
Abstract
This case series explores the diagnostic and management complexities of non-malignant ovarian masses, illustrated through three distinct cases: struma ovarii, mature teratoma, and ovarian mass with peritoneal splenosis. The first case details a struma ovarii initially misinterpreted as a potential malignancy due to its complex imaging features, leading to diagnostic uncertainty. The second case involves a mature teratoma, which, despite typical imaging characteristics, presented significant symptoms that necessitated careful clinical management. The third case highlights an ovarian mass with peritoneal splenosis, a condition often mistaken for metastatic disease, underscoring the need for differential diagnosis, particularly in patients with a history of splenic trauma or surgery. These cases emphasize the importance of a comprehensive diagnostic approach that integrates detailed imaging, surgical findings, and histopathological examination to accurately distinguish between benign and malignant ovarian masses and inform appropriate management strategies.
Keywords
Introduction
Ovarian masses present a broad diagnostic challenge due to their diverse etiology and potential for mimicking malignant conditions. These complexities often necessitate a multidisciplinary approach to accurately identify and manage these masses, avoiding unnecessary aggressive treatments while ensuring appropriate care. The variability in presentation and overlapping imaging characteristics with malignant tumors make it crucial to utilize a combination of clinical assessment, imaging, and histopathology to achieve accurate diagnoses. 1
This case series discusses three distinct presentations of non-malignant ovarian masses: struma ovarii, mature teratoma, and ovarian mass with peritoneal splenosis. Each case provides valuable insights into the diagnostic challenges and management strategies associated with ovarian tumors. Struma ovarii, a rare form of teratoma primarily composed of thyroid tissue, often presents imaging challenges that may suggest malignancy. 2 Mature teratomas, though generally benign, can lead to acute complications requiring timely intervention. 3 Peritoneal splenosis with adnexal mass, frequently misinterpreted as metastatic cancer on imaging, emphasizes the need for careful historical and diagnostic consideration to avoid unnecessary surgeries. 4
By focusing on the clinical presentations, imaging findings, 5 and surgical outcomes, this report aims to contribute to the broader understanding of ovarian mass management. It highlights the critical role of tailored therapeutic strategies based on precise diagnostic results. This approach not only aids in avoiding overtreatment but also underscores the importance of preserving patient quality of life whenever possible. The following case series will further showcase how diagnostic tests can guide healthcare professionals in the management of complex ovarian masses (struma ovarii, mature teratoma, and ovarian mass with peritoneal splenosis) along with assessing the necessity for surgical intervention when needed.
Case presentation
Case 1
A 34-year-old woman para 3+1 (3 alive) with a history of three cesarean deliveries presented with recent health concerns. She had regular menstrual cycles without menorrhagia or metrorrhagia, and her last menstrual period (LMP) was four months prior, coinciding with the onset of her symptoms. Although historically having regular menstrual cycles without menorrhagia or metrorrhagia and not taking any recent medication, she began experiencing heavy menstrual bleeding four months prior. This was accompanied by dysmenorrhea, dyspareunia, and low back pain. She reported no significant weight loss or other systemic symptoms and was not on any chronic medications. On physical examination, the abdomen was soft, non-tender, and non-distended with no signs of pallor, jaundice, or edema. During the pelvic examination, the cervix and vaginal walls appeared normal, and there was no abnormal vaginal discharge. The uterus presented regular dimensions. The left ovary was enlarged, raising suspicion of a mass a non-tender, while the right ovary was normal. There were no urinary or gastrointestinal symptoms reported by the patient.
Initial pelvic ultrasonography was performed in an attempt to rule out the presence of fibroids, endometriosis, or neoplasms. The pelvic ultrasonography identified a heterogeneous mass on the left ovary, which was further characterized by transvaginal ultrasonography as a large, complex pelvic mass of probable adnexal origin featuring neovascularization. The dimensions were 7 cm × 5 cm × 5 cm for the left complex ovarian cysts, with the right ovary presenting as normal. Nonetheless, following medical treatment, the cyst did not resolve. Accordingly, transvaginal ultrasonography was performed, which showcased that the cyst was vegetative in nature and not fluid filled. In order to rule out any malignancy, tumor markers CA 125 and Carcinoembryonic Antigen (CEA) were checked, resulting in values within normal ranges and not indicative of malignancy.
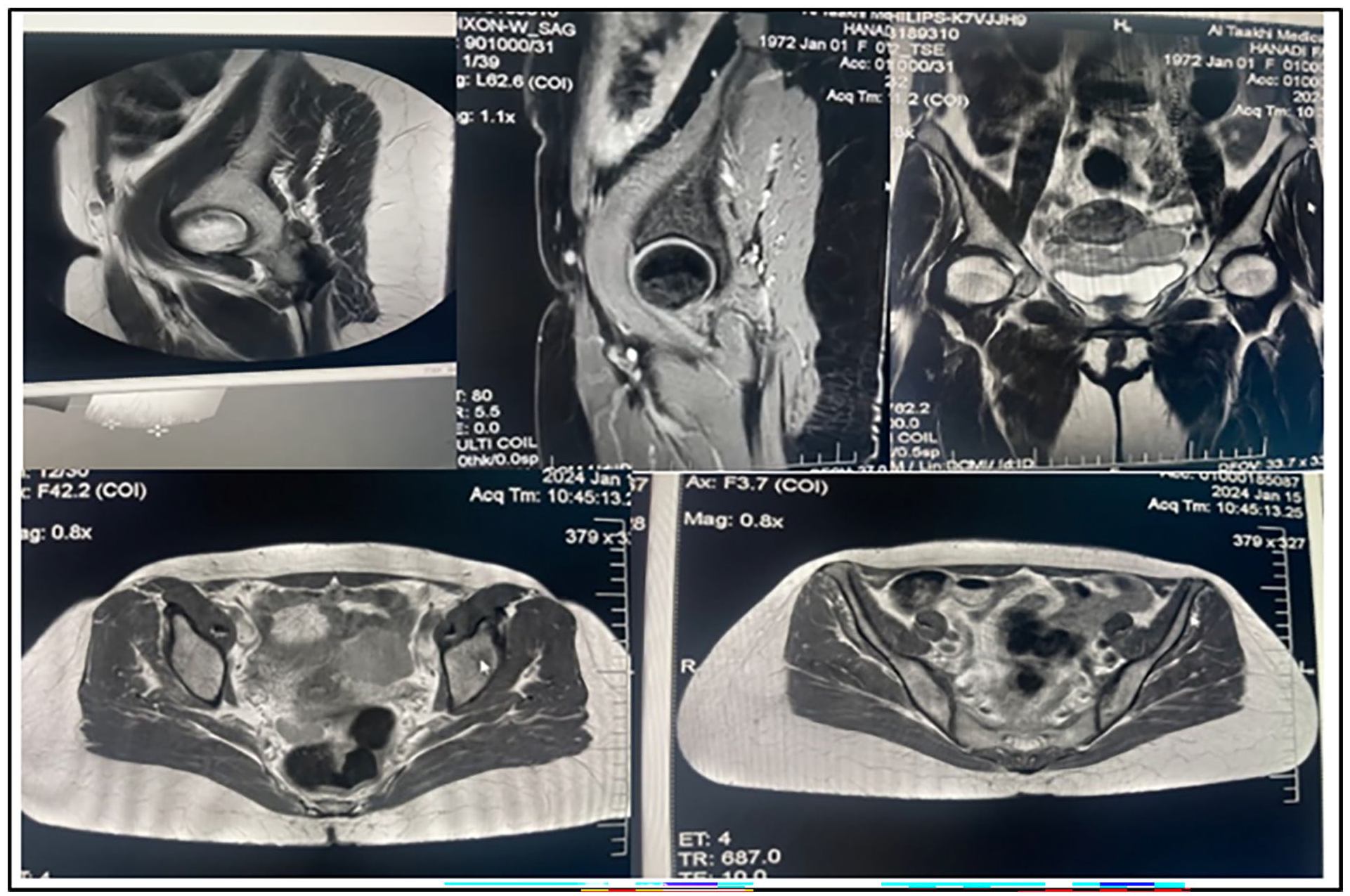
In an attempt to further assess the morphology of the cyst, magnetic resonance imaging (MRI) scans, both T1 and T2 weighted, were performed. The results displayed a multicystic tumor with a solid component and a multilobulated surface, with signal intensities suggesting the presence of viscid, gelatinous material (Figure 1).
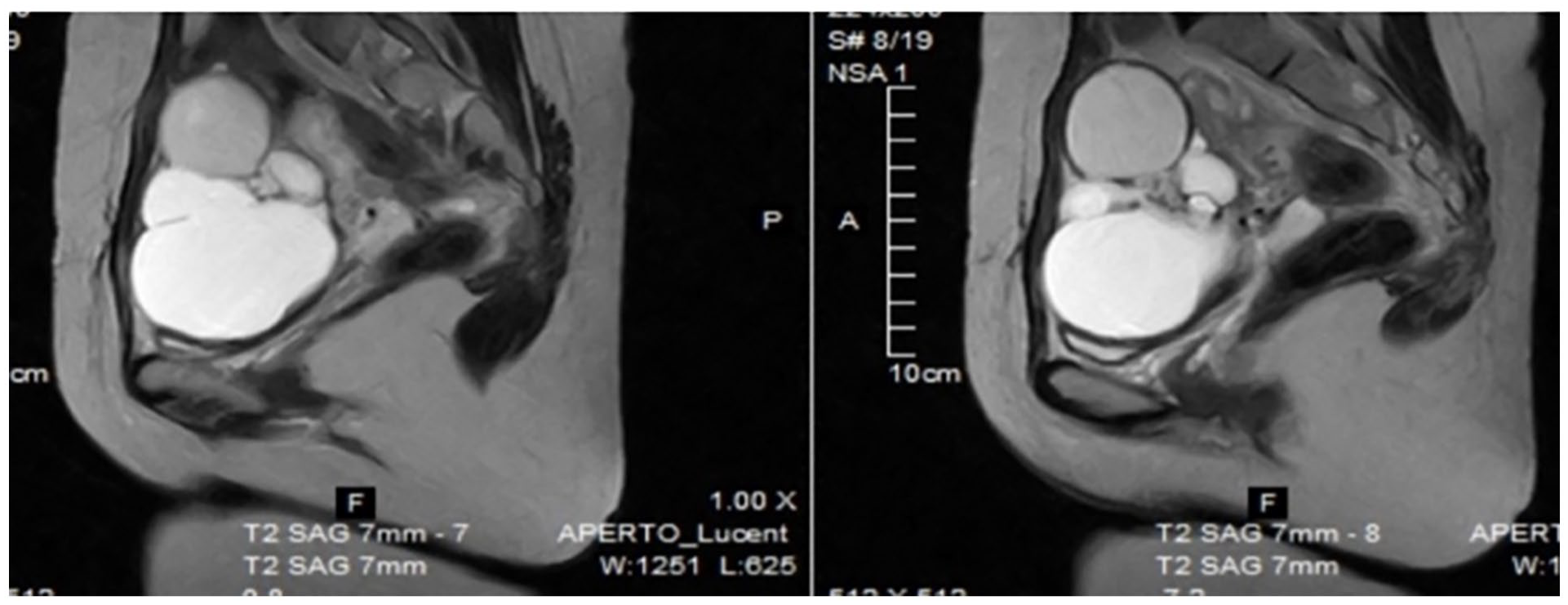
Multicystic tumor with solid component and multilobulated surface on the left ovary: low signal intensity on T1-weighted image and very low intensity on T2-weighted images corresponding to gelatine colloid material.
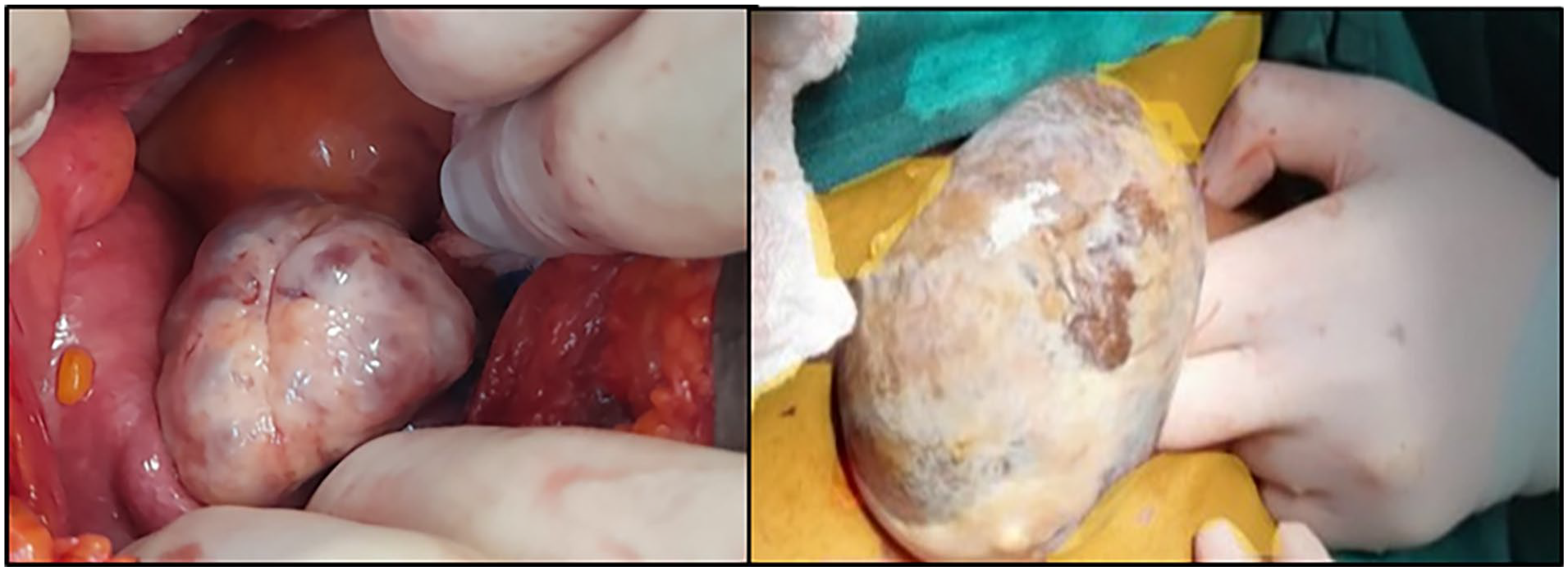
Considering these findings, the patient subsequently underwent a laparotomy and left adnexectomy. During surgery, a smooth-walled left ovarian mass measuring approximately 10 cm was excised with ovary (Figure 2). The examination revealed no signs of capsular invasion or peritoneal spread, and both the uterus and the right ovary appeared normal (Figure 3).
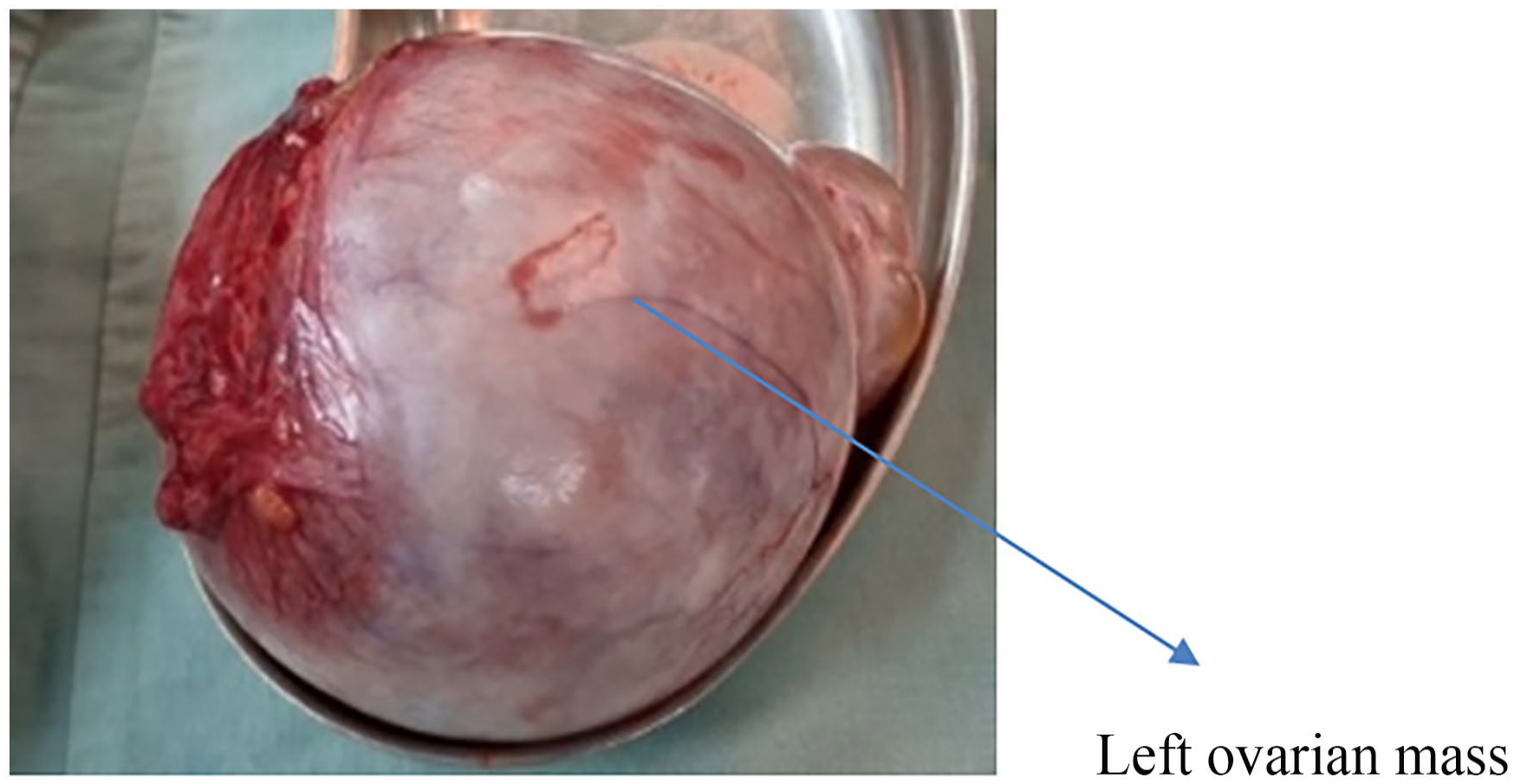
Left ovarian mass measuring approximately 10 cm was excised with ovary.
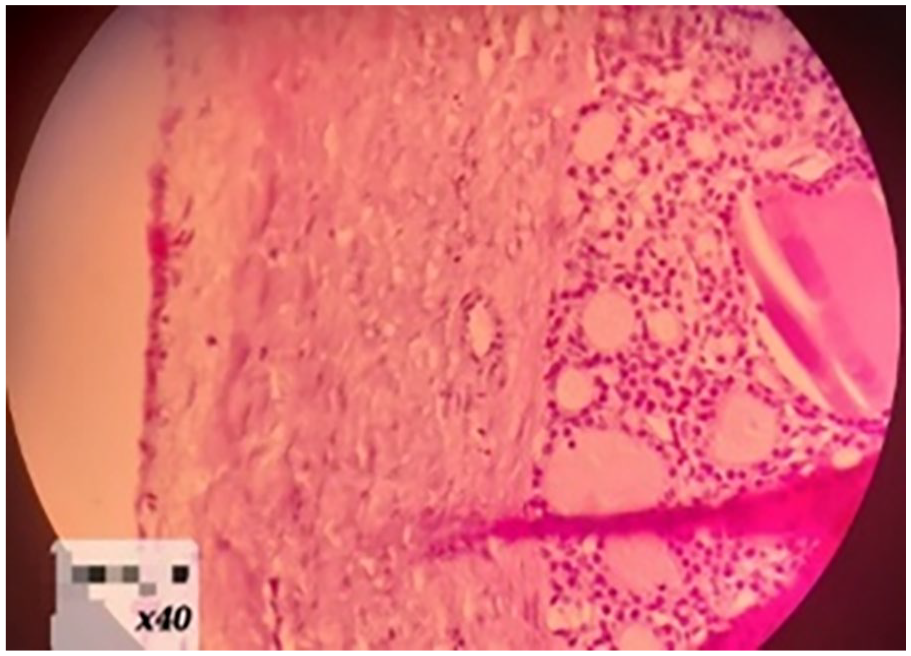
Histology shows thyroid follicles, some of which were filled with colloid.
Histological analysis revealed that the ovarian tumor consisted of multiloculated cysts filled with gelatinous, brown, mucinous material. Microscopy showed that the mass predominantly contained thyroid follicles, some of which were filled with colloid. No malignant features were observed. Immunohistochemical staining was positive for thyroglobulin and thyroid transcription factor-1 (TTF-1), confirming a diagnosis of struma ovarii, a rare ovarian tumor characterized by the presence of thyroid tissue. This diagnosis highlighted the unusual nature of the tumor and its thyroid-like biochemical activity within the ovary (Figure 3). Indeed, the symptoms presented by our patient can mimic several conditions, including, leiomyomas, endometriosis, polycystic ovary syndrome (PCOS), and ovarian cancer, which can further lead to misdiagnosis. Nonetheless, after careful consideration, ultrasounds, MRI, and the histopathological analysis converged on a different diagnosis of an extremely rare condition: struma ovarii.
Challenges in surgical management
The surgical management of struma ovarii is particularly challenging due to its rarity and the potential for misdiagnosis as malignant ovarian tumors. Ensuring the preservation of the patient’s fertility while removing the tumor effectively requires meticulous surgical planning. The complexity of the tumor, with its gelatinous content and multilobulated structure, posed additional difficulties in achieving complete resection without spillage, which could lead to complications. Histological analysis revealed that the ovarian tumor consisted of multiloculated cysts filled with gelatinous brown mucinous material. Microscopy showed that the mass predominantly contained thyroid follicles, some filled with colloid, with no malignant features observed. Immunohistochemical staining was positive for thyroglobulin and TTF-1, confirming a diagnosis of struma ovarii, a rare ovarian tumor characterized by the presence of thyroid tissue.
The symptoms presented by the patient can mimic several conditions, including leiomyomas, endometriosis, PCOS, and ovarian cancer, leading to potential misdiagnosis. However, careful consideration of ultrasounds, MRI, and histopathological analysis converged on a diagnosis of struma ovarii, an extremely rare condition (Figure 3).
Case 2
A 33-year-old female patient presented to the emergency department with progressive abdominal pain localized in the lower quadrants. She has no significant medical or surgical history and has never been hospitalized. Her alcohol consumption is occasional; she does not smoke and reports no known allergies to food or drugs. The physical examination revealed no abnormalities, including absence of pallor, jaundice, or edema, and she exhibited no urinary or gastrointestinal symptoms. Her menstrual cycle was regular with pain during the cycle, without excessive or intermenstrual bleeding, and she had not ingested any recent medications that could account for her symptoms.
A comprehensive physical examination was performed before further investigations. On abdominal examination, the abdomen was soft, non-tender, and non-distended. During the pelvic examination, everything appeared normal from the vulva. The patient was nulliparous (verge), and there were no abnormal findings.
Upon admission, laboratory tests indicated mild anemia and leukopenia. Her hemoglobin level was recorded at 11.5 g/dL, slightly below the normal range of 12–18 g/dL, and her hematocrit was 36.0%, marginally below the normal range of 37%–52%. Her white blood cell count was slightly reduced at 4.05 × 103/μL, compared to the normal range of 4.5–10.5 × 103/μL. The differential count showed elevated lymphocytes at 52.8%, exceeding the normal range of 15%–40%, and monocytes were also elevated at 7.7%, surpassing the normal range of 1%–6%. Other hematological parameters, including the red blood cell count and indices, were within normal limits or slightly altered but not of clinical significance. Gynecologically, the patient reported no abnormal vaginal discharge or uterine bleeding. Her menstrual cycle was regular, without excessive or intermenstrual bleeding, and she had not ingested any recent medications that could account for her symptoms.
A computed tomography (CT) scan of the abdomen was performed in order to rule out the possibility of any neoplasm. The results showed the presence of a 9.7-cm mature ovarian teratoma located in the right iliac region. The liver appeared normal in both size and texture, without any focal lesions, although there were calcifications in the hepatic parenchyma (Figure 4). Additionally, several enlarged mesenteric lymph nodes were observed in the right iliac region, with adjacent edematous fat stranding suggestive of inflammation or a secondary infection. The gastrointestinal tract’s opacified sections showed no notable abnormalities. While appendiceal appendicoliths were detected, there was no sign of renal hydronephrosis or obstructive stones.
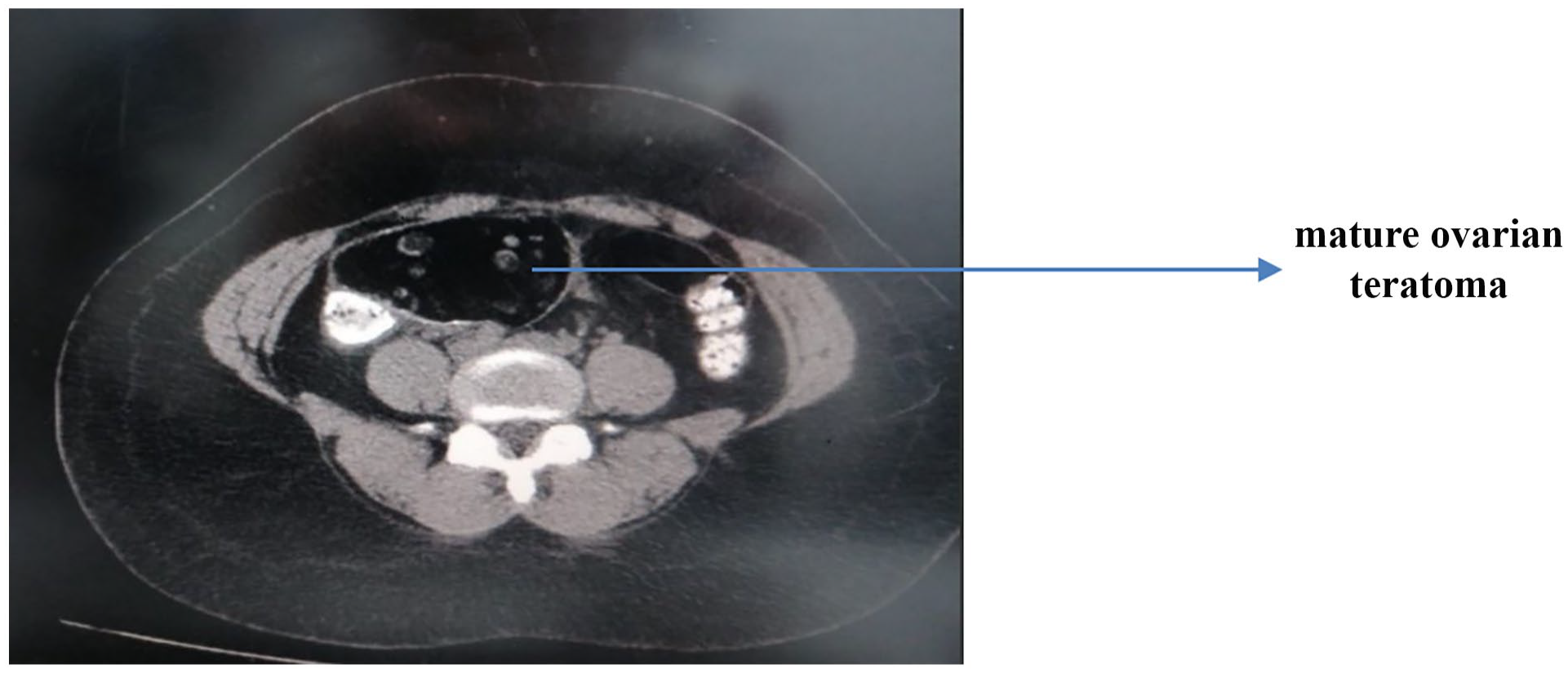
Computed tomography scan presents 9.7-cm mature ovarian teratoma in the right iliac region.
To investigate the possibility of Crohn’s disease, a colonoscopy was conducted. It revealed a congested internal hemorrhoid and an ulcerated, edematous ileocecal valve. Apart from these findings, the rest of the colon appeared normal.
The patient was subsequently scheduled for a right oophorectomy in order to remove the mature ovarian teratoma. During the operation, the exploration of the abdomen revealed a large closed cyst with a fibrotic wall and focal calcifications that were hard to the touch, interspersed within the right ovarian tissue. The cyst, which contained reddish fluid, was floating freely in the abdomen without any attachments. This condition and operative findings were documented in Figure 5.
The cyst (11 × 9 × 7.5 cm), which contained reddish fluid, was floating freely in the abdomen without any attachments.
During the surgical procedure, it was noted that the utero-ovarian ligament was fibrotic and calcified and had detached from its origin at the uterine wall which is suggests an unusual case of ovarian auto-cystectomy.
The excised mass was identified as a dermoid cyst, weighing 240 g and measuring 11 × 9 × 7.5 cm. It was lined with benign squamous epithelium and filled with keratin deposits, with teeth visible on its surface, indicative of its teratogenic origin. Importantly, there was no evidence of malignancy. Cytology of the fluid surrounding the cyst further confirmed the absence of malignant cells. The smears were sparsely cellular, containing a few lymphocytes, rare neutrophils, and red blood cells, with no mesothelial cells or atypical cells detected.
In the pathology report, the specimen was described as hard to the touch, with numerous teeth conspicuously scattered across its surface. The report detailed the presence of keratin deposits, characteristic of dermoid cysts. These findings emphasize the complex nature of the specimen, underlining the teratomatous origin of the cyst, which is lined by benign squamous epithelium and contains diverse tissue elements such as teeth and keratin.
Challenges in surgical management
The surgical management of mature teratomas is challenging due to the risk of spillage and potential complications such as chemical peritonitis. Ensuring the complete removal of the cyst without rupture was crucial. The presence of calcifications and the fibrotic nature of the cyst wall added complexity to the procedure, requiring careful dissection. The excised mass was identified as a dermoid cyst weighing 240 g and measuring 11 × 9 × 7.5 cm. It was lined with benign squamous epithelium and filled with keratin deposits, with teeth visible on its surface, indicative of its teratogenic origin. Importantly, there was no evidence of malignancy. Cytology of the fluid surrounding the cyst further confirmed the absence of malignant cells. The smears were sparsely cellular, containing a few lymphocytes, rare neutrophils, and red blood cells, with no mesothelial cells or atypical cells detected.
In the pathology report, the specimen was described as hard to the touch with numerous teeth conspicuously scattered across its surface. The report detailed the presence of keratin deposits characteristic of dermoid cysts, underlining the teratomatous origin of the cyst, which was lined by benign squamous epithelium and contained diverse tissue elements such as teeth and keratin.
Case 3
A 52-year-old woman, para 3+0 (3 alive), with a history of normal deliveries and menopause onset three years ago, reported no significant weight loss or other systemic symptoms and was not taking any chronic medications.
She presented for her annual screening, noting normal daily activity except for occasional pelvic pressure and pain upon defecation. There were no urinary symptoms reported.
Her LMP was 3 years ago, marking the onset of menopause. Menopause refers to the time in a woman’s life when her menstrual periods permanently stop, and she is no longer able to conceive naturally. It is diagnosed after 12 consecutive months without a menstrual period. The average age of menopause is 51, but it can occur in a woman’s 40s or 50s. Symptoms associated with menopause can include hot flashes, night sweats, mood changes, and vaginal dryness, but it is also marked by the end of menstrual cycles.
Her mammography was negative, and her Pap smear showed no intraepithelial lesion or malignancy but did note menopausal atrophy. The physical examination was unremarkable, featuring a soft, non-tender, and non-distended abdomen, with no signs of pallor, jaundice, or edema. She had previously undergone a splenectomy at age twenty following a spleen rupture due to a road traffic accident.
During the pelvic examination, the vagina and cervix appeared atrophic. The uterus was moderately enlarged for her age, resembling a fibroma uterus, and the patient experienced pain on the left side. The left ovary was increased in volume, raising suspicion of a mass, while the right ovary was normal. There was no tenderness on examination.
Pelvic ultrasonography revealed the uterus as normal in size with a regular contour, though it exhibited a heterogeneous appearance due to the presence of two small subserosal fibroids. The endometrial thickness was thin, and the myometrium appeared homogeneous. The right ovary was normal in both size and echotexture. However, the left ovary was not visible; instead, a tubular-shaped mass measuring 5 × 2 cm, filled with ground glass content, was identified in its expected location, showing moderate vascularity on color Doppler examination. No fluid was detected in the cul-de-sac.
This complex presentation underscores the intricate nature of diagnosing and managing pelvic masses, particularly when they mimic symptoms of common gynecological conditions but present with atypical underlying pathologies.
Given these findings, an MRI was recommended to provide further details and assist in the comprehensive assessment of the abnormal mass. The MRI revealed a normal-sized uterus measuring 5.8 × 5.5 cm, with a 1.3-cm subserosal nodule on the superior myometrial wall. This mass appeared isosignal on T2-weighted images and hyposignal on T1 and Short Tau Inversion Recovery (STIR) images, with post-contrast enhancement characteristics similar to those of the surrounding myometrium, suggestive of a fibroid. Additionally, one smaller intramural nodule, each under one centimeter, was identified on both sides of the uterus, also indicative of fibroids. The endometrium was regular, with normal thickness and signal intensity, measured at 2 mm. The junctional zone was of normal thickness. In the left ovary, a 4.5 × 3.6 cm multilobulated mass was observed, mostly suggestive of a tumoral lesion. A similar, smaller lesion measuring 7 mm was noted in the right ovary.
Furthermore, multiple lesions were found in the pouch of Douglas, with the largest measuring 2.7 × 0.8 cm. These findings raise the possibility of mesenteric carcinomatosis, which would require further investigation. These lesions were hypervascular on the arterial phase, showing strong and heterogeneous enhancement; the largest one exhibited serpiginous-like arterial enhancement, progressing to homogeneous signal intensity on venous and late phases. Additionally, mild free fluid was observed in the pelvis and pouch of Douglas, which may be indicative of an inflammatory or neoplastic process and warrants further evaluation.
On the upper abdomen, the native spleen was notably absent. Tumor markers CA 125 and CEA were checked, resulting in values within normal ranges and not indicative of malignancy (see Figure 6).
Low signal intensity on T1 weighted image and very low intensity in T2 weighted images corresponding to gelatine colloid material.
Under general anesthesia, with appropriate surgical preparations including supine positioning, scrubbing, draping, and Foley catheter placement, a midline incision was made. The incision was deepened layer by layer until the abdominal cavity was accessed. A vascularized lesion was identified on the left anterior uterine wall, and multiple blue peritoneal implants were observed throughout the pouch of Douglas, posterior uterine wall, and multiple perirectal extrafascial areas.
A frozen section biopsy of these lesions indicated that they were benign splenic tissue. The patient underwent a detailed surgical evaluation and treatment for multiple pelvic conditions. The surgical team proceeded with a total abdominal hysterectomy (TAH) and bilateral salpingo-oophorectomy (BSO), excising all identified lesions around the rectum and pouch of Douglas. Hemostasis was successfully achieved, and a drain was placed in the pouch of Douglas before the surgical site was closed in layers. The patient was then transferred to the recovery room in a stable condition and had a smooth postoperative course. The drain was removed, and the patient was subsequently discharged home (refer to Figure 6).
Pathological examination of the uterus revealed an unremarkable cervix, an atrophic endometrium, and intramural leiomyoma. Both the uterus and broad ligaments displayed serosal implantations of nodular splenic tissue. Additionally, multiple nodules of splenic tissue were found on the small bowel’s serosa, confirming a diagnosis of peritoneal splenosis.
Challenges in surgical management
The surgical management of peritoneal splenosis is particularly challenging due to its ability to mimic metastatic disease. Differentiating splenic implants from malignant lesions intraoperatively requires careful examination and often intraoperative consultation with pathology. Achieving a balance between removing suspicious lesions and preserving healthy tissue is crucial. A frozen section biopsy of these lesions indicated that they were benign splenic tissue. The patient underwent a detailed surgical evaluation and treatment for multiple pelvic conditions. The surgical team proceeded with a TAH and BSO, excising all identified lesions around the rectum and pouch of Douglas. Hemostasis was successfully achieved, and a drain was placed in the pouch of Douglas before the surgical site was closed in layers. The patient was then transferred to the recovery room in a stable condition and had a smooth postoperative course. The drain was removed, and the patient was subsequently discharged home (Figure 6).
Pathological examination of the uterus revealed an unremarkable cervix, an atrophic endometrium, and intramural leiomyoma. Both the uterus and broad ligaments displayed serosal implantations of nodular splenic tissue. Additionally, multiple nodules of splenic tissue were found on the small bowel’s serosa, confirming a diagnosis of peritoneal splenosis.
These findings emphasize the complex nature of diagnosing and managing pelvic masses, particularly when they mimic symptoms of common gynecological conditions but present with atypical underlying pathologies.
Discussion
Struma ovarii, first reported by Boettlin in 1889, is an exceptionally rare tumor whose pathogenesis is uncertain. According to the World Health Organization, thyroid tissue must replace at least 50% of the ovary. 6 Teratomas account for 1%–12% of all ovarian tumors, with 0.6% containing thyroid tissue zones and only 0.4% being struma ovarii. Other studies have reported that 15% of ovarian teratomas contain non-significant thyroid tissue, of which only 0.8% is struma ovarii. Neoplastic transformation occurs in only 5% of all cases. The malignant struma ovarii was first described by Wetteland in 1956.7–9 The diagnosis of struma ovarii exemplifies the rarity and diagnostic ambiguity of this condition. It is a highly specialized form of mature teratoma predominantly composed of thyroid tissue, making up about 2%–3% of all ovarian teratomas.10,11 Despite its generally benign nature, approximately 5%–10% can exhibit malignant features or functional thyroid symptoms, complicating the clinical picture. 2 The literature underscores the importance of recognizing this entity to avoid misdiagnosis and inappropriate treatment. 12 It is difficult to distinguish between struma ovarii and ovarian carcinoma preoperatively as the symptoms and images on ultrasound are often similar. An ovarian cyst with a large solid component on ultrasound may raise suspicions of struma ovarii. Nurliza Binti et al. 13 recommend using MRI and serum thyroglobulin to preoperatively diagnose struma and then proceed to a laparoscopic procedure. If struma ovarii is suspected, thyroid functions should be tested. I-131 scintigraphy can be used to confirm the presence of ovarian thyroid tissue and locate metastatic disease. 14 As the diagnosis of struma ovarii is usually made postoperatively, in our case, unilateral salpingo-oophorectomy is adequate in women who wish to retain fertility, and this would be the definitive treatment in benign disease.
Mature teratoma
The second case illustrates the diagnostic and management challenges associated with mature teratomas, which are the most common benign ovarian tumors, accounting for 15%–20% of all ovarian neoplasms. 2 These tumors can present with a wide range of symptoms, from being asymptomatic to causing acute abdominal pain due to complications like torsion or rupture. 15 The diagnosis is typically made through imaging, with ultrasound being the preferred modality. However, CT and MRI can also be diagnostic. 16 In our patient, a CT scan incidentally discovered the teratoma during evaluation for acute appendicitis. Surgical management through oophorectomy is crucial to prevent complications and ensure complete removal to avoid recurrence. Histological examination is essential to confirm the diagnosis and rule out malignancy. This case highlights the need for vigilance in the evaluation of ovarian masses and the potential for incidental findings during imaging for other conditions. Dermoid cysts, or mature cystic teratomas, generally grow slowly, with an average growth of 1.8 mm/year in premenopausal women. 17 Their diameter can range from less than 1 cm to 10 cm; however, their size does not reflect their malignant potential. 18 The vast majority of these cysts are asymptomatic unless secondary to complications like torsion, abdominal pain, distention, infection, vaginal bleeding, nausea, vomiting, and rupture. 15
Peritoneal splenosis
The third case emphasizes the diagnostic challenges posed by peritoneal splenosis, a condition resulting from the autotransplantation of splenic tissue following splenic trauma or surgery. This condition is often asymptomatic but can mimic metastatic cancer on imaging studies. 4 In our patient, the diagnosis was complicated by the incidental finding of splenic tissue during routine screening. MRI played a pivotal role in differentiating splenosis from other gynecological conditions, as splenosis implants exhibit signal characteristics similar to normal splenic tissue. 19 Recognizing the arterial enhancement pattern on MRI is crucial for diagnosis. The management of splenosis is typically conservative unless the patient is symptomatic, in which case surgical intervention may be necessary. This case underscores the importance of considering splenosis in the differential diagnosis of pelvic masses in patients with a history of splenic trauma or surgery to avoid unnecessary interventions. Pelvic splenosis commonly presents with pelvic pain or pelvic mass. 4 On MRI, splenosis implants show homogenous hypointensity on T1 weighted imaging and hyperintensity on T2 weighted images. 4 They also display an arterial heterogeneous/serpiginous enhancement pattern with progressive homogenization during dynamic studies. 4
Comparison with literature
The cases in this series underscore the necessity for careful differentiation between benign and malignant ovarian masses. The literature highlights that benign conditions like struma ovarii and mature teratomas can present with imaging characteristics similar to malignant tumors.1,3 Peritoneal splenosis is often misdiagnosed as a neoplastic process due to its radiological appearance, emphasizing the need for comprehensive evaluation and a high index of suspicion. 20
Implications for management
Effective management of ovarian masses requires integrating clinical, radiological, and surgical insights. Surgical intervention often provides definitive diagnosis and facilitates appropriate management. Pathological analysis is crucial in guiding the extent of surgical intervention to avoid overtreatment of benign conditions while ensuring optimal patient outcomes.1,12 Multidisciplinary care is essential in managing these complex cases.
Limitations
The case reports did not provide detailed follow-up information on all patients. This is a limitation, as long-term outcomes and potential recurrence are crucial for comprehensive case understanding and management planning.
Conclusion
This case series reinforces the complex nature of diagnosing ovarian masses, advocating for a meticulous approach that combines clinical evaluation, sophisticated imaging techniques, and judicious surgical exploration. These cases contribute to the broader medical literature by delineating clear examples of how benign conditions can mimic more serious pathology and the strategies employed to manage them effectively, avoiding unnecessary interventions while ensuring optimal patient outcomes.
Footnotes
Acknowledgements
None.
Author contributions
The study was designed, implemented, written, and presented for publication by K.G., H.B., and G.Y. J.H., Z.M., K.D., and C.E.H. made supervision for the manuscript. H.N., M.E.J.E.K., and C.M. enhanced the quality of the paper making it more professional.
Data availability statement
The data supporting the findings of this study are available upon request from the corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval to report this case was obtained from Rafik Hariri University Hospital by Dr. Georges Yared. Due to the unprecedented crisis in our country (Lebanon), formal ethical approval was not obtainable; however, all procedures performed in the study adhere to the ethical standards of the 1964 Declaration of Helsinki and its later amendments, with informed consent obtained from the patient for publication of this case report, ensuring the protection of confidentiality and privacy.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Trial registration
None.
Guarantor
I, Dr. Kariman Ghazal, am willing to take full responsibility for this article, including the accuracy and appropriateness of the reference list.