
Abstract
Leukemia cutis (LC) is an uncommon cutaneous manifestation of leukemia that involves the leukocytic infiltration of the skin. LC typically presents after a diagnosis of leukemia has been made but may rarely appear before confirmation of the disease. In this report, we describe the case of an 86-year-old male presenting with LC prior to a clear diagnosis of leukemia in the blood. This case highlights the importance of early recognition of LC lesions, to ensure earlier detection of the neoplasm, particularly when they present as the first sign of disease.
Introduction
Leukemia cutis (LC) describes the leukemic infiltration of the layers of the skin, typically presenting with erythematous to violaceus papules or nodules.1,2 These lesions may also manifest as plaques, ecchymosis, palpable purpura, or erythroderma.3,4 Patients with leukemia who go on to develop LC survive an average of 3–30 months after the appearance of lesions. 5 Very rarely, however, as in this case report and 2%–3% of overall cases, LC can present before the actual diagnosis of systemic leukemia is confirmed, in which case it is termed “aleukemic cutis.”2,6,7 This can occur months to years before the disease is detected in bone marrow or peripheral blood, 2 making it essential for dermatologists to recognize the various cutaneous manifestations of LC.
Case report
An 86-year-old male presented to dermatology with a 4-week history of skin lesions located on the abdomen and lower back. On exam, the patient exhibited numerous erythematous papules and nodules that were irregular, irritated, and moderate in severity (Figure 1). The patient also reported experiencing blurry vision and joint aches but denied any unintentional weight loss, chills, abdominal pain, problems with bleeding, healing, or scarring. In addition, the patient reported a 20 pack-year history of cigarette smoking but had quit nearly 50 years ago. He has no history of skin cancer and no other significant medical history.
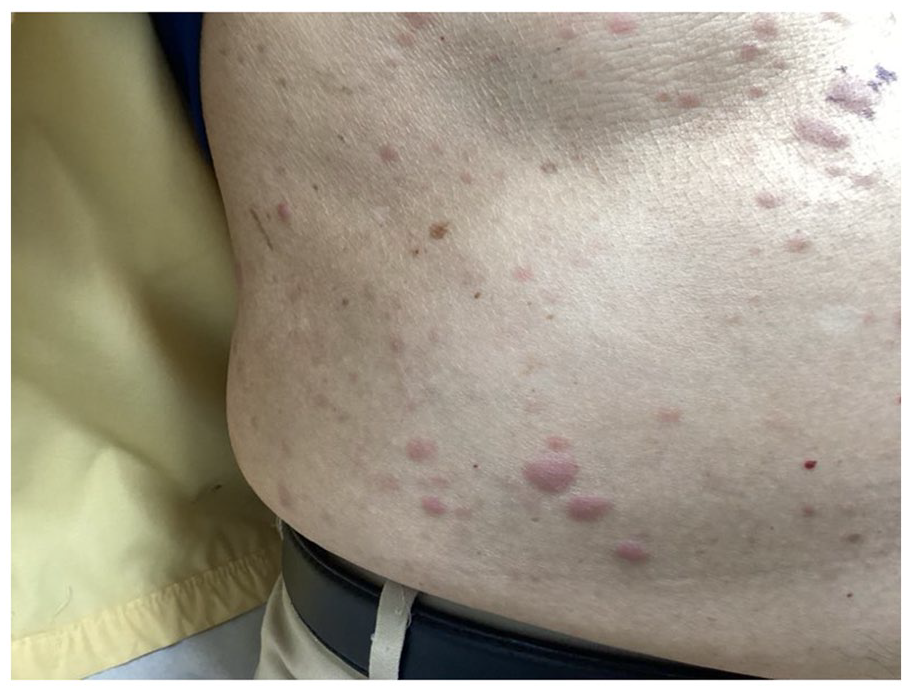
Leukemia cutis. Multiple red, irregular nodules and papules distributed on the abdomen and lower back region of the skin of an 86-year-old male.
Complete blood count results in 1 month prior to his visit revealed leukopenia (1,900/μL), anemia (3.24 million RBC/μL), mild thrombocytopenia (128,000/μL), and moderate neutropenia (766/μL). He also had elevated levels of C-reactive protein (19.5 mg/L) and alkaline phosphatase (249 U/L). His panel for sexually transmitted infections (STIs) was negative. A biopsy of the papules was conducted by shave method, 8 and microscopic analysis of the dermis revealed a dense infiltrate of monotonous neoplastic cells with dispersed chromatin and a high nuclear-to-cytoplasmic ratio (Figure 2). An immunohistochemical study was performed, and the neoplastic cells were found to be positive for CD15, CD33, CD43, CD56, and CD68 antigens and negative for Tdt, CD3, CD20, CD34, and CD117 antigens, confirming a diagnosis of myeloid LC (Figure 3).

Hematoxylin and eosin stain of the skin lesions revealing a dense infiltrate of monotonous neoplastic cells with dispersed chromatin and a high nuclear-to-cytoplasmic ratio, consistent with leukemia cutis (a) ×10 and (b) ×40.
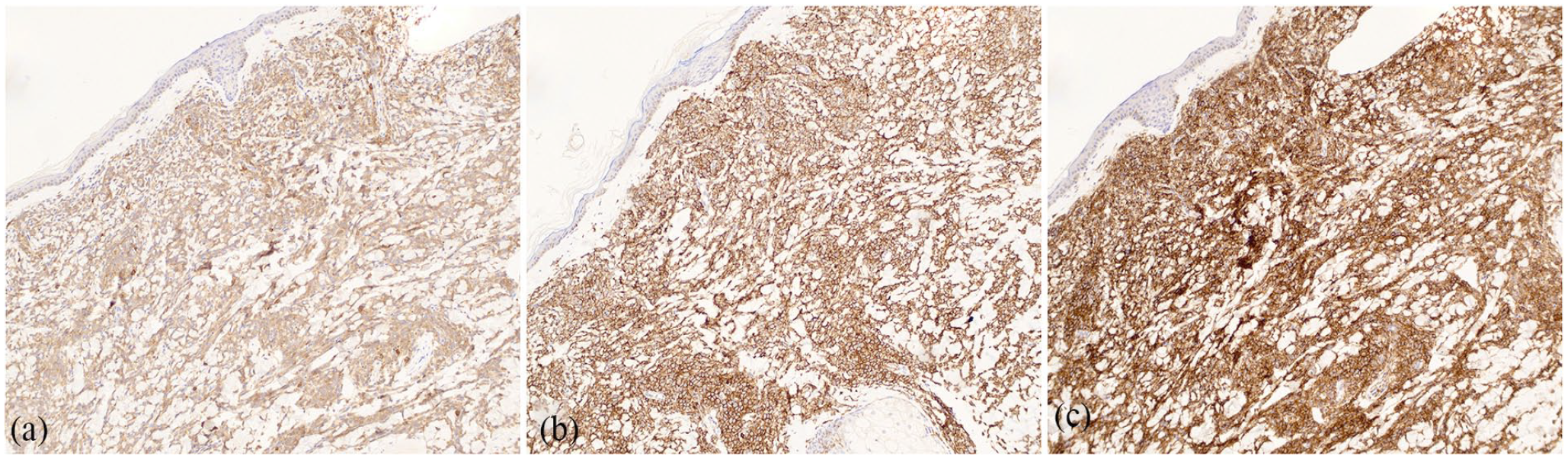
Immunohistochemical stains of the skin lesions showing cells positive for CD33 (a), CD43 (b), and CD56 (c), confirming a diagnosis of myeloid leukemia cutis.
Flow cytometry of a peripheral blood sample showed that 10.4% of lymphocytes and 6.1% of all cells analyzed were B cells. This B cell population appeared to show a slight excess of kappa light chain expression, with a kappa/lambda light chain ratio of about 4.1:1, but there were otherwise no signs of leukemia in the blood. Additionally, no aberrant expression of CD5 or CD10 was detected, and there was no immunophenotypic evidence of a T-cell lymphoproliferative disorder, acute leukemia, or an increase in circulating blasts. The patient was started on topical triamcinolone acetonide and referred to oncology, where peripheral blood studies were found to be unchanged from his last examination, and a bone marrow biopsy revealed no signs of leukemia.
Discussion
LC is usually a sign of a more advanced leukemia, associating the malignancy with a poor prognosis. 2 LC is present in 2% to 30% of leukemias, with the highest rates reported in acute myeloid leukemia and chronic lymphocytic leukemia. 2 Some of the differential diagnoses of LC include erythema exudativum multiforme, panniculitis, or other inflammatory and infectious agents.2,9 When LC presents on the trunk as in this case, it should be differentiated from basal cell carcinoma, squamous cell carcinoma, syphilitic papules, and pityriasis rosea. 9 Leukemia is also associated with other cutaneous manifestations that do not involve leukocytic infiltration, such as purpura, leukocytoclastic vasculitis, Sweet syndrome, and pyoderma gangrenosum.2,10
The pathogenesis of LC is poorly understood but is believed to involve increased leukocyte homing through chemokines and adhesion receptors.2,10 LC lesions have no predilection for a specific region of the body; however, they occur less frequently in the oral mucosa and palmoplantar surfaces. 9 Some lesions may also be associated with sites of previous surgeries, inflammation, or trauma.2,10
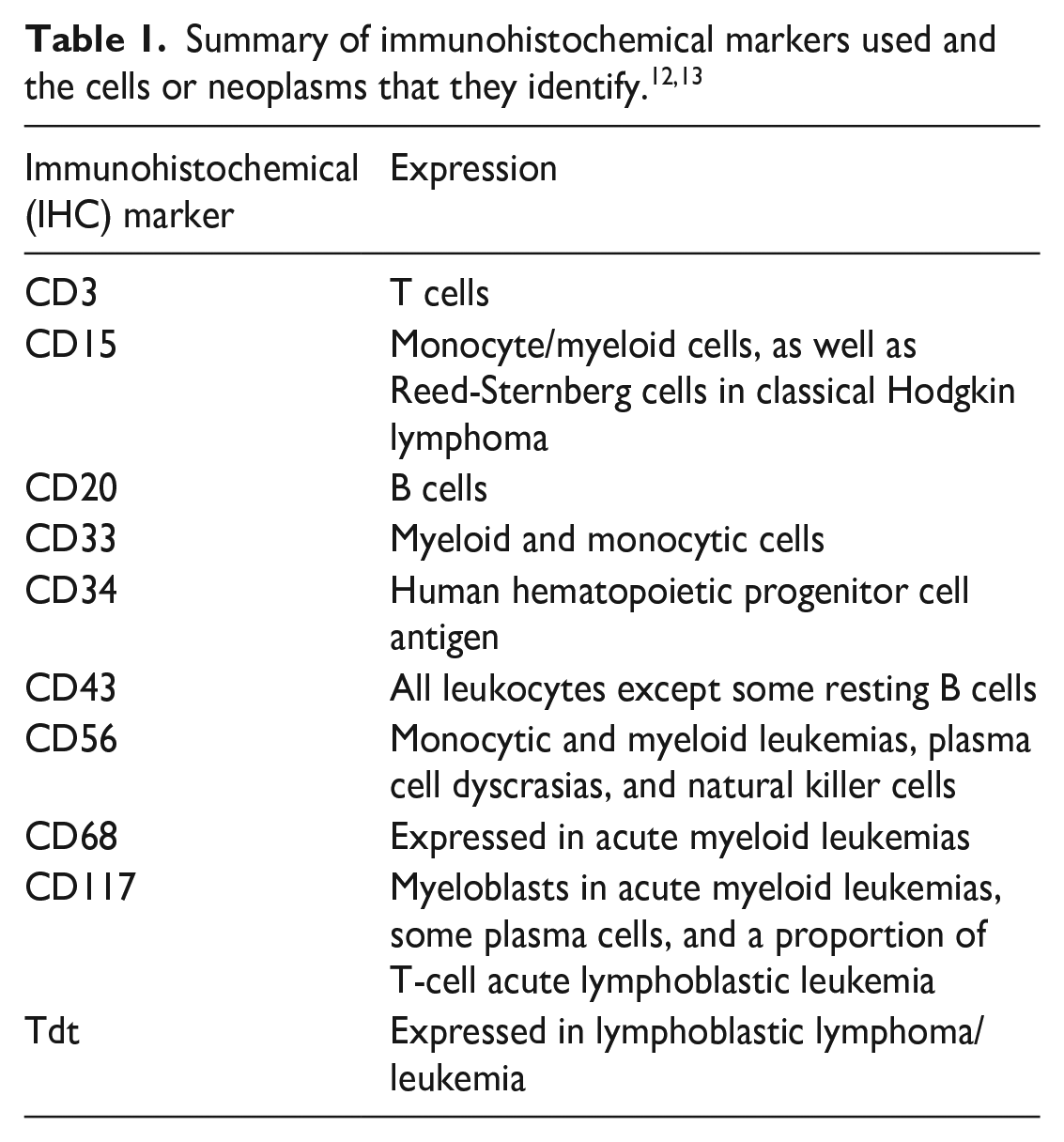
LC is diagnosed primarily by biopsy of the lesions, with histopathological analysis typically revealing a diffuse infiltrative pattern of the subcutis, superficial, or deep dermis.5,9,10 These infiltrates may also involve invasion of the vascular and adnexal structures. 5 Immunophenotyping of tumor cells through flow cytometry, along with clinical signs, helps confirm a diagnosis of LC and leukemia (Table 1).5,10 CD43 is a reliable marker that can be used to confirm the presence of myeloid cells in the skin, with CD56 providing further confirmation. 5 LC is also associated with a higher level of lactate dehydrogenase and B2 microglobulin. 10 Treatment of LC is dependent on therapy of underlying leukemia, with some local treatments such as gilteritinib showing positive results.2,11 Local radiotherapy can also be used in cases that do not remit with standard treatment. 2
Conclusion
LC is an uncommon cutaneous manifestation of leukemia. The presence of neoplastic, leukocytic cells in the skin without evidence of leukemia in the blood, as described in this report, is a very rare presentation. Recognition of these lesions may allow for earlier detection of leukemia prior to other signs of the disease.
Footnotes
Acknowledgements
None.
Author contributions
M.R.T. wrote the manuscript and reviewed the literature. S.K.T. edited the manuscript and provided the patient history and images.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.