
Abstract
Pseudomembranous conjunctivitis, caused by inflammation of the conjunctiva, is characterized by conjunctival injection, mucopurulent discharge, and formation of a thin membrane overlying the conjunctiva. This is often caused by a viral or bacterial infection. This case report discusses pseudomembranous conjunctivitis from Escherichia coli in a newborn infant which, to our knowledge, has not been reported in relevant literature. This infection was likely transmitted perinatally given that the mother of the infant had blood cultures growing E. coli with the same susceptibilities as the newborn. In addition, we discuss relevant literature on the subject including etiologies, management, and complications of pseudomembranous conjunctivitis.
Introduction
Neonatal conjunctivitis (also known as ophthalmia neonatorum) is one of the most common infections seen in the newborn period, often occurring in the first 4 weeks of life. Its incidence has significantly declined as a result of universal prophylaxis over the past decades.1,2 Pseudomembranous conjunctivitis is caused by inflammation of the conjunctiva leading to conjunctival injection, mucopurulent discharge, and formation of a thin membrane overlying the conjunctiva. It is often secondary to an infection from either a bacterial or viral pathogen. It may also develop as a result of foreign body irritation to the conjunctivae from allergens and toxins. Other etiologies include medication reactions, such as those seen in patients with Steven-Johnson syndrome. Pseudomembranous conjunctivitis has also been seen in genetic disorders. For example, ligneous conjunctivitis is thought to have an autosomal recessive inheritance pattern. 3 Pseudomembranous conjunctivitis is characterized by the absence of vascular supply, differentiating it from membranous conjunctivitis. As a result, pseudomembranous conjunctivitis does not bleed when removed. 4 Here, we report a case of pseudomembranous conjunctivitis from Escherichia coli which, to our knowledge, has not been reported in relevant literature.
Case report
A term male neonate was born by normal spontaneous vaginal delivery to a mom with normal prenatal screens. Membranes spontaneously ruptured for 13 h with clear fluid. Pregnancy was notable for gestational diabetes, hydronephrosis with stent placement, and multiple urinary tract infections secondary to Klebsiella sp. Infant was transferred to the neonatal intensive care unit (ICU) after delivery due to temperature instability and respiratory distress with increasing supplemental oxygen requirement. After delivery, he appeared dusky with oxygen saturations of 80%. He was placed on 2 L of nasal cannula at 21% FiO2, but he continued to exhibit signs of respiratory distress including grunting and tachypnea. His FiO2 was increased to 40% and he subsequently improved. His serum glucose, blood gas, complete blood count, renal function panel, and C-reactive protein were unremarkable. Chest radiograph showed mild diffuse ground glass opacities without focal consolidation. Blood culture was drawn. He was empirically started on ampicillin, gentamicin, and ceftazidime. His NICU course was complicated by respiratory failure on day 2 of admission, ultimately requiring intubation. Also around the same time, he developed copious purulent drainage from his left eye (Figure 1). Ophthalmologic examination revealed diffuse fleshy red pseudomembrane coating the bulbar and tarsal conjunctiva of the left eye with normal findings of the right eye. The pseudomembrane coating was debrided yielding purulent and serosanginous drainage. Bacterial culture from the left eye grew pan-sensitive E. coli (Table 1). The speciation of the species was performed by matrix-assisted laser desorption/ionization-time of flight (MALDI-TOF), and the susceptibility testing was performed using automated broth microdilution. Although the minimal inhibitory concentrations (MICs) of E. coli isolates from infant and mother were not identical, this could be due to lab-specific differences in how MICs are determined, as the isolates were worked up in different microbiology labs. The specific strain of E. coli was not determined due to the standard processes of our hospital lab. Viral culture was also sent which did not demonstrate any growth. His blood and urine cultures did not demonstrate any growth. Cerebral spinal fluid studies were collected in the setting of early-onset neonatal sepsis and were also negative. Mom’s placental pathology did not show any abnormal findings. The patient’s mother was hospitalized shortly after delivery for urosepsis secondary to E. coli. Sensitivities of E. coli recovered from the mother’s urine culture mirrored that of the infant’s E. coli isolated from his ocular drainage (Table 1). By day 3 of life, the infant was successfully extubated to nasal cannula. Repeat ophthalmologic examinations showed significant clinical improvement after 24–48 h of intravenous and topical antimicrobials. He completed a full 14-day course of antimicrobial therapy with ampicillin for the left eye pseudomembranous conjunctivitis, pneumonia, and sepsis, all presumed to be from the same E. coli isolated from the affected eye. In addition, he completed 11 days of moxifloxacin eye drops. The infant was weaned to room air on day of life 5 and was ready to be discharged home when the antibiotic course was complete. His follow-up eye examination 1 week after discharge was normal, showing complete resolution of conjunctivitis.

Erythematous pseudomembrane coating the bulbar and tarsal conjunctiva of the left eye.
E. coli sensitivities.
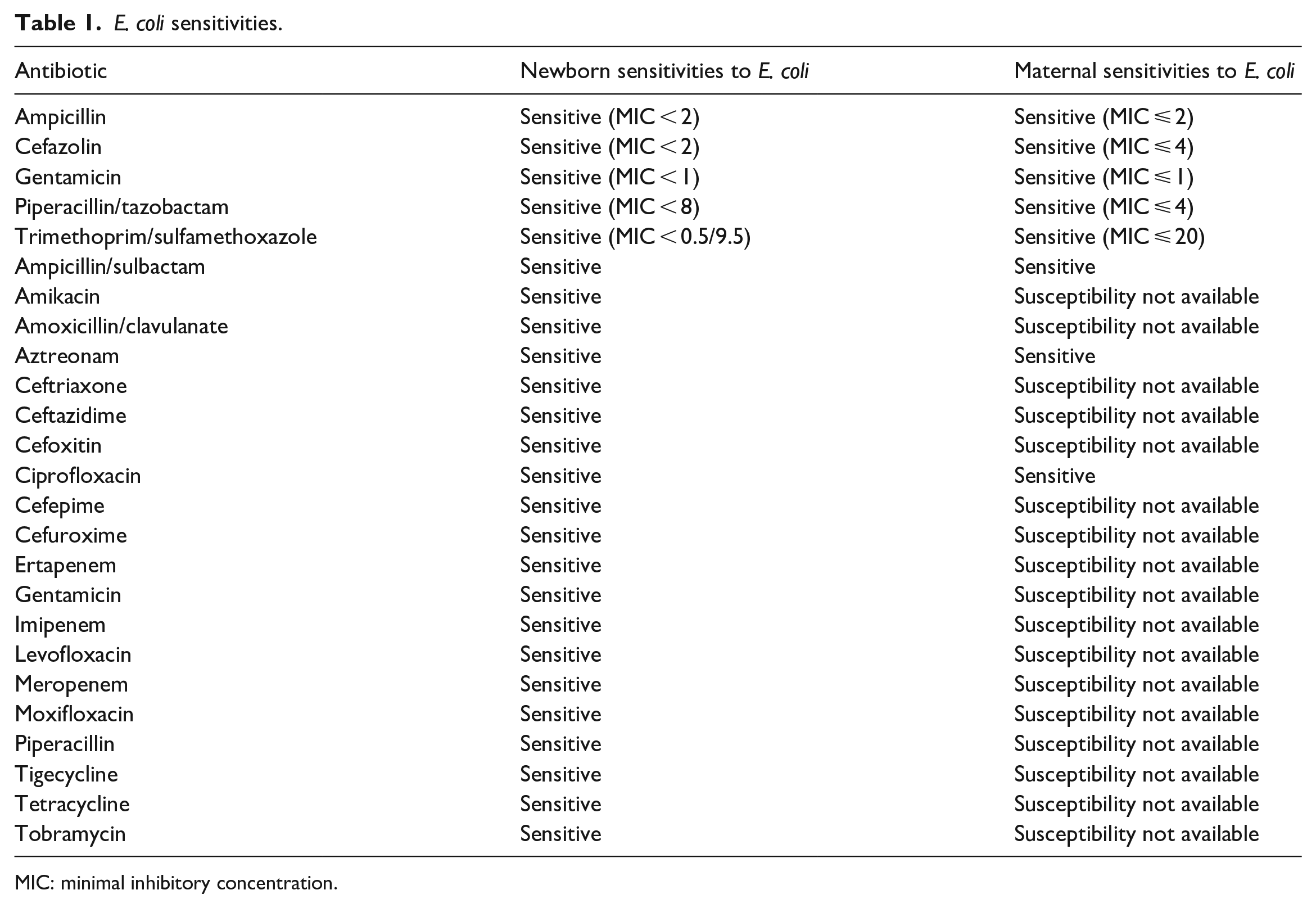
MIC: minimal inhibitory concentration.
Discussion
The incidence of ophthalmia neonatorum in the United States has continued to decline due to universal prophylaxis. However, its overall incidence of 1%–2% has remained of clinical relevance.1,2,5 Pseudomembranous conjunctivitis is an inflammatory condition that is characterized by muco-purulence and pseudomembrane formation, most commonly described in the setting of infection. The organisms that have been linked to pseudomembranous conjunctivitis include Streptococcus, Staphylococcus, Klebsiella, Chlamydia, Corynebacterium, and adenovirus. 3 It is postulated that the organisms that are involved in this form of conjunctivitis are part of the normal flora of the conjunctiva. Risk factors for development of conjunctivitis in neonates include decreased tear production, premature rupture of membranes, prolonged delivery, prematurity, inconsistent prenatal care, maternal infection (urinary tract infections, sexually transmitted infections), and history of midwife interference. The infant in our case was at higher risk given ruptured membranes for 13 h and maternal urinary tract infection leading to urosepsis.
E. coli has been reported to be the cause of about 17% of Gram-negative conjunctivitis among low birth weight and low gestational premature infants in a retrospective study. 7 There are only two case reports of E. coli conjunctivitis reported in term babies.2,8 Both of these cases did not report pseudomembrane formation. To our knowledge, pseudomembranous conjunctivitis secondary to E. coli infection has not been reported in relevant literature. In our patient, the infection most likely occurred perinatally given that the mother of this neonate was hospitalized with urosepsis secondary to E. coli.
Treatment of infectious pseudomembranous conjunctivitis involves removal of the pseudomembrane and targeted antimicrobials to treat the underlying infectious etiology. Following treatment, recurrence of the pseudomembrane is not uncommon. Many cases have required repeated removal of the pseudomembrane followed by a course of topical steroids to relieve the inflammation. 3 In an epidemiologic study of pseudomembranous viral conjunctivitis among adults, 38.4% of patients were found to incur one of the following complications: subepithelial infiltrates, corneal abrasions, filamentary keratitis, and subtarsal fibrosis. 4 It is, however, hard to extrapolate from this study whether these complications occur in the neonatal population. In a reported case of an 8-year-old patient with pseudomembranous conjunctivitis from Streptococcus pyogenes, full resolution of the infection and inflammation were observed after removal of the pseudomembrane and receipt of antibiotics. 3 Our patient was treated with surgical debdridement of the pseudomembrane along with culture-guided systemic antibiotics and a course of a topical antibiotic with complete resolution of symptoms.
Conclusion
Neonatal conjunctivitis is not uncommon; however, pseudomembranous conjunctivitis in a newborn secondary to E. coli is unusual. Early diagnosis and treatment with culture-guided systemic and topical antibiotics is required for resolution of symptoms. Although unusual, E. coli should be considered as the causative agent when evaluating and treating pseudomembranous conjunctivitis. While there are specific guidelines used to treat conjunctivitis secondary to Chlamydia trachomatis and Neisseria gonorrhoeae, treatment of conjunctivitis secondary to other bacterial organisms is not as well established. If left untreated, this infection can result in significant complications including ulceration of the cornea and blindness.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from a legally authorized representative for anonymized patient information to be published in this article. Written informed consent was obtained from a legally authorized representative for publication of images in this case report.