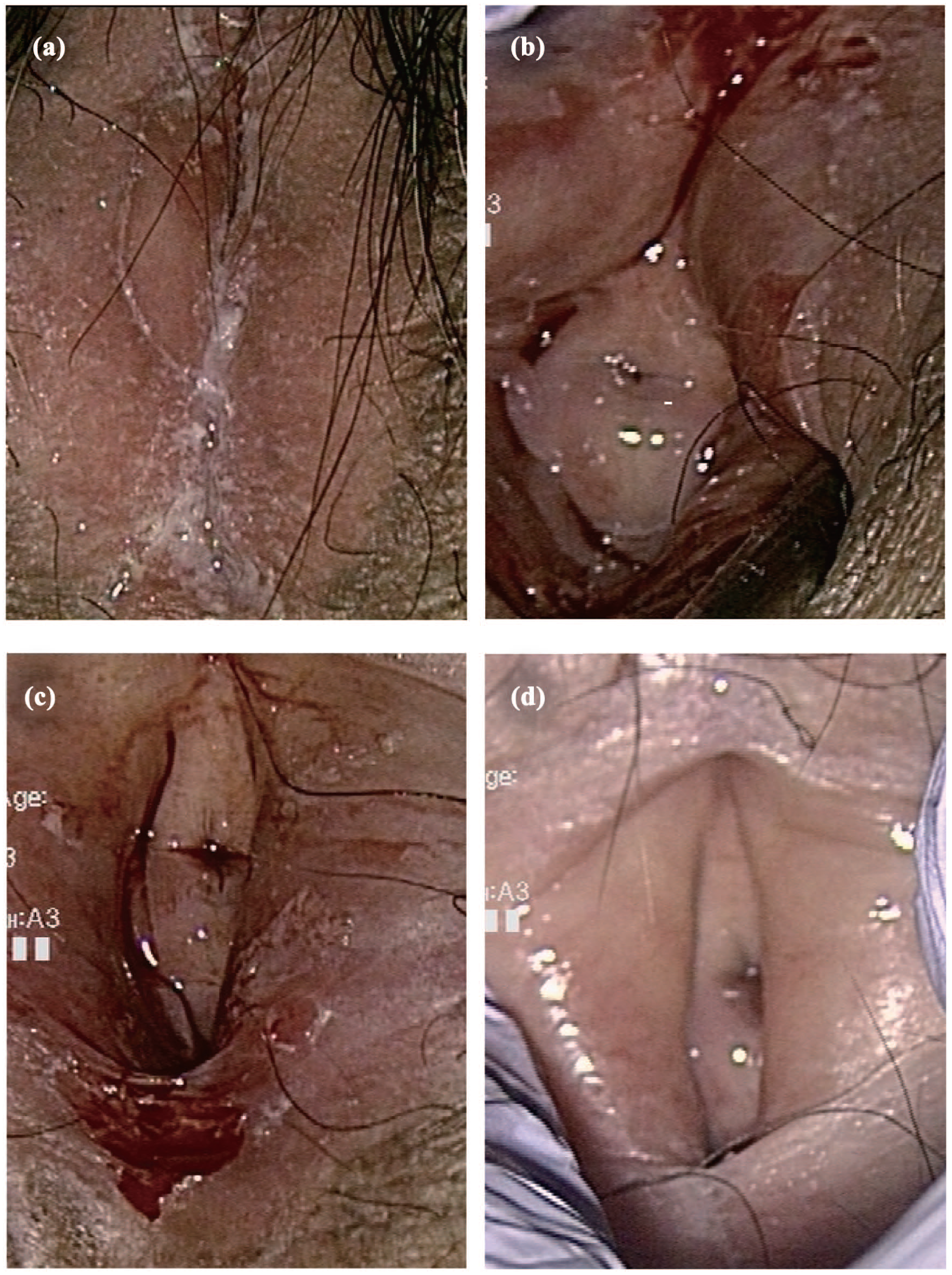
A case of refractory labial fusion despite repeated fusion open surgery. (a) Labial fusion at the time of referral to our department. Re-fusion is observed after multiple open surgeries performed at the former facility. (b) Labia after the initial surgery in our department. After applying vaginal estradiol gel postoperatively, the patient complained of pain, and the labia re-adhered. (c) Labia after the second surgery in our department. The labial adhesion is completely released by incising the adhesion site with iris scissors. (d) Labia 1 month after the second surgery. Two weeks after completing 16 days of oral estriol administration, local inflammation improves, and no re-adhesion of the labia is observed.
The fourth case was a 58-year-old woman with suspected invasive cervical cancer based on cervical cytology. Computed tomography and ultrasound performed at a former facility revealed a metal IUD embedded in the myometrium, and magnetic resonance imaging (MRI) was challenging to perform owing to the metallic foreign body (Figure 4(a)). The patient was referred to our department because of the difficulty in removing the IUD associated with VVA. We also attempted to remove the IUD but were unsuccessful because of cervical stenosis and VVA. In addition, sonohysterography identified part of the IUD embedded in the myometrium (Figure 4(b)). After 10 days of administration of 1 mg of oral estriol, a hysterofiberscope was able to pass through the cervical canal and revealed a metallic IUD embedded in both uterine horns (Figure 4(c)). Subsequently, the IUD was successfully removed, and the following MRI and diagnostic conization revealed invasive squamous cell carcinoma of the cervix; thus, total hysterectomy was performed (Figure 4(d)). VVA improved, and cervical ripening was achieved along with an increase in cervical mucus. The patient experienced Grade 1 urinary urgency during estriol administration, but it was tolerable. The patient continued to maintain a disease-free survival for 24 months postoperatively.

A case of difficulty in performing MRI and conization due to a metallic IUD in the uterine cavity. (a) Pelvic computed tomography reveals a high-density foreign body within the uterus (arrow). (b) Transvaginal ultrasound imaging demonstrates a shadow of an IUD located within the endometrial cavity and embedded in the myometrium, indicated as arrows. (c) Hysteroscopy after 10 days of oral estriol administration reveals part of the IUD positioned horizontally at the fundus of the uterus, while the remainder has penetrated the myometrium. (d) T2-weighted sagittal magnetic resonance image after IUD removal shows that the cervical cancer mass is not indistinct.
The last case was a 56-year-old woman who wanted the removal of a metallic IUD owing to abnormal uterine bleeding. Despite hospitalization and attempts to remove the IUD at a former facility, the removal was unsuccessful because the IUD was embedded in the cervix and protruded from the vaginal portion of the cervix rather than the external os (Supplemental Figure 1(a)), resulting in complex entrapment from the cervical canal into the myometrium (Supplemental Figure 1(b)). After 14 days of administering 1 mg of oral estriol, adequate cervical ripening was achieved, and the IUD was removed (Supplemental Figure 1(c)). The cervical portion protruding from the IUD showed slight erosion 2 weeks later (Supplemental Figure 1(d)). The patient presented with grade 1 abnormal uterine bleeding during estriol administration, but it was tolerable. VVA improved, and cervical ripening was achieved along with an increase in cervical mucus. No abnormal uterine bleeding has been observed after the IUD removal, and follow-up was concluded 1 month after IUD removal.
Discussion
We obtained adequate cervical dilatation, prevention of re-adhesion of the labia, and removal of the IUD in this case series. Adequate cervical dilatation with cervical ripening is necessary to perform endometrial examinations for endometrial thickening or lesions that do not exclude endometrial malignancies. It is also required to remove the IUD in postmenopausal women with VVA. Misoprostol administration and mechanical cervical dilatation are often performed before the outpatient hysteroscopy in premenopausal patients 5 ; however, the effectiveness of these procedures in postmenopausal patients has not been clarified. In addition, mechanical cervical dilatation using Laminaria rods, Lamicel cervical dilators (Medtronic Xomed, Inc., FL, USA), and Hegar dilators is a painful procedure, especially in postmenopausal women with VVA. Contrarily, many studies have shown the efficacy of vaginal estriol administration for VVA in postmenopausal patients.3,6,7 Furthermore, although limited in number, some studies have reported the effectiveness of oral estriol in treating VVA. A meta-analysis on the efficacy of oral estrogen, including estriol administration in managing urogenital atrophy in postmenopausal patients, revealed that low-dose oral estriol is effective for VVA but has no effect on the serum levels of estradiol. 7 Furthermore, 14 days of administration of 2 mg of oral estriol alters the vaginal flora, with a predominance of lactobacilli in postmenopausal older patients. 8 Daily oral estriol administration of up to 8 mg for 4 weeks significantly improves urogenital symptoms and exerts beneficial effects on the vaginal epithelium. 9 These reports provide a rationale for administering oral estriol tablets in place of vaginal estriol tablets.
Estriol is a final metabolite of estrogen synthesis and has a shorter estrogen receptor occupancy and lower receptor affinity compared with estrone and estradiol. Estriol has weaker effects on the endometrium compared to estradiol, and it selectively acts on the cervix and vagina. 10 Estriol increases cervical mucus secretion, promotes cervical ripening, and restores the vaginal self-cleaning mechanism compromised by estrogen deficiency. It also promotes keratinization of the vaginal epithelial cells and strengthens the vaginal defense against inflammation. After oral administration, estriol is readily absorbed and metabolized in the liver, and 1%–2% of the administered dose reach the circulation in its unchanged active form, conferring beneficial effects on the vaginal epithelial tissue. On the other hand, intravaginal administration of estriol directly binds to estrogen receptors in the lower genital tract and changes vaginal flora with a significant decrease in vaginal pH and an increase in the rate of vaginal colonization with lactobacilli. 11 In addition to its local effects on the genitourinary system, estriol also exerts systemic effects. Oral administration of estriol results in a transient increase in serum estriol levels, which may lead to breast tenderness even after short-term use. 12 Although the incidence of adverse events in estriol is lower compared to estradiol, long-term administration requires careful monitoring for potential risks of thromboembolism and breast cancer. With vaginal administration, systemic absorption of estriol is minimal, and it is estimated that a dose 10–20 times higher than that of oral administration would be required to produce comparable systemic effects. 10 Therefore, continuous administration of 1 mg of oral estriol for up to 16 days, as used in this case series, is considered to have minimal impact on endometrial proliferation. Local estriol administration for VVA-related genitourinary symptoms does not increase the risk of endometrial hyperplasia and endometrial cancer, 13 and long-term use of oral estriol does not increase the prevalence of endometrial hyperplasia and endometrial cancer. 14 Daily single-dose treatment with vaginal estriol is safe and does not increase the risk of endometrial proliferation and hyperplasia. 15 Moreover, vaginal estriol treatment of genitourinary syndrome of menopause in breast cancer and gynecologic cancer survivors, including endometrial cancer, improved associated symptoms and were not associated with cancer recurrence over the 6-month follow-up. 16 All these reports examined the effects of estriol on normal endometrium but not in endometrial cancer. Therefore, estriol should be administered in the smallest possible dose for the shortest possible duration in patients with endometrial lesions for which malignancy cannot be ruled out. If endometrial cancer is diagnosed after estriol administration, it is necessary to quickly proceed to the next treatment step.
IUD insertion is the most widely used contraception method worldwide, particularly in developing countries. The contraceptive efficacy of an IUD is as high as that of oral contraceptives, and once inserted, it can remain in place until menopause, making it a widely adopted method. Although IUD removal is recommended after menopause, many women remain asymptomatic even if the IUD remains in place. Furthermore, IUD removal after menopause can often be painful; as such, many women may leave it in place. The removal of an IUD inserted during reproductive age is challenging in postmenopausal women with cervical stenosis and VVA; adequate cervical ripening prior to IUD removal is necessary.
Labial adhesion is rare post-menopause but is more commonly observed in older individuals. Hypoestrogenism, virginity, sexual inactivity, cervical cancer, hysterectomy, urinary tract infection, and lichen sclerosis are risk factors for labial adhesion in postmenopausal women. 17 Surgery to release the adhesion is an effective approach with a low recurrence rate; however, recurrent re-adhesion may occur in older women with VVA. Local estrogen supplementation in addition to the adhesion-releasing surgery may be effective in cases of recurrent re-adhesion. 18 In the third case, we initially administered 17β-estradiol gel locally, but the patient presented with vulvar pain, and re-adhesion of the labia occurred. After the oral estriol administration, neither localized pain nor burning sensation was observed, and re-adhesion did not occur. Although we do not expect such favorable results in all cases, labial incision surgery followed by oral estriol administration may be a treatment option for recurrent labial adhesion in older women.
Adverse events were observed in two patients during estriol administration: grade 1 urinary urgency and abnormal vaginal bleeding. In both patients, a metallic IUD was embedded in the uterus. Generally, estriol administration improves urinary urgency caused by stress urinary incontinence, urinary tract infection, and overactive bladder symptoms in postmenopausal women.11,19 The patient who reported urinary urgency had previously undergone two unsuccessful attempts at IUD removal, once at the referring hospital and once at our institution, prior to the initiation of estriol administration. After successful removal of the IUD, the patient’s symptoms resolved. It is possible that this background contributed to the urinary urgency observed during estriol administration. The patient who experienced abnormal vaginal bleeding during estriol administration exhibited a shift in the position of the metallic IUD, which had been embedded in the cervical canal, associated with cervical ripening before and after estriol treatment. This positional change may have contributed to the bleeding.
This study has some limitations. The most critical limitation of this case series is the absence of an appropriate control group. Since this case series targeted patients in whom standard treatments including vaginal administration of estriol and mechanical cervical dilation was inherently difficult, a control group could not be established. Next, the follow-up period after estriol administration was short. Among the five cases in this series, two patients underwent hysterectomy, and one patient developed worsening dementia, making continued outpatient follow-up unfeasible. In the case where labial adhesion was released, the patient was advised to return if any issues arose, but no follow-up visit occurred. In the case where a metallic IUD was removed, the initial therapeutic objective had been achieved, and further follow-up was deemed unnecessary. Nevertheless, in cases with a preserved uterus, the influence of estriol on the endometrium needs to be considered, and long-term follow-up may be required. Moreover, estriol was principally administered for 14 days; however, there was a variation in the duration of estriol administration. One patient received a 10-day administration of estriol, and another received a 16-day administration due to patient-related factors. The estriol administration duration could influence outcomes. In the patient who received a 10-day course of oral estriol, the improvement in VVA appeared to be modest, whereas in the patient treated for 16 days, both vaginal epithelial maturation and VVA improvement seemed more pronounced. Notably, adverse events were observed even in the patient who received a 10-day administration of estriol. Lastly, quantification of outcomes using the degree of cervical dilation and symptom scores was challenging because the location and severity of cervical stenosis differed among cases, and the only patient who had subjective symptoms was the one with refractory labial adhesion. It is worth noting that the effectiveness of oral estriol for VVA and the lack of proliferative effects on the endometrium observed in this small case series represent only preliminary findings.
Conclusion
Short-term oral estriol administration improved cervical stenosis, prevented re-adhesion of the labia, and made it possible to remove the IUD in postmenopausal women. The oral estriol administration had good compliance, and the adverse events were well-tolerated even in older patients. Although these results are promising, drawing definitive conclusions based on a case series of only five patients is challenging. More extensive randomized controlled trials and optimal dosing studies are needed to validate these results.
Supplemental Material
sj-jpg-1-sco-10.1177_2050313X251358978 – Supplemental material for Short-term oral estriol for cervical stenosis, labial adhesion, and challenging intrauterine contraceptive device removal in postmenopausal women: A case series
Supplemental material, sj-jpg-1-sco-10.1177_2050313X251358978 for Short-term oral estriol for cervical stenosis, labial adhesion, and challenging intrauterine contraceptive device removal in postmenopausal women: A case series by Ayano Yuge, Hiroshi Ishikawa, Rie Okuya, Yuki Goto, Meika Kaneko and Kaori Koga in SAGE Open Medical Case Reports
Footnotes
Acknowledgements
Ethical considerations
Ethical approval to report this case series was obtained from the Ethics Review Committee for Observational Studies, Chiba University Hospital (HK202312-09).
Consent for publication
Written informed consent was obtained from all patients to publish this case series, including any accompanying images.
Author contributions
Ayano Yuge contributed to the data curation, investigation, validation, and writing – original draft. Hiroshi Ishikawa contributed to the conceptualization, investigation, validation, formal analysis, visualization, and writing – review and editing. Rie Okuya contributed to the data curation and validation. Yuki Goto contributed to the data curation and validation. Meika Kaneko contributed to the data curation and validation. Kaori Koga contributed to the conceptualization, validation, funding acquisition, and supervision. All authors have approved the submission of this version of the manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is supported by a Health and Labour Sciences Research Grant from the Ministry of Health, Labour and Welfare of Japan, (23FB1003).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.