
Abstract
Antenatal Bartter syndrome is a rare condition that affects approximately 1.2 individuals per million. It is caused by renal tubular dysfunction that impairs the reabsorption of sodium and chloride. This results in various symptoms such as polyuria, vomiting, dehydration, and failure to thrive. Because of its low prevalence, diagnosing this disorder can be challenging for medical professionals. In this report, we describe a rare case of a 3-month-old female infant who had symptoms of Bartter syndrome, such as severe hypotension, facial flattening, cough, and seizures. She also had the typical features of the condition, except for prematurity and hypercalciuria, which were not present. In this case, we highlight the importance of regular follow-ups and monitoring of patients with dehydration and electrolyte imbalances, as these can lead to complications in Bartter syndrome. Early intervention and close monitoring can enhance patient outcomes and avoid complications.
Background
Bartter syndrome is a genetic disorder caused by mutations in genes that regulate the synthesis or function of sodium chloride transporters. 1 These transporters are responsible for sodium chloride reabsorption in the kidneys. When the activity of these transporters is reduced due to these mutations, it leads to a slight decrease in the blood volume. This, in turn, activates the renin–angiotensin–aldosterone system. 2 The syndrome is classified into five types based on specific mutations and clinical presentations. 3 Types I, II, and IV are present during fetal and newborn periods and are known as antenatal Bartter syndrome (aBS). There are several genes associated with aBS, most notably the recently discovered changes in the MAGED2 gene. 4 Infants with aBS exhibit low blood potassium levels and elevated pH levels above 7.45 and require mineral supplements to regulate electrolyte balance. They also experience polyuria, decelerated or arrested physical growth, increased renin concentration in the blood, and renal salt wasting, necessitating lifelong fluid and electrolyte supplementation. 5 In addition, complications such as polyhydramnios and premature labor are likely to occur in infants with aBS. However, many clinical manifestations of aBS resolve completely within the first few months of life. Nonetheless, dehydration and vomiting can complicate this condition. The total incidence of aBS is estimated to be 1.2 per million individuals, and late diagnosis can increase morbidity and mortality rates. 6 The objective of this study was to document a clinical case of a 3-month-old female infant diagnosed with Bartter syndrome.
Case presentation
A 3-month-old female infant, first child, normal birth at 40 weeks, weight birth 3500 g, with no pregnancy complications. Because of her complication-free pregnancy, the mother never had an amniotic fluids study done before. The infant was admitted to our hospital with a history of vomiting, diarrhea, and failure to thrive since birth. Despite receiving medication for vomiting and artificial milk, the baby’s symptoms persisted and there was no weight gain. Clinical examination revealed signs of dehydration, including sunken cheeks, coughing, and abnormal lung sounds. The infant’s vital signs were stable, except for low blood pressure, which was indicated by a reading of 8.5/45 mmHg, outside the normal range of 70–40/110–60. Laboratory findings from the complete blood count showed a normal hemoglobin level (11 g/dL), decreased white blood cell (WBC) at 1200 C/μL, and normal neutrophil (44%) and lymphocyte (47%) counts. However, the platelet count was elevated at 1220 × 109/L, exceeding the normal range (150–450) × 109/L). The C-reactive protein (CRP) test result was negative, but the reticulocyte count was significantly elevated at 23%, suggesting an increased demand for oxygen-carrying capacity. The levels of sodium were decreased to 124 mmol/L, potassium was 2.5 mmol/L, calcium was within the normal range at 2.4 mmol/L, and chloride levels were notably low at 82 mmol/L. The alanine transaminase (ALT) level was elevated at 24 IU/L, and the creatinine level was increased to 0.5 mg/dL, indicating potential renal involvement. Blood gases showed an alkaline state with a pH of 7.60 and a reduction in bicarbonate HCO3 = 27 mEq/L. Urinalysis revealed the presence of WBC (13–18/μL or HPF) and red blood cells (RBC:46/μL or HPF), whereas stool analysis was normal. Studies by ultrasound of kidney, liver, spleen, and pancreas were within normal limits.
Further investigations were conducted to confirm the diagnosis of Bartter syndrome. The patient was prescribed aspirin to reduce elevated platelet levels, nonsteroidal anti-inflammatory drugs to reduce urine production and fluid loss, and electrolyte supplementation including potassium chloride. A high-salt diet was prescribed to increase sodium intake and prevent dehydration. The patient was treated for symptoms associated with Bartter syndrome, including dehydration, electrolyte imbalances, and urinary output management. The patient was followed up for 3 months after initiating the treatment. The treatment was effective in the first month, with a gradual decrease in symptom intensity. This allowed us to stop the drug therapy and maintain the observation until the third month post-treatment onset. We detected no negative reactions or symptom recurrence after the first month (Table 1).
Laboratory tests.
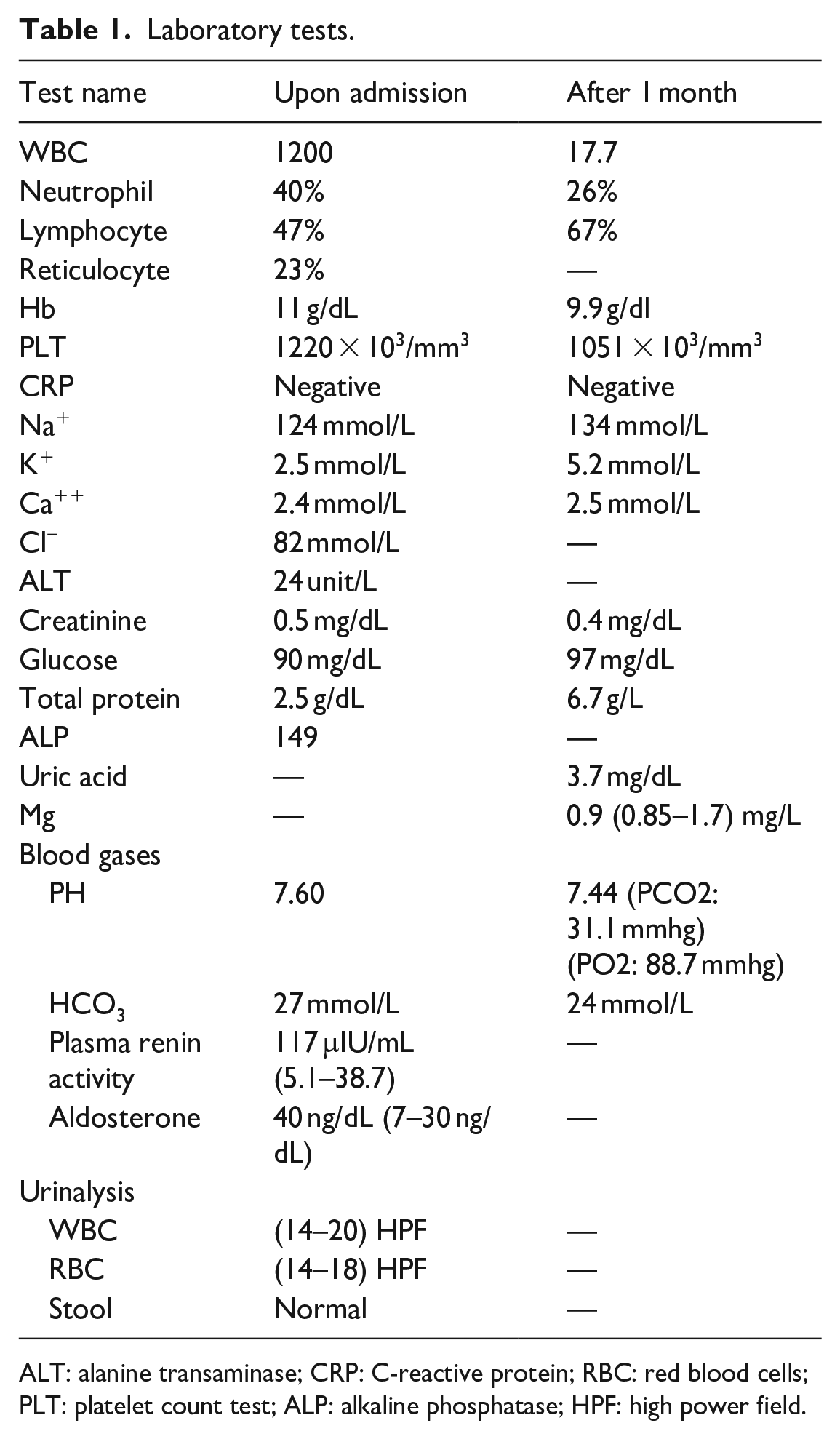
ALT: alanine transaminase; CRP: C-reactive protein; RBC: red blood cells; PLT: platelet count test; ALP: alkaline phosphatase; HPF: high power field.
Discussion
Bartter syndrome is a rare genetic disorder that affects the renal tubules and causes failure of NaCl transporters. It was first described by Frederick Bartter in 1962 and is now named after him. Approximately 1.2 million people are affected by this condition. 6
Bartter syndrome has been classified into two types: prenatal Bartter syndrome and classic Bartter syndrome. The most common characteristic of Bartter syndrome before birth is polyhydramnios, which is a rare genetic disease in the literature and medical reviews. Typical symptoms of this syndrome include polyuria, vomiting, dehydration, and failure to thrive. Bartter syndrome may be confused with other diseases in differential diagnoses, such as metabolic kidney disease, immunodeficiency, lactose intolerance, urinary tract infections, and Gitelmann syndrome. In our case, the diagnosis was made based on laboratory results only because the genetic study was not conducted due to its unavailability in Syria, as the 3-month-old infant showed symptoms of severe hypotension, metabolic alkalosis, hypokalemia, hyperreninemia, hyponatremia, and normal calcium levels. These symptoms are typical of Bartter syndrome and are consistent with previous cases, except for the imbalance in calcium levels, which is a distinguishing feature of Bartter syndrome, in addition to the severe drop in blood pressure, which may have worsened due to dehydration or perhaps the use of anti-vomiting medications at the beginning. In a 2021 study, elevated calcium levels were reported in a Chinese infant, 5 whereas 13 male infants from seven different families were reported in 2016 to present with hypercalciuria along with other symptoms. 7 They were all born prematurely, which is inconsistent with our case, in which the female infant was born after 40 weeks of gestation. This may be related to the sex of the infant, as most previous studies involved premature males.
The pathogenic mechanism of this syndrome is caused by a defect in the reabsorption of sodium chloride in the ascending section of the loop of Henle, which directly results from mutations in the genes. For many years, Bartter syndrome was classified into only four types (from I to IV), with the SLC12A1 gene responsible for type I, the KCNJ1 gene responsible for type II, the CLCNKB gene responsible for type III, while BSND, CLCNKA, and CLCNKB are responsible for type IV.
The first three types exhibit prematurity and failure to thrive as their two most prominent symptoms, while the fourth type is characterized by sensorineural hearing loss in the inner ear with milder symptoms than the first three types. 8 In 2016, Legman et al. added a new fifth type of aBS caused by a mutation in MAGED2 (the skin cancer-associated antigen gene), which is mainly responsible for polyhydramnios and located on the X chromosome at site XP11.2. 9 A recent study by Mingsheng Ma et al. found a new variant of the MAGED2 gene (C.1598C > T, P.Ala533Val) in exon 12. 5 To our knowledge, no previous cases of Bartter syndrome associated with the absence of subcutaneous tissue in cheeks have been reported. Further studies on MAGED2 and its expression are required, as one study found that it can lead to skin cancer. 5 It is possible that the absence of subcutaneous tissue in our case is the first manifestation of skin cancer in the future. Returning to Gitelman syndrome, which is similar to Bartter syndrome, the marking points were clarified for the first time in a study conducted in 2015, in which it was demonstrated that aBS appears in the prenatal period or infants, while the third type of Bartter syndrome appears in infancy and Gitelman syndrome in late childhood or adulthood, so age was considered an important criterion at diagnosis but not sufficient to differentiate between Bartter type 3 and Gitelman syndrome due to the similarity of symptoms to a large extent, and accordingly our diagnosis was confirmed 10 (Table 2).
Comparison of the patterns of Bartter syndrome with Gitelman syndrome.

Until now, there have been no clear treatments for this syndrome due to its rarity 11 ; in our case, the treatment focused mainly on correcting dehydration, electrolyte disturbances, and improving urinary output. However, more accurate studies are needed to fully understand this disease and monitor its progression, especially in developing countries where pregnant women need to be aware of their symptoms during pregnancy. Finally, in light of our data and due to the lack of a genetic study to determine which subtype of Bartter syndrome is responsible for our condition, we believe that a mutation in MAGED2 is responsible for several reasons: The symptoms appeared in early childhood, transient, and be associated with the skin and its cancers and this raised our doubts about the absence of subcutaneous tissue in our case.
Conclusion
This case report underscores the importance of early recognition and appropriate management of Bartter syndrome in infants, as it highlights the clinical presentation, diagnosis, and treatment of this rare genetic condition in a 3-month-old female infant. Continuous follow-up and monitoring are crucial to ensure the well-being of patients with electrolyte imbalances and dehydration, as they can lead to complications associated with Bartter syndrome. Timely intervention and close monitoring are necessary to improve patient outcomes and prevent complications.
Footnotes
Acknowledgements
Not applicable.
Authors’ contributions
H.H., J.A., M.A.N., and A.A. have participated in writing the manuscript. H.H. and J.A. reviewed the literature. All authors critically and linguistically revised the manuscript. H.H. and N.A. contributed to the revision of the manuscript. H.H. and J.A. prepared and revised the final manuscript. N.A. supervised the conduct of the study. All authors read and approved the final manuscript.
Availability of data and materials
Not applicable.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval to report this case was obtained from the Faculty of Medicine at the University of Kalamoon with a serial number (6789/23).
Informed consent
Written informed consent was obtained from a legally authorized representative for anonymized patient information to be published in this article.