
Abstract
Adult intussusception is rare, and an underlying benign or malignant aetiology is often found. Inflammatory fibroid polyp, a benign neoplastic polyp that can arise anywhere in the gastrointestinal tract is a rare cause of intussusception of the small bowel. Clinical presentation differs depending on the location of the lesion in the gastrointestinal tract. Diagnosis may be confirmed on a computed tomography scan or ultrasound. Definite diagnosis is based on histopathology and immunocytochemistry. We present the case of a 58-year-old lady with an inflammatory fibroid polyp who presented with microcytic anaemia and chronic abdominal pain due to recurrent intussusception.
Introduction
This is the first reported case of inflammatory fibroid polyp (IFP) in the Mauritian population. IFP, a benign neoplastic polyp that can arise anywhere in the gastrointestinal tract, is an uncommon condition. Clinical presentation differs depending on the location, and a definite diagnosis is through histopathology. The mass can act as a lead point for intussusception. Adult intussusception is rare and could arise either because of benign or malignant origin in comparison to the paediatric population where it is often idiopathic. This patient presented with a mass and pain in the lower abdomen, and full blood count results revealed microcytic anaemia. Ultrasound and computed tomography (CT) scan confirmed the presence of a pelvic mass suggestive of an ovarian mass, and a jejuno-ileal intussusception was identified. The patient underwent a laparotomy with small bowel resection and end-to-end anastomosis. The right ovarian mass was also resected. Intra-operatively gross findings showed that the small bowel and the ovary acted as a lead point for intussusception. Histopathological diagnosis revealed the presence of an IFP which arises due to a mutation in the platelet-derived growth factor receptor alpha (PDGFRA) gene which concomitantly occurs in gastrointestinal stromal tumours.
Case presentation
A 58-year-old female was referred with an abdominal mass and lower abdominal pain. She was seen at a peripheral hospital 2 months earlier with microcytic anaemia, and a haemoglobin of 5.3 g/dl, for which she was transfused and discharged home. She has a background history of type II diabetes mellitus and hypertension. She had a hysterectomy and left oophorectomy for a fibroid uterus at the age of 35. On examination, she was tender in the suprapubic region and the rest of the examination was normal. An ultrasound scan (Figure 1) showed a 6 cm mass in the pelvis. She underwent a contrast-enhanced CT scan (Figure 2) of the abdomen and pelvis showing a solid pelvic mass suspected to be the right ovary and a jejuno-ileal intussusception (Figure 3) with a small bowel mass as lead point.
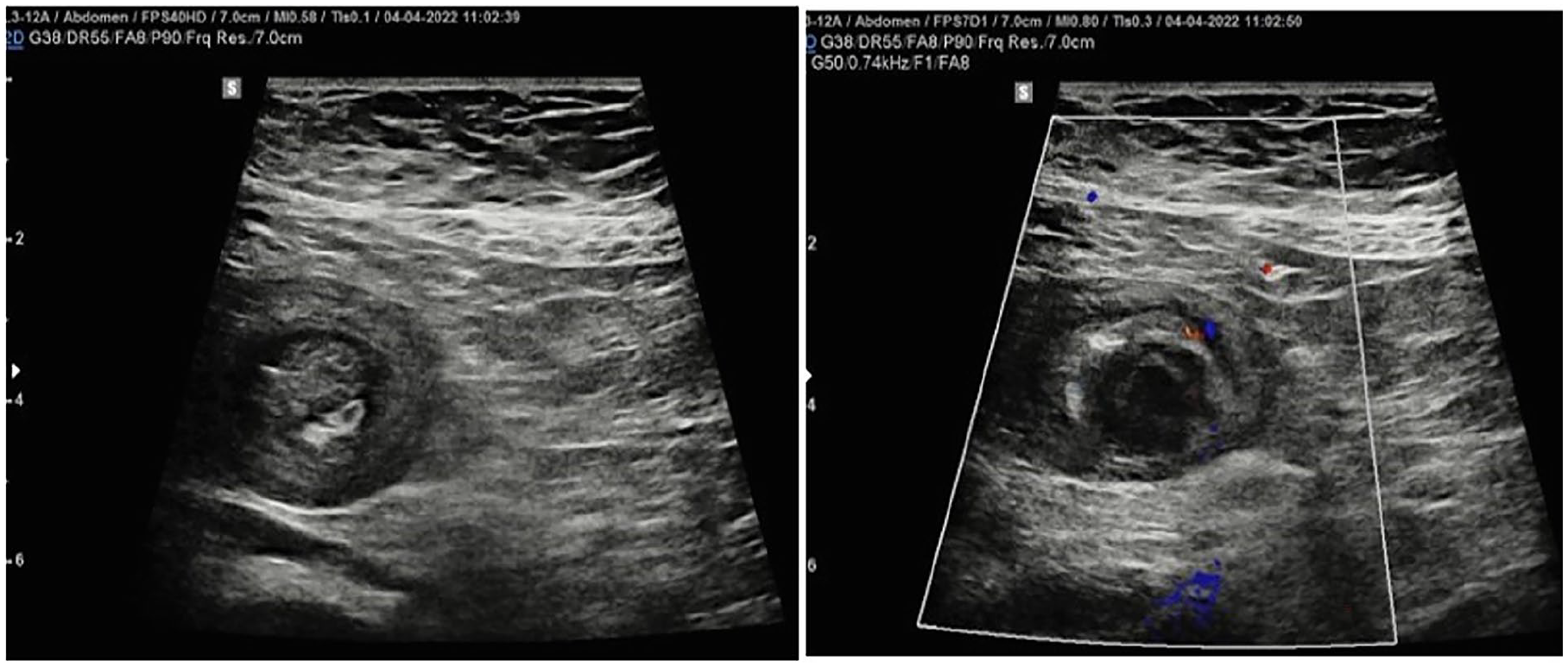
Ultrasound scan shows a target lesion in the mid-abdomen, suggestive of an intussusception with the presence of an intra-luminal, hypoechoic nodular lesion.

CT scan shows the presence of a discrete hypodense polypoid formation in a jejunal loop.

Intraoperative view of the jejunoileal intussusception.
There was no small bowel obstruction. Tumour markers CA125 (cancer antigen 125) and carcinoembryonic antigen were within the normal range. The patient underwent a laparotomy with small bowel resection and end-to-end anastomosis. The right ovarian mass was also resected. The patient had an uneventful recovery and was discharged on the fourth postoperative day. The patient had no further adverse outcome and was well on her follow-up after 2 weeks.
On gross examination within the small bowel intussuscepted (Figure 4) part, a sessile lesion was noted measuring 20 × 15 × 10 mm. Histopathological examination revealed a polypoidal lesion within the submucosa that was poorly marginated. The overlying mucosa displayed foci of ulceration and this hypocellular lesion was made up mostly of short spindled and stellate cells with an oedematous stroma rich in eosinophils and chronic inflammatory cells. Some of the blood vessels admitted showed onion skin fibrosis (Figure 5). The ovarian mass was confirmed as a fibroma. Immunocytochemistry was positive for CD 34 and negative for DOG 1(Discovered On GIST 1) excluding GIST (Figure 6).

Right ovary (left side) and small bowel mass (right side) acting as lead point for intussusception.
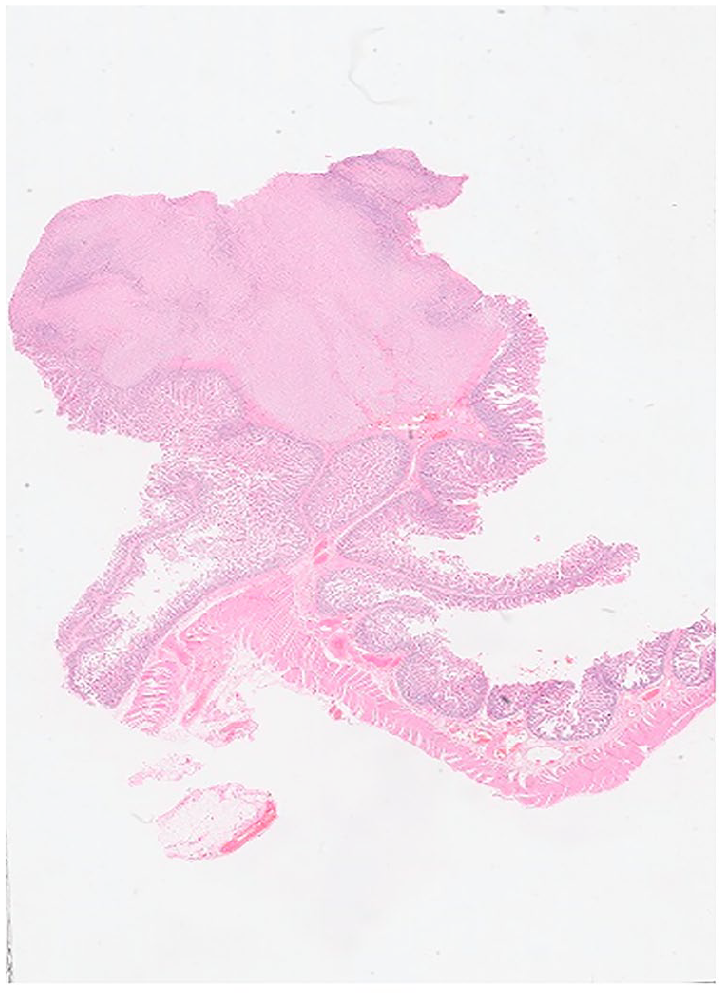
Inflammatory fibroid polyp (Ventana DP 200 Slide Scanner Roche Diagnostics).

On the left image slide was CD 34+ on immunocytochemistry and the right image was DOG 1 (Discovered On GIST 1) negative.
Discussion
Intussusception of the small bowel is defined as the telescoping of a proximal segment of the gastrointestinal tract within the lumen of the adjacent segment. It was first described by Barbette in 1675 and the first surgical intervention was done by Sir Jonathan Hutchinson on a child with intussusception in 1871. 1 Adult intussusception is rare representing only 5% of all cases of intussusception and only 1%–5% of all cases of bowel obstruction in adults. 2 Adult intussusception is a distinct entity from paediatric intussusception. Paediatric intussusception is primary or idiopathic in most cases and is benign. Pneumatic or hydrostatic reduction of the intussusception will suffice in 80% of cases. 3 However, adult intussusception is secondary to a pathologic condition that acts as the leading point. This ranges from benign tumours to carcinomas of the small bowel. Common causes of intussusception in adults include Meckel’s diverticulum, adhesions, hamartomas, lipomas, lymphoid hyperplasia and tuberculosis.3,4 In this patient IFP was causing anaemia due to occult bleeding and intermittent intussusception causing subacute bowel. Thus, definite treatment would be primary bowel resection to identify the cause and relieve the obstruction.
IFP is a benign polypoid lesion first described by Vanek in 1949 as an eosinophilic submucosal granuloma. 4 IFPs are rare and there is a slight female preponderance with a peak incidence in middle-aged adults. The antrum of the stomach is the most affected site (66%–75%), followed by the ileum (18%–20%) although IFPs may arise throughout the gastrointestinal tract. 5 Tumours are usually centred in the submucosa but can be restricted to the mucosa.
IFPs can be both sporadic and familial. Both forms have been associated with mutations in the PDGFRA gene. Previously Gastrointestinal Stromal Tumours (GIST) were the only known PDGFRA mutant gastrointestinal tumours. 6 Familial IFPs show a mutation of the c.1664A>G variant. In the sporadic form exon 18 mutations usually c.2525A>T predominate in gastric tumours while exon 12 mutations are more commonly identified in small intestine tumours. 7 Other risk factors for IFPs include trauma, allergic reaction, bacterial infection, and physical and chemical irritants. 8
The clinical picture depends on the size and site of the tumour. Most tumours are found incidentally due to their small size. Gastric tumours can present with epigastric pain, nausea and vomiting. Small bowel tumours most commonly present with chronic abdominal pain and obstruction with bile-stained vomiting secondary to intussusception. Some patients can present with bleeding due to ulceration of the polyp. 5 Our patient was asymptomatic except for microcytic anaemia. This is likely due to chronic blood loss because of ulceration of the tumour.
CT scan of the abdomen is the investigation of choice in diagnosing intussusception with a sensitivity of 50%–100%. If the polyp is large, it can be identified as a lead point. However, in most cases of intussusception in adults, no lead point is identified. 9 Endoscopic ultrasound is of diagnostic value in IFPs. The most common ultrasound pattern is that of a hypoechogenic, homogeneous, non-encapsulated lesion with poorly defined margins located in the second and/or third echo layer of the gastrointestinal wall. Endoscopic ultrasound (EUS) is also of value in evaluating the vascularity of the tumour. 2
The definite diagnosis is based on histopathological analysis and immunocytochemistry. IFP need to be differentiated from GIST. Unlike GIST, IFP shows strong positivity for CD34 and negativity for CD119. 10 This differentiation is essential as GIST requires adjuvant therapy following excision of the tumour.
The treatment of IFPs depends on the size and location of the tumour. Endoscopic polypectomy can be carried out for small accessible tumours. Larger tumours though endoscopically accessible will require surgical excision as the remnant can act as a lead point for intussusception. Our patient underwent small bowel resection with primary anastomosis. There has been no recurrence of the tumour reported in the literature. Hence, following the removal of the IFP, no further adjuvant therapy is required.
Conclusion
The primary ‘takeaway’ lesson of this case report is to identify IFP from GIST since their management differs considerably.
Footnotes
Acknowledgements
We thank all the authors who contributed equally to the management of this patient and the writing of this case report. We would also like to thank all the medical and non-medical personnel who contributed to the day-to-day management of this case. We are grateful to our reviewers for their guidance and advice to help us go accordingly with the publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymised information to be published in this article.