
Abstract
A 41-year-old female who underwent right-sided styloidectomy via tonsillectomy approach experienced refractory short-lasting severe secondary haemorrhage on the third, seventh and thirteen postoperative days. On examination under general anaesthesia, no major vessel injury was noticed. Contrast-enhanced computerized tomography scan of the neck was done because no obvious bleeder was seen and refractory nature of bleeding. Contrast-enhanced computerized tomography scan neck showed pseudoaneurysm of facial artery which was managed with endovascular embolization successfully.
Introduction
Tonsillectomy is the most common throat surgery performed by otorhinolaryngologists in most of the countries including India. 1 It is one of the most common surgeries performed in the United States.2,3 The most dreaded complication after tonsillectomy is haemorrhage which may be primary (occurs within 24 h of surgery) or secondary (occurs after 24 h). The incidence of post tonsillectomy haemorrhage is 3.9%–6%.1–4 Primary haemorrhage is mainly due to faulty operative technique and coagulopathy. 5 Secondary haemorrhage is due to the separation of the slough from the granulating fossa and is seen after the fifth–seventh postoperative days (POD).2,5,6 Secondary haemorrhage can be seen with arterial dissection or pseudoaneurysm caused by blunt or direct trauma to vessels and placing of ligation suture.2,5 Recalcitrant bleeding despite surgical intervention is one of the great signs of pseudoaneurysm following tonsillectomy/styloidectomy.2,7 In literature, lingual, facial, and external or internal carotid artery pseudoaneurysms are described.5,7 The best treatment for pseudoaneurysm is selective embolization of the concerned artery using different materials like coils.4,5
Case report
A 41-year-old female presented with right-sided tonsillar pain radiating to the ipsilateral neck. On oral examination, a tender and palpable right styloid process is noticed in the right tonsillar fossa. Her computerized tomography neck scan neck demonstrated an enlarged and calcified right styloid process of 44 mm (Figure 1). She underwent right styloidectomy via tonsillectomy approach by cold steel dissection method. Intraoperatively, deep dissection was done to expose the styloid process and there was some difficulty in cutting the styloid process since it was calcified otherwise operation was uneventful. She had bleeding from the oral cavity on the third POD which was small and stopped spontaneously. On 7th POD, she had short-lasting but abrupt and profuse secondary haemorrhage leading to haemorrhagic shock and managed with transfused with 3 units of fresh whole blood. Re-exploration under general anaesthesia, except granulation tissue and minor ooze from breached constrictor, no other major bleeding was seen. She was discharged on the tenth POD. She again came with profuse and short-lasting bleeding from the right side of the oral cavity on 13th POD which was stopped on arrival. She was readmitted and a contrast-enhanced computerized tomography scan (CECT) of the neck was done due to the redcurrant and unusual nature of the bleeding. CECT neck showed contrast-filled dilatation of a branch of the right facial artery in the right palatine tonsillar fossa within the operative bed—likely pseudoaneurysm. She was referred to the centre where endovascular service was available. Pseudoaneurysm which was clearly seen at the bed of the right tonsillar fossa during angiography (Figure 2) was successfully coiled and embolized (Figure 3). After that, the patient did not bleed and was discharged after 2 days. On a 6-month follow-up, the patient was normal.
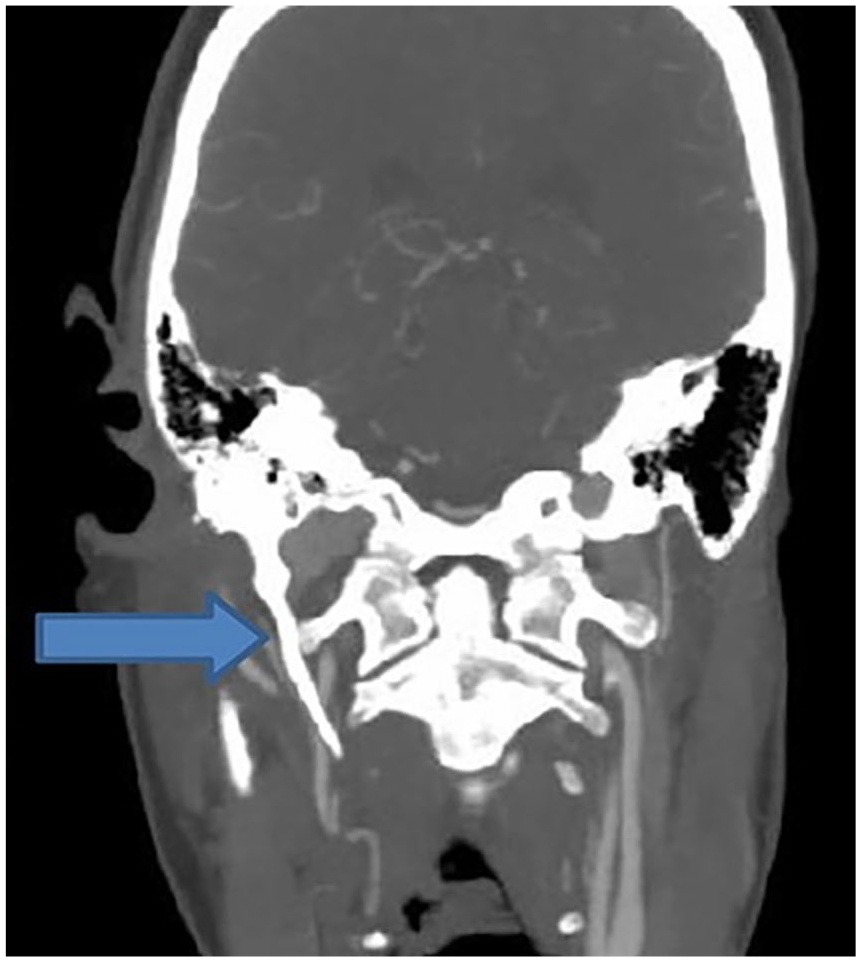
Enlarged right styloid process.

Pseudoaneurysm of the right facial artery.

Pseudoaneurysm of the right facial artery successfully embolized with platinum coil.
Discussion
Haemorrhage is the most common complication following tonsillectomy/styloidectomy. But secondary haemorrhage due to pseudoaneurysm after tonsillectomy is a rare entity.5,6 The risk of haemorrhage increases with age, peaking at 30–34 years with no sex preference. The incidence of serious haemorrhage tends to rise with increasing age 8. Secondary haemorrhage usually occurs between the fifth to tenth postoperative day 9.
Pseudoaneurysm rupture significantly compromises the hemodynamic status of patients8–10 due to significant blood loss. Pseudoaneurysms develop from intraoperative vessel luminal blunt injury from dissection or suturing. This results in vessel wall rupture with subsequent contained bleeding into the local soft tissues that create the pseudoaneurysm 2 which enlarges and ruptures leading to bleeding and subsequent quiescent period. 3 Periods of active bleeding and quiescence repeatedly occur until treated. Many cases of haemorrhage from pseudoaneurysm have presented in the range of 1–3 weeks after tonsillectomy. 5 Lingual artery pseudoaneurysm is more common than the facial artery.2,3,5 In a literature review by Manzato et al. 8 among 23 cases of post-tonsillectomy pseudoaneurysm, two have involved the facial artery. The blood supply of palatine tonsils comes from the descending palatine artery (branch of the internal maxillary artery), the ascending pharyngeal artery, the dorsal lingual artery (branch of the lingual artery), and the ascending palatine artery and tonsillar artery, both originating from the facial artery2,5 (Figure 4). Abnormal blood supply to a tonsil may pose a risk of iatrogenic pseudoaneurysm in the tonsillar bed. 5 The facial artery may have a variable course looping high over the submandibular gland and approaching the posteroinferior tonsillar pole.5,6 The facial artery or even the lingual artery may have an upward course and come close to the inferior tonsillar pole.11,12 These scenarios make that area vulnerable to arterial injury. In our case, angiography did not reveal an aberrant course of the facial artery, and therefore surgical manipulations deeper into the tonsillar fossa during styloidectomy may have caused the injury to the facial artery at the level of the tonsillar artery origin.

Blood supply of palatine tonsil.
Repeated episodes of bleeding should be considered a warning sign of serious post-tonsillectomy haemorrhage. In the presented case, the first bleeding episode occurred on the third POD and then on the 7th and 13 POD days. No active bleeding was seen during oral cavity inspection at any time. Van Cruijsen et al. explained that pseudoaneurysm develops slowly and expands when the periarterial clot dissolves and more blood flows outside the vessel. 13 The size of the injury to the vessel wall might determine the volume of blood in the pseudoaneurysm and whether it will be large enough to be visible. In our case, the injury may have been small thus the pseudoaneurysm grew slowly and was not visible. Lying down in bed might have increased blood pressure in the carotid artery system with subsequent leakage from the pseudoaneurysm. The formation of a new clot at the site of injury would have made the severe short-lasting bleeding stop. 13
There are three treatment options accepted in the literature for late-onset secondary haemorrhage: local manoeuvres, surgical ligature, and endovascular treatment. 8 Surgical ligation of the external carotid artery can be done in emergencies such as life-threatening bleeds or expanding hematomas but this manoeuvre puts cranial nerves at risk of injury, cerebrovascular accident, reduction of vascular reserve in the distribution of the arterial supply to the ligated vessels.11,14 Bleeding can still continue after surgical ligation due to the significant collateralization of head and neck vasculature. 2
Endovascular embolization of pseudoaneurysms is now becoming popular and was first described in 1975. 15 Its use should be encouraged in stable patients because it offers a series of advantages over other procedures: firstly, it is selective, secondly, it is less mutilating and it poses fewer risks to neighbouring structures, such as injuries to the vagus and accessory nerves.5,8,5 Thirdly, diagnostic angiography can be followed by therapeutic embolization during the same surgical intervention.5,12 The materials available for use in endovascular treatment in the head and neck area include coils (platinum), polyvinyl alcohol particles and gelatin sponges. 16 The possible risks of embolization include pain, extravasation of embolic material, inadvertent embolization of other vessels, ischaemic injury to surrounding tissues, arterial vasospasm and the need for further procedures. 1
Conclusion
Diagnosis of post-tonsillectomy secondary haemorrhage due to ruptured pseudoaneurysm of either lingual or facial or external carotid artery needs a high index of suspicion and it should be considered as a differential diagnosis in recalcitrant secondary haemorrhage. One should be very careful while doing deep dissection, excessive cauterization or suture ligation to avoid arterial injury. Endovascular embolization is the safe and effective method to treat this condition with a high success rate and low morbidity.
Footnotes
Acknowledgements
Dr. Muskan Shrestha, our anaesthesiologist. Mr. Binay Uprety, our operation room in-charge.
Author contributions
N.R. operative surgeon; S.P. embolization of pseudoaneurysm.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The ethical approval is not required for the case presentation in our institution.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.