
Abstract
Spontaneous pneumomediastinum is associated with SARS-CoV-2 infection-related respiratory manifestations. Coexistence of pneumomediastinum with severe pneumonia may interfere with providing mechanical ventilation due to the possibility of the development of tension inside the mediastinum. We describe a case of severe COVID-19 pneumonia with spontaneous pneumomediastinum and subcutaneous emphysema who required mechanical ventilation. A novel drain was inserted into the mediastinum to decompress the large pneumomediastinum. A 47-year-old male with severe COVID-19 pneumonia required invasive ventilation due to respiratory failure. With the commencement of invasive ventilation, the patient developed a large pneumomediastinum with extensive subcutaneous emphysema. With the deterioration of COVID-19 pneumonia, it was necessary to increase respiratory parameters but was limited because of the possibility of tension pneumomediastinum. Two different drains were inserted, one to the subcutaneous space and the other to the mediastinum. A fenestrated suction drain with an outer protective sheath was created using a 24 Fr chest drain tube and a temporary peritoneal dialysis catheter increment of positive end-expiratory pressure was limited by the risk of development of tension pneumomediastinum. After the procedure, the patient slowly improved over the next few days. After 7 days of the procedure, the patient succumbed due to a secondary bacterial infection of the lung. This case report highlights that a simple technique using easily available equipment improves the condition and can assist in the escalation of ventilatory support in patients with pneumomediastinum.
Background
SARS-CoV-2 virus can lead to a spectrum of respiratory diseases ranging from asymptomatic infection to severe acute respiratory distress syndrome-like picture. 1 Although pneumomediastinum is uncommon with viral pneumonia, there are several case reports available describing spontaneous pneumomediastinum of variable severity in association with SARS-CoV-2. 2 In most cases, this is incidental.2,3 The pathophysiology is attributed to the Macklin effect. Macklin first observed that air released from alveolar rupture migrates centripetally, dissecting through the pulmonary interstitium along the bronchovascular sheaths toward the pulmonary hila and into the mediastinum. 4 Even though this is commonly associated with blunt chest trauma, case reports are available indicating its effect on spontaneous pneumomediastinum. 4 Most cases are self-limiting.
In some cases, a breach in the visceral pleura or peritoneum allows air to escape into the pleural cavity (pneumothorax) or peritoneal cavity (pneumoperitoneum), where they may be managed in the standard manner. If this “escape” does not happen in a large pneumomediastinum, it can adversely affect the dynamics of ventilation in a mechanically ventilated patient. An increase in positive end-expiratory pressure (PEEP) will increase the leaking of air through damaged alveoli, increasing the risk of tension pneumomediastinum. We report a case of a patient with massive pneumomediastinum and subcutaneous emphysema during mechanical ventilation for severe COVID-19 pneumonia, which was managed by inserting a novel mediastinal drain.
Case presentation
A 47-year-old male was admitted to a local hospital with fever, cough, and dyspnea for 3 days during the first wave of COVID-19. He tested positive for the SARS-CoV-2 virus on admission. Initial screening was done with a rapid antigen test on admission; later, the diagnosis of COVID-19 was confirmed with polymerase chain reaction (PCR) testing of nasopharyngeal secretions. The patient had no comorbidities and was not on any medications. On arriving at the COVID-19 designated hospital, he was febrile but hemodynamically stable, with a blood pressure of 120/80 mmHg and a heart rate of 100/min. He was breathing through a non-rebreathing mask and recorded a saturation of 94% with a respiratory rate of 32/min.
He became increasingly hypoxic, with an initial chest radiograph showing bilateral patchy opacifications suggestive of COVID pneumonia. He was commenced on noninvasive ventilation and was treated with intravenous Dexamethasone 6 mg daily and subcutaneous Enoxaparin 60 mg daily due to high initial D-dimer levels. A Computerised tomography (CT) angiogram was not performed at this point as the patient was not stable enough to transfer to noninvasive ventilation. In addition, he received IV Cefuroxime 750 mg tds for a possible secondary infection.
On the 4th day, he further deteriorated, needing mechanical ventilation and admission to Intensive Care Unit (ICU). Here, we noticed that the patient had developed subcutaneous emphysema. A chest radiograph (Figure 1) showed extensive subcutaneous emphysema with features of severe COVID-19 pneumonia.
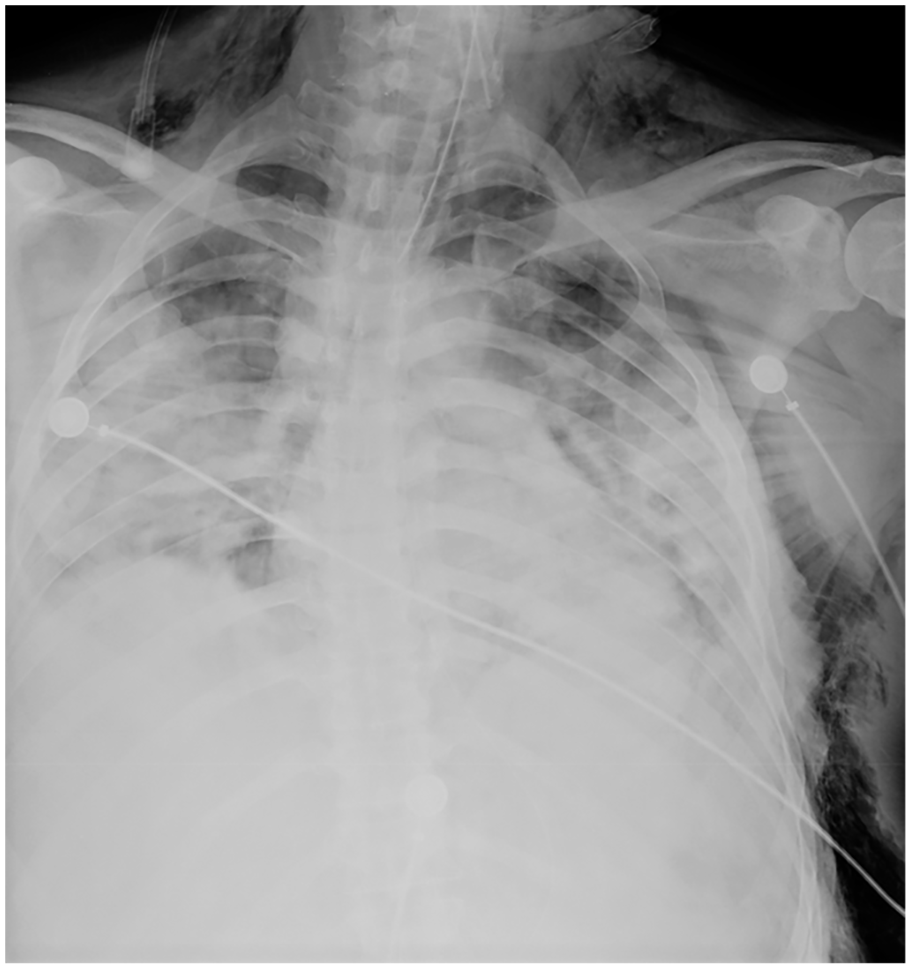
Chest radiograph showing bilateral patchy consolidation suggestive of COVID pneumonia and extensive subcutaneous emphysema.
A chest CT was performed on the second day of ICU, which showed a large pneumomediastinum with subcutaneous emphysema. It also showed bilateral ground-glass opacifications compatible with severe COVID-19 pneumonia (Figure 2).

CT showing coronal and sagittal views of the chest. Shows extensive diffuse ground glass opacities involving most of both lungs with bilateral lower lobe consolidations. There is extensive pneumomediastinum with extensive subcutaneous emphysema noted involving the face, neck, and chest wall.
The patient further deteriorated, requiring 100% oxygen. The patient was ventilated with a lung protective strategy with volume control ventilation. The initial 6 mL/kg tidal volume was reduced to 4 mL/kg as the plateau pressure rose from 28 to 32 mmHg. The initial oxygenation level was maintained at 60–70 mmHg. His CO2 was on a rising trend, and by the end of 3rd day, it was 65 mmHg with a PH of 7.21. With the presence of pneumomediastinum, PEEP was kept at 5 cm H2O. Prone ventilation was not attempted at this point due to the presence of pneumomediastinum.
On 3rd day in the ICU, the patient desaturated further. Bilateral subcutaneous drains were inserted into the subcutaneous space in the upper part of the chest to release pressure in the subcutaneous space. Low-pressure suction was applied. This was not adequate as the patient deteriorated more rapidly. Further increment of PEEP was required in this case but would have led to an increase of the tension pneumomediastinum. Therefore, mediastinal drain insertion was planned.
Since the patient was not deemed stable for transfer to an operating theater, we had to devise a method that could be performed with minimal risk of complications in the ICU. A 2 cm incision was made at the lower margin of the xiphoid process under aseptic conditions and deepened up to the bone. From this entry, a plane was created cranially between the anterior mediastinum and the sternum with blunt dissection, taking care not to stray laterally and breach the pleural reflections. Immediate expulsion of gas was noted. Once a satisfactory space was created, a fenestrated suction drain with an outer protective sheath was created using a 24 Fr chest drain tube and a temporary peritoneal dialysis catheter. The outer sheath was added to prevent occlusion of the holes by tissue. The two tubes fitted together with a good seal. The inner tube was connected to a suction of −20 cm H2O across an underwater seal bottle (Figure 3). Immediate bubbling was noted. The incision was closed with an anchoring suture for the drain.
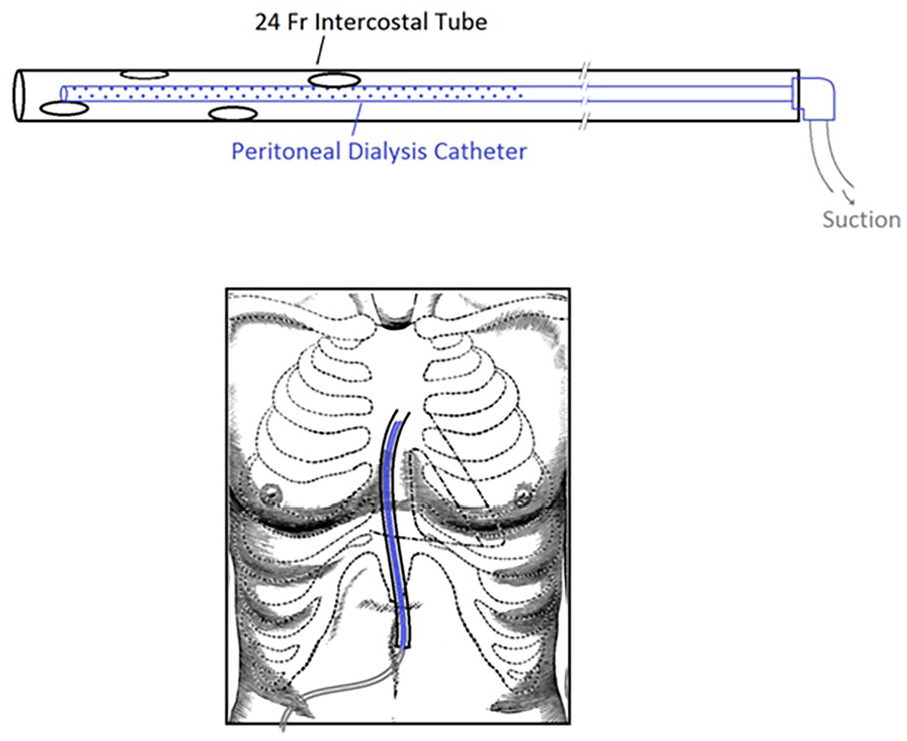
Illustration showing the novel drain made up of a peritoneal dialysis catheter with an outer protective sheath using an intercostal drain (above), Its placement in the chest (below).
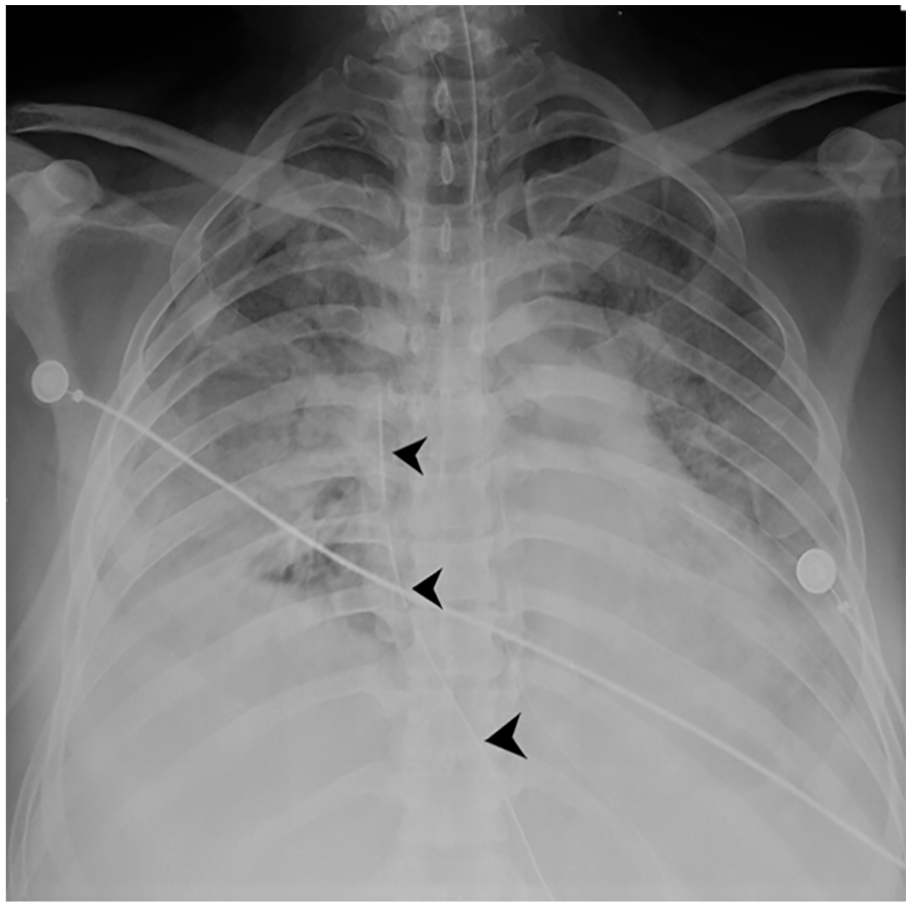
Figure 4 shows the chest radiograph following the insertion of the mediastinal drain.

Chest radiograph showing mediastinal drain in situ (Arrowheads). Features of bilateral patchy consolidation suggestive of severe COVID-19 pneumonia with extensive subcutaneous emphysema are also seen.
With the insertion of the mediastinal drain, we could gradually increase his PEEP to match his oxygen requirement. Within 6 h of releasing pneumomediastinum, PEEP was increased from 5 to 10 cm H2O. Tidal volumes were also increased to 6 ml/kg by the end of day one, keeping plateau pressure around 27 mmHg. Oxygenation was markedly increased from 55 to 80 mmHg at the end of day 1. CO2 clearance was observed over the next 48 h with clearing of acidosis.
Continuous bubbling of the suction through the mediastinal drain was observed. Over the next 3 days, gradual weaning of oxygen and PEEP was done. Clinically the subcutaneous emphysema cleared. Figure 5 shows the clearing of subcutaneous emphysema as seen in the chest X-ray.
A chest radiograph showing the clearing of subcutaneous emphysema. Mediastinal drain is also in situ (arrowheads).
On the 4th day after the insertion of the mediastinal drain, the patient started deteriorating with evidence of secondary bacterial pneumonia. The patient succumbed on day 7 of mediastinal drain insertion and 11 days post-admission.
Discussion
SARS-CoV-2 infection gives rise to a variety of respiratory system-related complications. Pneumomediastinum is one such complication that used to be rarely associated with viral pneumonia. 1 With the onset of the COVID-19 pandemic, there are many reported cases of pneumomediastinum. True incidence of COVID-19–associated pneumomediastinum is not known. Some studies have shown that the use of noninvasive ventilation and radiological severity of COVID-19 pneumonia predisposes to the development of pneumomediastinum in these patients. 5
A study done by Marza et al. 6 has shown pneumomediastinum is a serious complication of SARS-CoV-2 infection that increases the risk of in-hospital mortality by almost four times. Its association with COVID-19 pneumonia led to prolonged hospitalization and a high risk of fatal outcomes, especially among the elderly.
There are many causes leading to the development of pneumomediastinum, including damage to the tracheobronchial or esophagus, the presence of gas-forming organisms in the chest or bowel, and damage to the alveoli. Macklin and Macklin first observed the release of alveolar air from alveolar rupture, which dissects centripetally through the pulmonary interstitium along the broncho vascular sheaths toward the pulmonary hila and into the mediastinum. 4 This mechanism gives rise to pneumomediastinum without pneumothorax. Outpatient had this phenomenon, as shown by the chest CT. The air in the mediastinum will leak into the subcutaneous space, giving rise to subcutaneous emphysema. This usually does not need any interventions unless it is very severe.
Most pneumomediastinum are incidental findings that do not give rise to any clinical manifestations. Presence of pneumomediastinum can adversely affect the respiratory parameters of mechanically ventilated patients. Hypoxia in acute respiratory distrss syndrome (ARDS) can be managed with prone ventilation. This is the standard of care in COVID-19 patients as well.7,8 However, literature has shown that prone positioning in patients with acute respiratory distress is a known risk factor for pneumomediastinum and tension pneumomediastinum. 9 Our patient developed pneumomediastinum at the beginning of the respiratory distress, and therefore, prone ventilation was not done.
Increments in PEEP will lead to an increase in air accumulated in the mediastinum. This can lead to the rare complication of tension pneumomediastinum. Tension pneumomediastinum can be life-threatening due to hemodynamic instability. Therefore, this needs urgent intervention. There are no standard guidelines for the drainage of pneumomediastinum. Most of the simple ones are managed conservatively. Some case studies have suggested that severe cardiorespiratory effects due to the presence of air in the mediastinum warrant drainage. 10 The decision to drain the pneumomediastinum in our patient was challenging. The patient needed high PEEP to maintain oxygenation, and an increment of PEEP was associated with hemodynamic disturbances. Therefore, a decision was made to insert the drain, which allowed us to increase PEEP without any hemodynamic effects.
Campisi et al. 11 have described a technique of successful decompression of tension mediastinum through incisions made below the xiphoid process and above the sternal notch followed by mediastinal drain insertion.
The inserted drain was made in the form of a fenestrated suction drain with an outer protective sheath, which was created using a 24 Fr chest drain tube and a temporary peritoneal dialysis catheter. The outer sheath was added to prevent occlusion of the holes by tissue. The two tubes fitted together with a good seal. This improvisation was needed because there was no proper draining tube available. The post-tube insertion chest X-ray showed the appropriate placement of the tube, and we were able to go up on PEEP without any hemodynamic disturbances.
Conventional chest drains are used in the pleural cavity and as mediastinal drains in the mediastinal cavity, particularly after cardiac surgeries. In these instances, the pleural cavity is breached and the drain is placed to prevent pneumothorax or pneumohydrothorax and not for the purpose of pneumomediastinum. Our purpose was to drain a continuous leakage of air that would accumulate in the mediastinum. There is no actual space created, and the dissection was done through tissue planes. If only a conventional chest drain had been used, the tube would have gotten clogged easily with fat and tissue debris. Using a chest drain as a sheath while the actual suction is applied to the peritoneal catheter inside it would prevent the holes from being occluded from the materials.
Immediate bubbling of the tube was noted upon insertion of the mediastinal tube, suggesting the release of air in the mediastinum. The other rare possibility of this is the broncho-mediastinal fistula. Broncho-mediastinal fistula is usually associated with malignancy or infection. 12 In our patient the presence of this was unlikely as the CT did not show any evidence of this. The highly likely mechanism for the air in the mediastinum is the Macklin effect, as described previously.
Subcutaneous emphysema may be observed in association with pneumothorax or pneumomediastinum as a result of pathological changes in the respiratory tract. This can rarely be associated with airway compromise, respiratory failure, and death. 13 Treatment involves treating the underlying condition and most are managed conservatively. Sometimes, decompression may be done by making bilateral 3-cm infraclavicular incisions down to the pectoralis fascia.13,14 Fenestrated catheters have been used in the treatment of subcutaneous emphysema.13,15 The drainage of emphysema is debatable. In this patient, we decided to insert drains with the expectation of improvement of respiratory parameters, but this was unsuccessful.
The outcome related to pneumomediastinum is not being widely studied. However, our patient succumbed due to a secondary bacterial pneumonia complicating severe COVID-19 pneumonia.
Conclusion
Although often asymptomatic, pneumomediastinum could sometimes be detrimental to patients with severe COVID-19 pneumonia requiring high ventilatory support, due to the risk of tension affecting ventilator pressures. This simple technique using easily available equipment improves the condition and can assist in the escalation of ventilatory support.