
Abstract
Choledochotomy and choledochoduodenostomy were commonly used technique in the early twentieth century to extract bile duct stones. Endoscopic retrograde cholangiopancreatography and sphincterotomy revolutionised the scenario and is currently the preferred first-line option for managing choledocholithiasis. However, in certain circumstances, where endoscopic retrograde cholangiopancreatography fails, choledochotomy and choledochoduodenostomy are the only available options. We present the case of an 86-year-old female with a background of multiple previous presentations with biliary sepsis and ascending cholangitis requiring multiple endoscopic retrograde cholangiopancreatographies that failed to remove all stones in the common bile duct. She underwent a laparoscopic choledochotomy and choledochoduodenostomy that successfully resolved her common bile duct obstruction. Laparoscopic choledochotomy and choledochoduodenostomy reduce the length of hospital stay and help to minimise complications associated with open surgery.
Introduction
Endoscopic retrograde cholangiopancreatography (ERCP) and sphincterotomy is the current gold standard for the management of choledocholithiasis.1,2 However, choledochotomy (CD) and choledochoduodenostomy (CCD) is the only fallback option if ERCP fails. Laparoscopic CD and CCD procedure (in experienced hands) is the preferred intervention compared to open procedure. 3 With the increasing availability and improvement of advanced endoscopic equipment, CCD (open/laparoscopic) is a rarely performed procedure nowadays. 4 We present a case where laparoscopic CD and CCD was utilised following multiple failed ERCP attempts for the management of a large recurrent complicated choledochal obstruction. 5 Though the particular procedure is performed rarely these days, the procedural video will augment the existing literature and aid surgeons globally for this potentially life-saving procedure.
Case presentation
An 86-year-old lady of Chinese background presented to our emergency department with fevers and upper abdominal pain. She had multiple previous presentations with biliary sepsis and ascending cholangitis. Computed tomography (CT) and ultrasound scan (USS) imaging suggested extensive intra- and extrahepatic duct dilatation with choledocholithiasis and cholelithiasis. The common bile duct (CBD) measured up to 17.6 mm. Previous ERCP had failed to relieve the obstruction completely due the size of the stone.
The patient had non-ischemic cardiomyopathy with moderate to severe left ventricular (LV) dysfunction. She was earlier on aspirin that had been replaced by clopidogrel 1 year back due to severe symptomatic erosive gastritis. During this presentation, given her age, history of dyslipidaemia and cardiac disease, cardiac biomarkers were added to the regular blood tests. She had a high level of troponin without any electrocardiography (ECG) changes. She was assessed by the cardiology team suggesting type 2 myocardial infarction. This led to her receiving a high dose of enoxaparin and continuing of her clopidogrel.
Her cholangitis warranted urgent ERCP. Subsequently, ERCP demonstrated multiple stones (at least 6) within the CBD with the largest being > 1.5 cm (Figure 2) in its largest dimension. The major duodenal papilla was located in a diverticulum with a bezoar limiting its access severely (Figure 1).

Endoscopic retrograde cholangiopancreatography (ERCP) images.
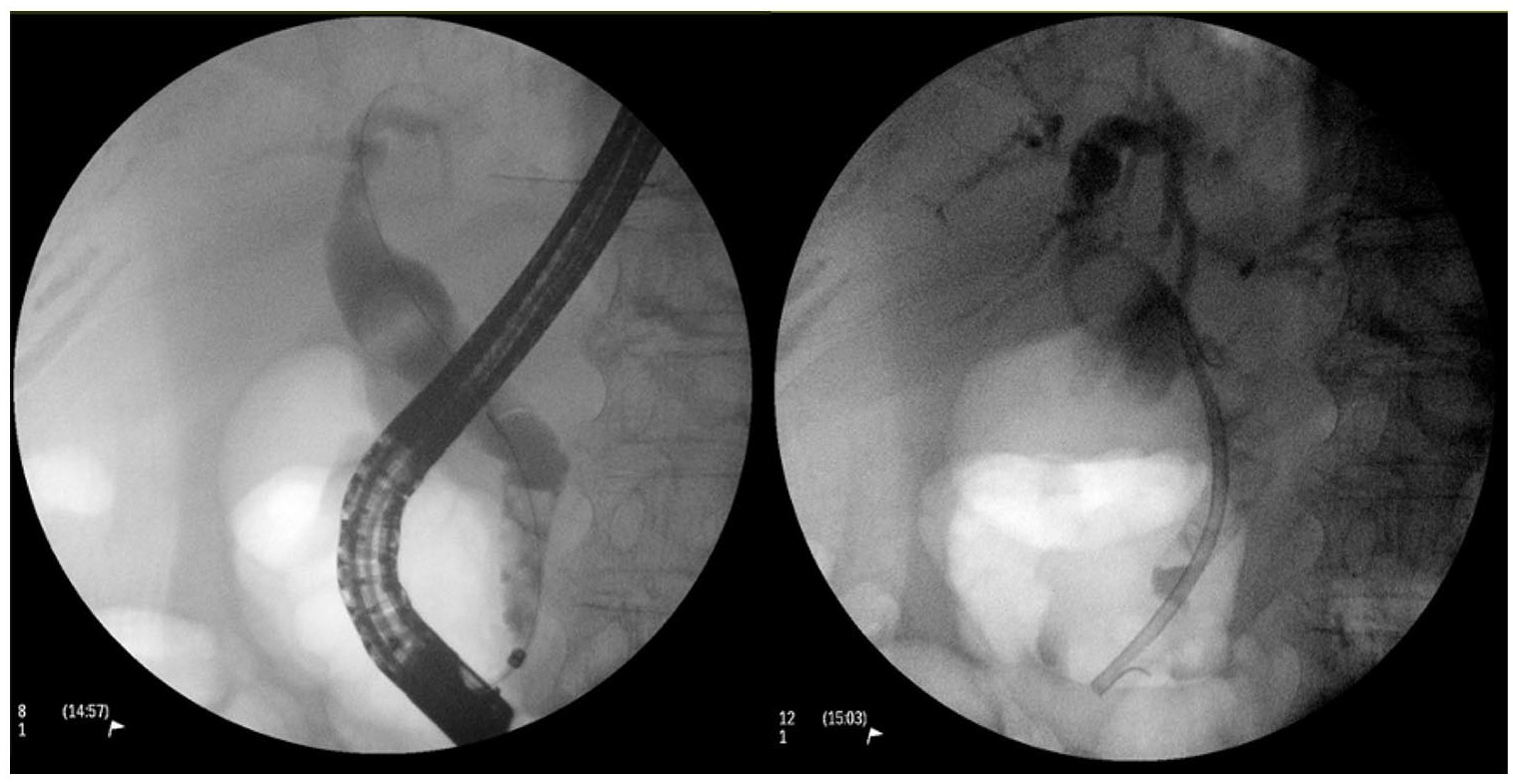
Left: Cholangiogram showing multiple filling defects and dilated proximal common bile duct. Right: Cholangiogram showing position of plastic stent.
With the main calculi in question being > 1.5 cm in its largest dimension and failed endoscopic attempts at retrieval, including failed papillary dilatation, during ERCP, the decision was made for a CBD exploration rather than attempting to retrieve such a big calculi. With this decision, sphincterotomy was not performed as it would not have changed management. Thus, a 7 cm 10 Fr plastic stent was placed as a temporary measure. There was a stone beyond the reach of the stent as noted on the cholangiogram.
Following resolution of the acute septic episode, the patient underwent an elective laparoscopic CBD exploration, CCD and cholecystectomy. The patient did not undergo cholecystectomy earlier because her obstructive jaundice had resolved. Moreover, considering her age and other comorbidities, it was the patient’s preference to not have any major procedures unless it was life-saving. However, following the last episode, she changed her mind. The patient had her ERCP within the same admission where she presented with biliary sepsis and subsequently underwent the laparoscopic CBD exploration, CCD and cholecystectomy 4 months after the ERCP. During the laparoscopic procedure, her clopidogrel was stopped 5 days prior to the procedure. It was recommenced post-procedure.
The patient’s past medical history comprises hypertension, hyperlipidaemia, type 2 diabetes mellitus, Alzheimer’s disease and cardiomyopathy. She had not undergone any previous laparoscopic or open surgical procedures.
Her regular medications included bisoprolol (beta blocker), simvastatin (statin), metformin, donepezil, furosemide and clopidogrel. During her presentation, the patient was treated with intravenous antibiotics, namely, piperacillin–tazobactam, which was subsequently stepped down to amoxicillin–clavulanate in line with clinical improvement and local guidelines.
Prior to the laparoscopic CBD exploration, CCD and cholecystectomy, she was icteric with a total bilirubin of 107 µmol/L. Other liver function tests were also deranged, gamma-glutamyl transferase (GGT) 325 U/L, alkaline phosphatase (ALP) 582 U/L, alanine aminotransferase (ALT) 11 U/L, aspartate aminotransferase (AST) 67 U/L. Her inflammatory markers were elevated with a white cell count of 14.1 × 109/L and C-reactive protein (CRP) of 74 mg/L. Following the laparoscopic CBD exploration, CCD and cholecystectomy, there was marked improvement in her liver function tests with a total bilirubin 6 µmol/L, GGT 32 U/L, ALP 77 U/L, ALT 6 U/L and AST 15 U/L. At the time of discharge, her inflammatory markers normalised with a white cell count of 8.1 × 109/L.
Standard laparoscopic port insertion (American style) for laparoscopic cholecystectomy was used for the procedure. As we are more familiar with the American style in our daily practice, we followed that in our procedure. A longitudinal incision was made on the dilated CBD with diathermy. One large stone was removed and multiple smaller calculi were flushed out. A Fogarty’s catheter was used to dilate the cystic and common hepatic duct. We did not use a choledochoscope as it would not have changed the management. Balloon sweeping was done and the patency of the duct with free flowing bile was established. The previous stent was left in situ. Laparoscopic ultrasound confirmed no further obstruction in the biliary tract. A side-to-side CCD was then performed with the first part of the duodenum using 3-0 Vicryl-lock absorbable suture followed by a cholecystectomy. A 10 Fr Jackson-Pratt drain was placed in the gallbladder fossa. There were no intra- or post-operative complications and the patient was discharged home safely 5 days after her hospital stay. ERCP was repeated 8 weeks later and the previous stent was removed (Figure 2). She did not have any residual obstruction during the follow up 3 months later – confirmed by normal liver function tests and ultrasound imaging.
Discussion
First described in 1888, CCD was a commonly used technique in the early twentieth century to extract bile duct stones. With the emergence of ERCP and sphincterotomy, the indications for CCD have narrowed. Presently, common indications include endoscopic failure to clear distal CBD obstruction due to strictures or altered biliary anatomy, large impacted CBD stone, multiple stones, intrahepatic stones and recurrent stones. 6
CCD can be performed either open or laparoscopically using a side-to-side or end-to-side anastomosis. Compared to open procedure, laparoscopic bile duct exploration is associated with less blood loss, post-operative pain and morbidity, shorter hospital stay as well as shorter recovery time.7,8 A study by Grubnik et al. 9 showed that the post-operative morbidity in open CBD exploration was higher at 12.7% compared to 6.5% in the laparoscopic group. Another study utilising the American College of Surgeons National Surgical Quality Improvement Program database to compare open and minimally invasive bile duct exploration involving 2635 patients showed that the open procedure was associated with a statistically significant higher rate in mortality, composite morbidity, bleeding, return to the operation room and readmission. 10 Laparoscopic CCD has also been shown to be a safe and effective procedure especially for patients with advanced age and multiple comorbidities.11,12
Side-to-side CCD is often associated with ascending cholangitis, sump syndrome and alkaline reflux gastritis. 13 Follow-up results in a case series involving 70 patients who underwent side-to-side CCD, it was concluded that it is a safe and effective therapeutic measure and the complications associated with it were not seen very often. 13 In a case series involving 270 patients who underwent CCD, Malik et al. 14 reported that there was none experienced sump syndrome when side-to-side anastomosis was performed. A study of 130 cases of CCD comparing side-to-side and end-to-side anastomosis showed that there was no statistical difference in surgical outcome between the two approaches. 4 This included parameters, such as operative time, blood loss, length of hospital stay and post-operative complications. A study by Srivengadesh et al. 15 involving follow-up of 21 patients who underwent side-to-side anastomosis concluded that it is a safe procedure with good long-term results and infrequent complications. In a 20-year follow-up of 78 patients who underwent end-to-side CCD reported by Funabiki et al., 16 it was reported that there were only five cases of reflux cholangitis with anastomotic stenosis. Similarly, a study by Bosanquet et al., 17 which evaluated 68 patients who underwent CCD under a single surgeon from 1992 to 2009 taking into account post-operative morbidity and mortality, and complications also concluded that it is a safe and effective procedure. It has been reported in the literature that CCD results in a low rate of recurrent cholangitis and long-term biliary drainage.4,5 A study with a mean follow-up of 5.6 years showed that 71.5% of patients who had CCD were asymptomatic and did not experience episodes of cholangitis. 18 While end-to-side hepaticojejunostomies have better long-term outcome with anastomotic stricture, the advantage of CCD is easier access for endoscopic therapies and it remains more suitable for patient with previous extensive abdominal surgeries or shortened small intestine. The overall morbidity after hepaticojejunostomies and CCD was comparable. However, patients with an anastomotic stricture after hepaticojejunostomies could be managed by endoscopic/radiological re-intervention, while all patients with a stricture after CD required surgical re-intervention. Hence, it is important to tailor the choice of procedure according to the patient as each patient is different and might benefit more from one procedure type over the other. 19
With the advancement of technology, there have also been reported cases of robotic CCD.20,21 Current literature available has demonstrated that it is a safe and feasible option. However, it is still in its nascent phase and robotic consoles are not widely available yet and surgeons need to be trained how to tackle the same scenario using laparoscopic or open technique in case robotic technique fails.
Conclusion
Laparoscopic choledochotomy and CCD should be considered in management of CBD obstruction that is not amenable to ERCP. The ability to perform it laparoscopically helps reduce length of hospital stay and avoid other complications associated with open surgery. Although not a commonly performed procedure, it is no doubt an extremely useful surgical procedure in complex CBD stones and this report details the crucial steps involved in the procedure (Video).
Footnotes
Author contributions
A.M. (principal) and S.P.R. (assistant) were the surgeons and conceived the case report. T.S.H.S. and S.S. wrote the first draft. S.S. edited and narrated the supplemental video. All authors participated in the construction and editing of the manuscript and drafts. A.M. and S.P.R. supervised the write up and S.P.R. is the corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.