
Abstract
Coexistent aneurysmal involvement of common iliac artery is frequently seen in patients with infrarenal abdominal aortic aneurysm. Bilateral iliac branch devices are an option to preserve bilateral internal iliac arteries in order to decrease the risk of buttock claudication. In Asian population, however, the aortoiliac lengths are commonly not adequate for bilateral iliac branch endoprosthesis. In this technical note, we use a novel hybrid technique to preserve bilateral internal iliac arteries in a patient without adequate aortoiliac length for bilateral iliac branch endoprosthesis. The right internal iliac artery is preserved with iliac branch endoprosthesis. The left internal iliac artery is preserved with cross-over chimney stent grafts which are deployed simultaneously with the parallel grafting of iliac extension from the contralateral gate to the right iliac branch endoprosthesis. Follow-up computed tomography and three-dimensional angiography showed complete aneurysm exclusion with flow preservation to bilateral internal iliac arteries.
Keywords
Introduction
Iliac branch endoprosthesis (IBE) with aortic endovascular repair (EVAR) has been accepted as an alternative for treating aortoiliac aneurysms (AIA). The anatomical criteria are challenging if bilateral IBEs are planned, especially in patients with short distance between the lowest renal artery and common iliac artery (CIA) bifurcation. 1 In the present case, we performed a novel hybrid approach with IBE and cross-over parallel chimney graft in a patient with AIA with bilateral CIA aneurysm to preserve bilateral internal iliac arteries (IIA).
Case-presentation
We present a case with written informed consent. This 82-year-old Asian man with hypertension and a 3.5 cm infrarenal abdominal aortic aneurysm (AAA) with bilateral CIA aneurysms (CIAA, right: 37 mm, left: 28 mm) was indicated for endovascular AIA repair. The aortic centerline analysis showed short bilateral aortoiliac lengths from the lowest renal artery to external iliac artery (EIA) and IIA bifurcation (right = 164 mm, left = 167 mm), which was common in Asian population.2,3 This anatomy made bilateral GORE® EXCLUDER® IBE (W.L.Gore & Associates, Inc. Phoenix, AZ) to preserve both IIA infeasible (Figure 1). The patient was planned for a hybrid technique to preserve bilateral IIAs.4,5 The GORE® EXCLUDER® IBE device was loaded into the aortic wire and the preloaded through-and-through wire. It was delivered through a 16F sheath into the right CIA. After deployment of the IBE device, a 12F sheath was inserted from the left femoral artery and advanced over the through wire into the internal iliac gate. The internal iliac component was advanced into the right IIA, followed by the deployment of both internal iliac component and the remaining external iliac limb. Before the delivery of the GORE® EXCLUDER® AAA device via left femoral artery, a second access was punctured in the right femoral artery and a cross-over wire was advanced into the left IIA with an 8F sheath. The remainder of repair was completed with an Excluder bifurcated main body via the left femoral artery and the ipsilateral iliac limb was extended to the left EIA. The cross-over chimney stent grafts were deployed 2 cm inside the left IIA with two Viabahn self-expandable covered stents telescoping each other and extended to the proximal end of right IBE. These two cross-over stent grafts were simultaneously deployed with parallel 27 mm iliac extension from the contralateral gate of the Excluder bifurcated device to the right IBE of which the proximal diameter is 23 mm (Figure 2). Follow-up computed tomography (Figure 3) and three-dimensional angiography (Figure 4) 10 days after the procedure showed complete aneurysmexclusion with flow preservation to bilateral IIAs. At one-year clinical follow-up, this patient had no symptoms of buttock claudication.Computed tomography (CT) scan at 16 months after the surgery showed that the stent grafts are all patent, and the flow to the bilateral internal iliac artery is preserved. There is no endoleak or stent migration. At 2 years, a CT scan revealed the patent cross-over chimney stent (Figure 5).

From the aortic centerline analysis, the patient had short bilateral aortoiliac lengths from the lowest renal artery to external iliac artery and internal iliac artery bifurcation (right = 164 mm, left = 167 mm).
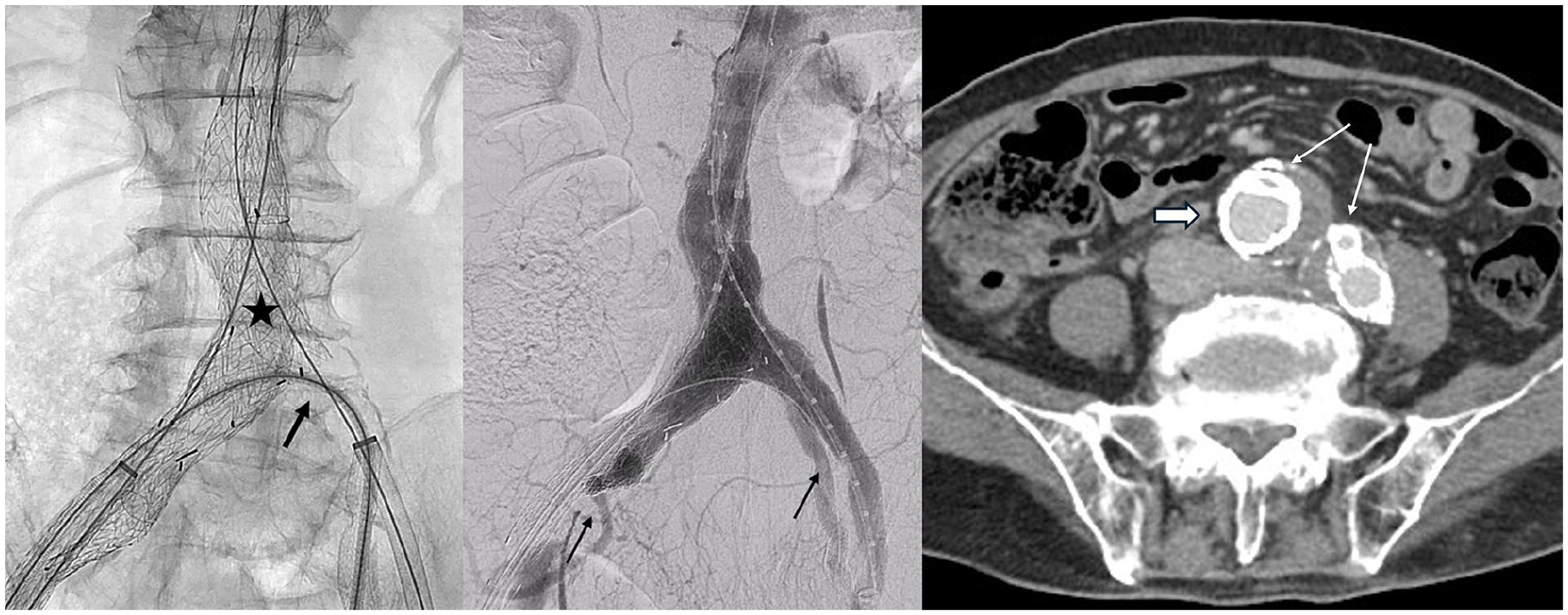
Two cross-over chimney stent grafts (thick black arrow) were deployed simultaneously with the iliac limb extension stent (star) and parallel grafting at the proximal end of iliac branch endoprosthesis. The postoperative angiography showed patent bilateral internal iliac arteries (thin black arrow). On the axial view of the computed tomography scan, one end of the cross-over chimney stent grafts (thin white arrow) was deployed within the proximal end of right iliac branched device (thick white arrow). The other end was deployed parallel to the ipsilateral left iliac limb extension stent (thin white arrow).
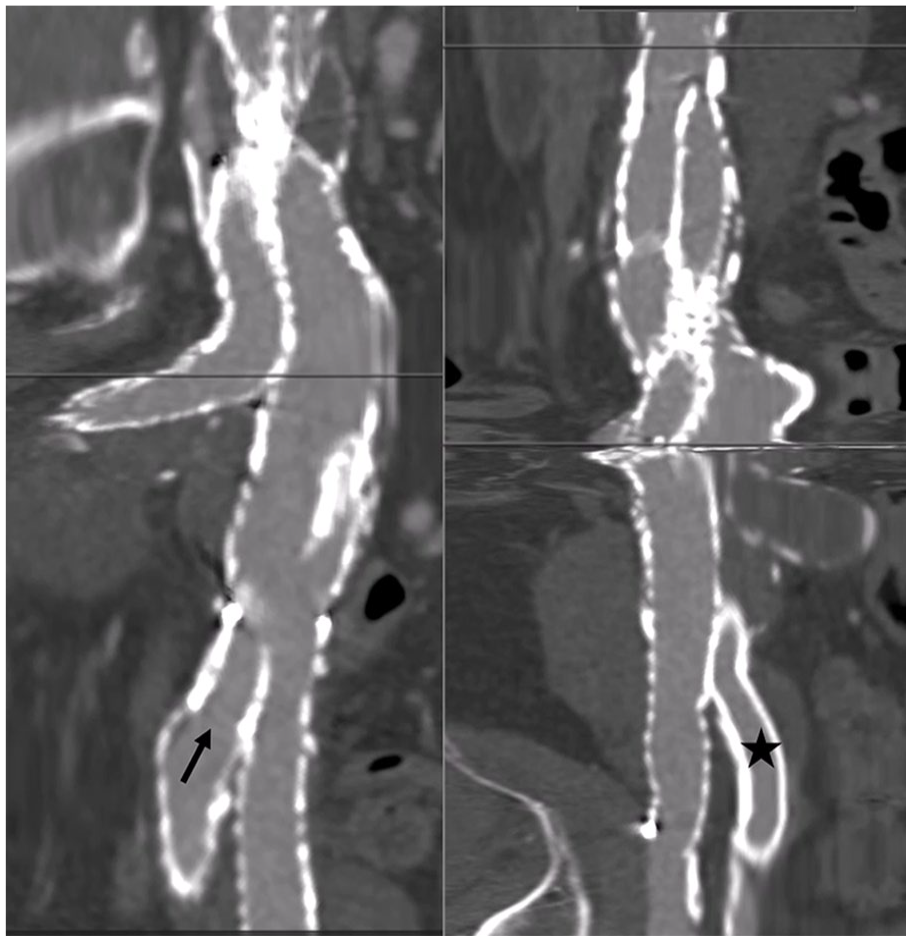
Computed tomography showed patent right internal iliac artery (arrow) from the iliac branch device and patent left internal iliac artery (star) from the cross-over chimney stent grafts.

Computed tomographic angiography showed the morphology of cross-over chimney grafts (star) and the parallel graft with the iliac branch device (arrow).

Computed tomography showed the patent cross-over chimney stents (thick arrow) 2 years after the surgery.
Discussion
Coexistent aneurysmal involvement of CIAs is seen in up to 40% of patients with AAA. 6 It is generally agreed that preservation of flow into at least one IIA is recommended. However, in a recent publication, in patients with bilateral CIA aneurysms, the risk of postoperative buttock claudication can be further decreased with both IIA preservation if patients are anatomically suitable for bilateral IBEs, and excellent results have been achieved with the bilateral IBE.5,7 Several techniques for the preservation of IIA flow have been developed, including the open EIA to IIA bypass, sandwich chimney grafts, and iliac branched devices.
Anatomic criteria for implantation of bilateral IBEs per instruction for use are challenging. Longer distances up to 195 mm and 205 mm from lowest renal artery to CIA bifurcation were required as the bridging stent will dock within the longer ipsilateral limb of the Gore Excluder main body device. The distance between the lowest renal artery and the CIAs bifurcation, the length, and width of CIAs were significantly shorter in Asians compared to Caucasians in this case.1–3 In the report from Li et al, less than half of Eastern Asian patients with AIAs were eligible for IBEs, and the suitability was significantly lower in bilateral CIAAs than in unilateral CIAAs. 3 Therefore, the combination of parallel cross-over chimney graft with the IBEs device to eliminate the anatomic limitation of bilateral IBEs to preserve bilateral IIAs is attractive in this case.
Conclusion
In Asian patients with AIA, short aortoiliac lengths are common. To preserve bilateral IIA, an iliac branch device with a parallel cross-over stent graft is a novel and feasible technique.
Footnotes
Author contributions
I.H.W. conceived of and carried out the presented idea. I.H.W. and S.H.Y. contributed to the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval to report this case was obtained from the institutional review board of the National Taiwan University Hospital Ethics Committee (201410080RINA).
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.